

Abstract
Objective:
To assess hamstrings and quadriceps strength of basketball players ages 11–13 and 15–17 years.
Design and Setting:
This cross-sectional study occurred during the 2000 American Youth Basketball Tour National Tournament. We investigated whether sex- or age-related strength differences existed among study participants.
Subