

Abstract
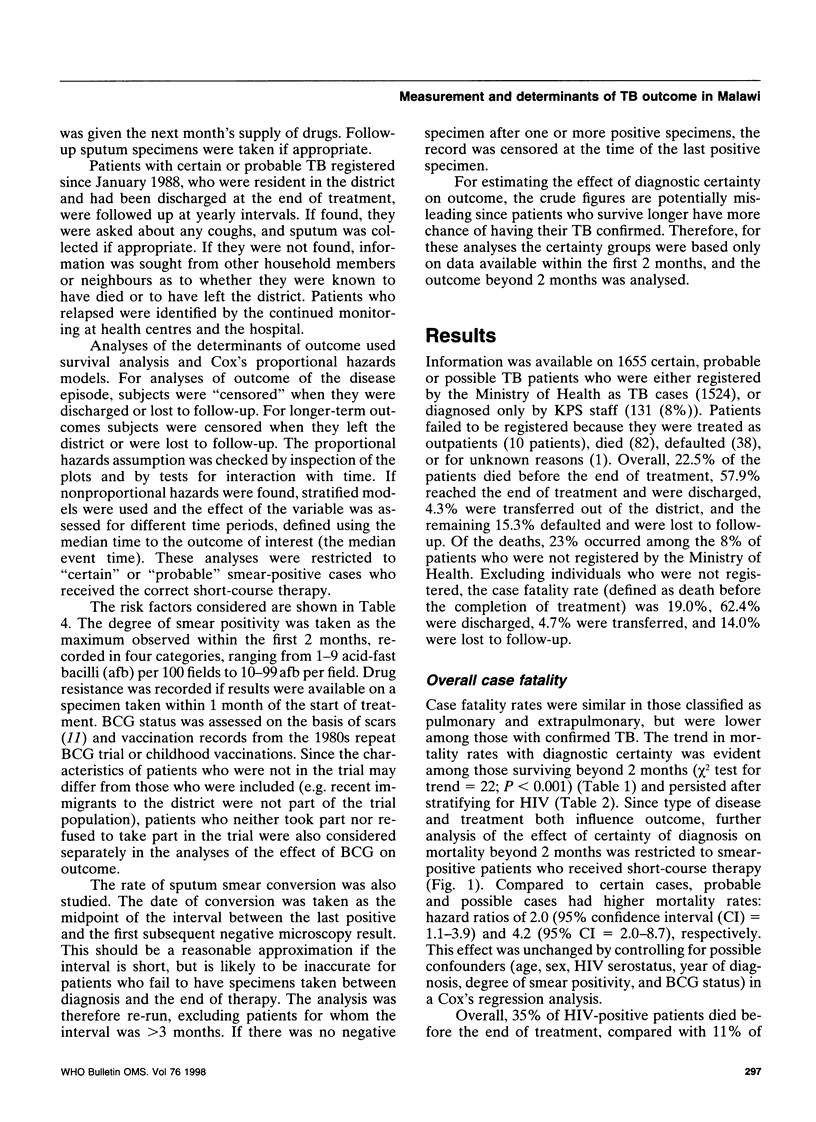
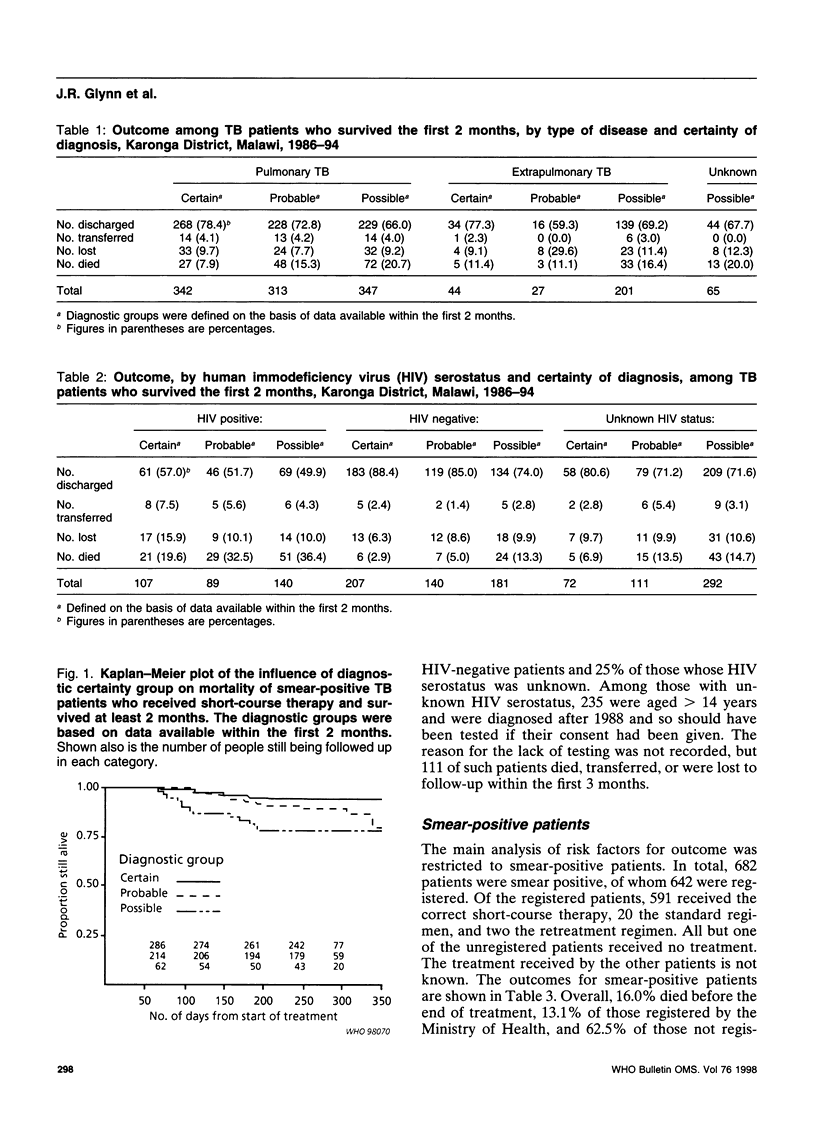
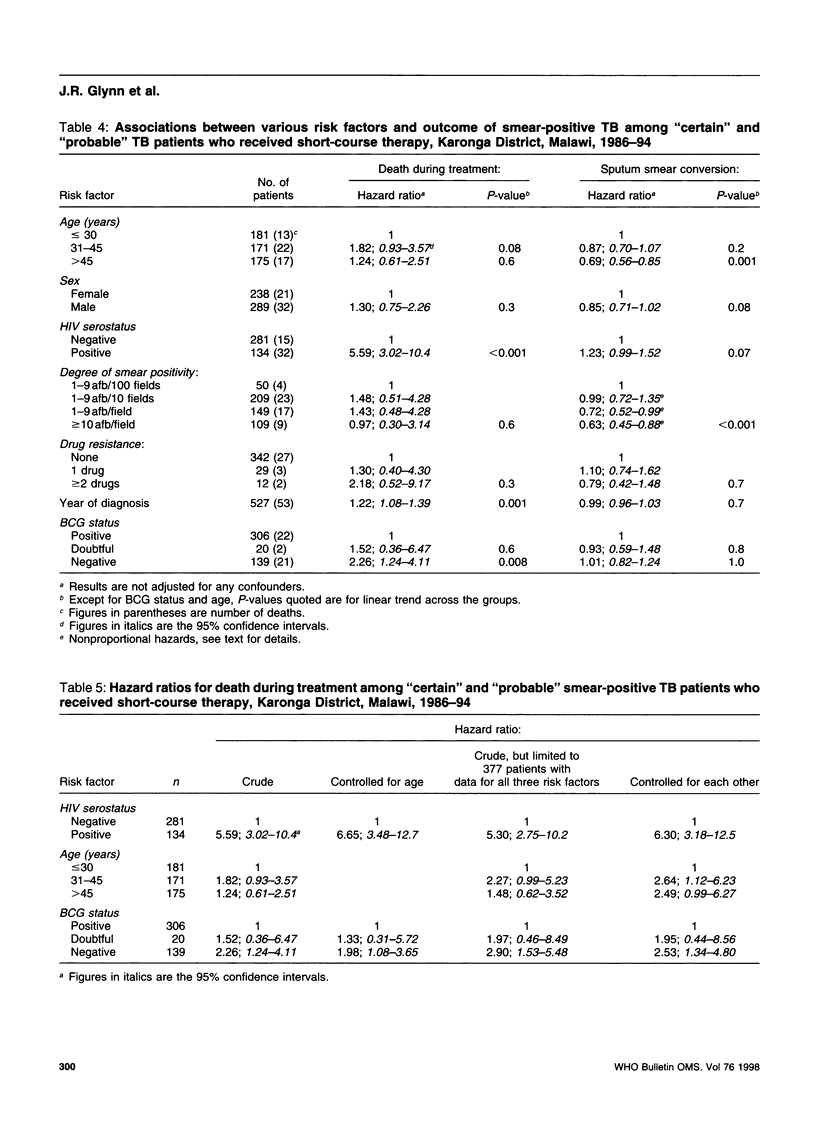
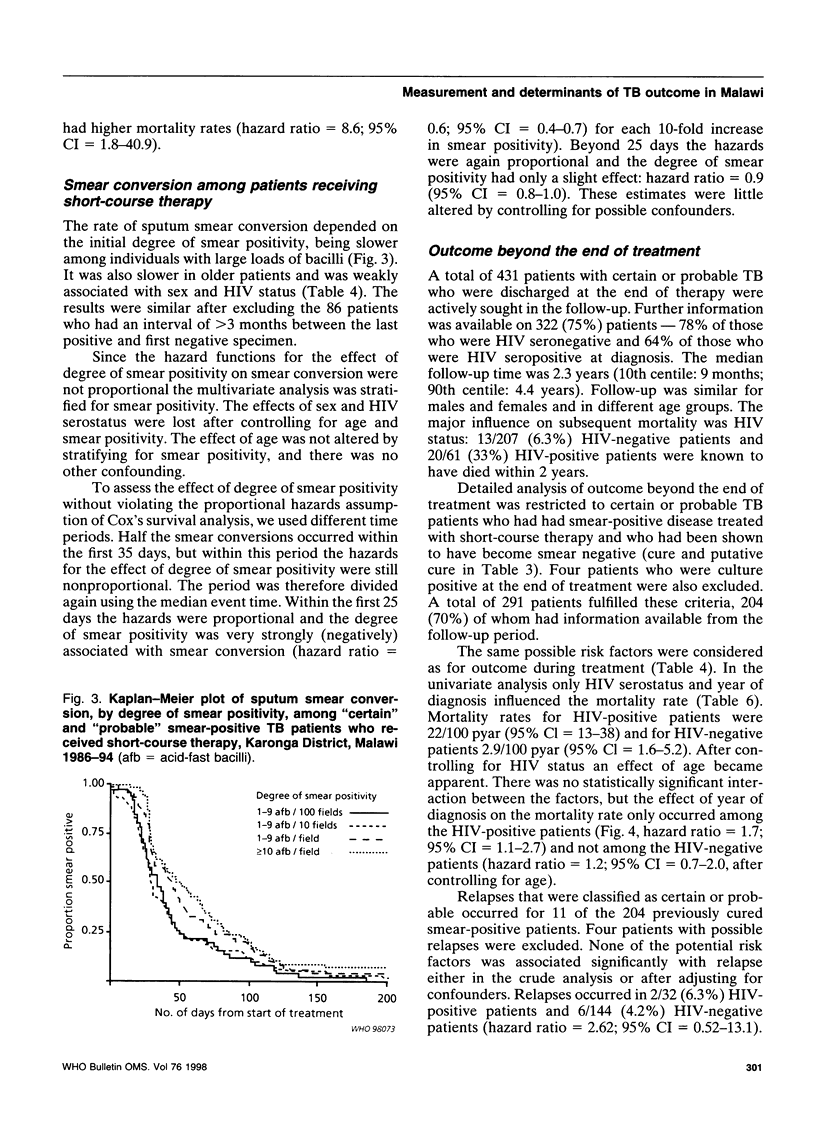
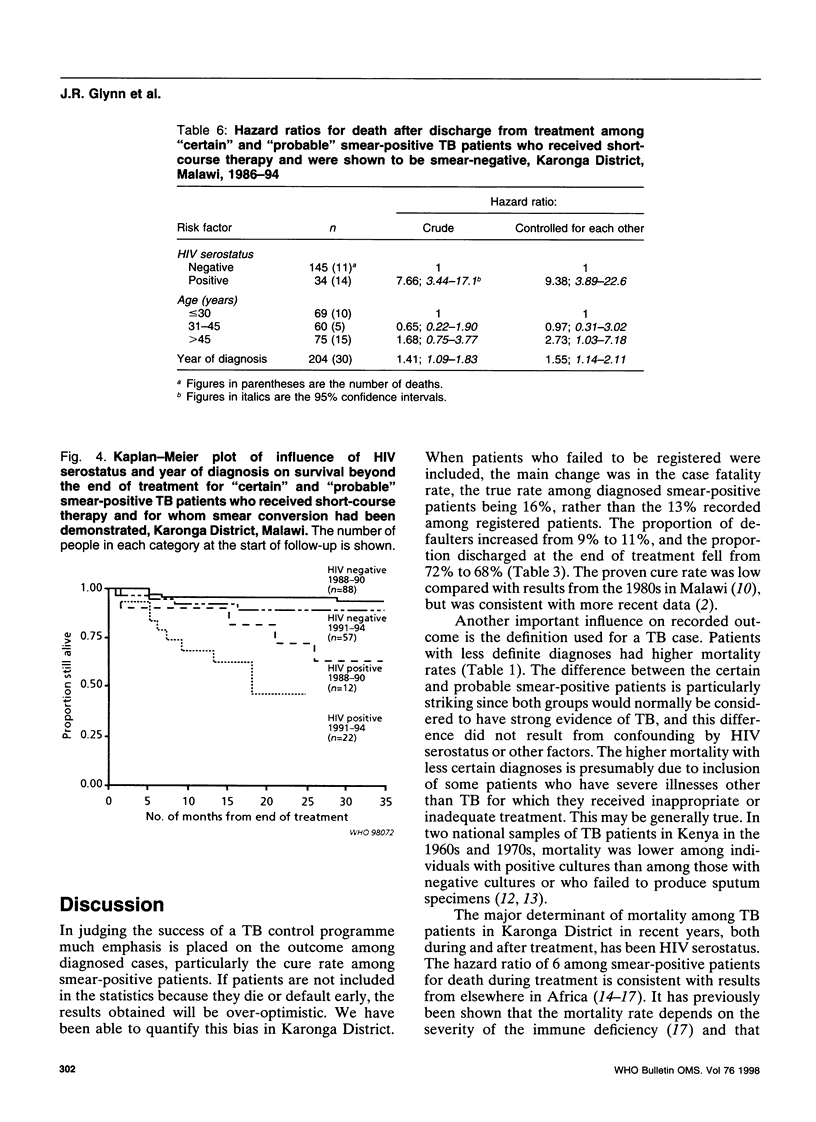
Evaluation of disease outcome is central to the assessment of tuberculosis (TB) control programmes. In the study reported in this article we examined the factors influencing the measurement of outcome, survival rates during and after treatment, smear conversion rates, and relapse rates for patients diagnosed with TB in a rural area of Malawi between 1986 and mid-1994. Patients with less certain diagnoses of TB were more likely to die than those with confirmed TB, both among those who were seropositive and those who were seronegative to human immunodeficiency virus (HIV). The mortality rate among smear-positive patients with a separate culture-positive specimen was half that of patients with no such diagnostic confirmation. Patients not registered by the Ministry of Health had much higher mortality and default rates than did registered patients. Among smear-positive patients, HIV serostatus was the most important influence on mortality both during and after treatment (crude hazard ratios (95% confidence intervals) = 5.6 (3.0-10) and 7.7 (3.4-17), resp.), but HIV serostatus did not influence smear conversion rates. The initial degree of smear positivity influenced smear conversion rates, but not mortality rates. No significant predictors of relapse were identified. Unless considerable care is taken to include all TB patients, and to exclude nontuberculous patients, recorded TB outcome statistics are difficult to interpret and may be misleading. In populations with high rates of HIV infection, TB target cure rates of 85% are unrealistic. When new interventions are assessed it cannot be assumed that factors which influence the smear conversion rate will also influence the mortality rate.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ackah A. N., Coulibaly D., Digbeu H., Diallo K., Vetter K. M., Coulibaly I. M., Greenberg A. E., De Cock K. M. Response to treatment, mortality, and CD4 lymphocyte counts in HIV-infected persons with tuberculosis in Abidjan, Côte d'Ivoire. Lancet. 1995 Mar 11;345(8950):607–610. doi: 10.1016/s0140-6736(95)90519-7. [DOI] [PubMed] [Google Scholar]
- Elliott A. M., Halwiindi B., Hayes R. J., Luo N., Mwinga A. G., Tembo G., Machiels L., Steenbergen G., Pobee J. O., Nunn P. P. The impact of human immunodeficiency virus on response to treatment and recurrence rate in patients treated for tuberculosis: two-year follow-up of a cohort in Lusaka, Zambia. J Trop Med Hyg. 1995 Feb;98(1):9–21. [PubMed] [Google Scholar]
- Fine P. E., Ponnighaus J. M., Maine N. The distribution and implications of BCG scars in northern Malawi. Bull World Health Organ. 1989;67(1):35–42. [PMC free article] [PubMed] [Google Scholar]
- Glynn J. R., Jenkins P. A., Fine P. E., Pönnighaus J. M., Sterne J. A., Mkandwire P. K., Nyasulu S., Bliss L., Warndorff D. K. Patterns of initial and acquired antituberculosis drug resistance in Karonga District, Malawi. Lancet. 1995 Apr 8;345(8954):907–910. doi: 10.1016/s0140-6736(95)90016-0. [DOI] [PubMed] [Google Scholar]
- Hawken M., Nunn P., Gathua S., Brindle R., Godfrey-Faussett P., Githui W., Odhiambo J., Batchelor B., Gilks C., Morris J. Increased recurrence of tuberculosis in HIV-1-infected patients in Kenya. Lancet. 1993 Aug 7;342(8867):332–337. doi: 10.1016/0140-6736(93)91474-z. [DOI] [PubMed] [Google Scholar]
- Kochi A. The global tuberculosis situation and the new control strategy of the World Health Organization. Tubercle. 1991 Mar;72(1):1–6. doi: 10.1016/0041-3879(91)90017-m. [DOI] [PubMed] [Google Scholar]
- Murray C. J., DeJonghe E., Chum H. J., Nyangulu D. S., Salomao A., Styblo K. Cost effectiveness of chemotherapy for pulmonary tuberculosis in three sub-Saharan African countries. Lancet. 1991 Nov 23;338(8778):1305–1308. doi: 10.1016/0140-6736(91)92600-7. [DOI] [PubMed] [Google Scholar]
- Nyangulu D. S. The point of view of a high prevalence country: Malawi. Bull Int Union Tuberc Lung Dis. 1991 Dec;66(4):173–174. [PubMed] [Google Scholar]
- Perriëns J. H., Colebunders R. L., Karahunga C., Willame J. C., Jeugmans J., Kaboto M., Mukadi Y., Pauwels P., Ryder R. W., Prignot J. Increased mortality and tuberculosis treatment failure rate among human immunodeficiency virus (HIV) seropositive compared with HIV seronegative patients with pulmonary tuberculosis treated with "standard" chemotherapy in Kinshasa, Zaire. Am Rev Respir Dis. 1991 Oct;144(4):750–755. doi: 10.1164/ajrccm/144.4.750. [DOI] [PubMed] [Google Scholar]
- Pönnighaus J. M., Fine P. E., Bliss L., Gruer P. J., Kapira-Mwamondwe B., Msosa E., Rees R. J., Clayton D., Pike M. C., Sterne J. A. The Karonga Prevention Trial: a leprosy and tuberculosis vaccine trial in northern Malaŵi. I. Methods of the vaccination phase. Lepr Rev. 1993 Dec;64(4):338–356. doi: 10.5935/0305-7518.19930039. [DOI] [PubMed] [Google Scholar]
- Randomised controlled trial of single BCG, repeated BCG, or combined BCG and killed Mycobacterium leprae vaccine for prevention of leprosy and tuberculosis in Malawi. Karonga Prevention Trial Group. Lancet. 1996 Jul 6;348(9019):17–24. [PubMed] [Google Scholar]
- Results of directly observed short-course chemotherapy in 112,842 Chinese patients with smear-positive tuberculosis. China Tuberculosis Control Collaboration. Lancet. 1996 Feb 10;347(8998):358–362. [PubMed] [Google Scholar]
- Rieder H. L. Sputum smear conversion during directly observed treatment for tuberculosis. Tuber Lung Dis. 1996 Apr;77(2):124–129. doi: 10.1016/s0962-8479(96)90026-x. [DOI] [PubMed] [Google Scholar]
- Sterne J. A., Turner A. C., Fine P. E., Parry J. V., Lucas S. B., Pönnighaus J. M., Mkandwire P. K., Nyasulu S., Warndorff D. K. Testing for antibody to human immunodeficiency virus type 1 in a population in which mycobacterial diseases are endemic. J Infect Dis. 1995 Aug;172(2):543–546. doi: 10.1093/infdis/172.2.543. [DOI] [PubMed] [Google Scholar]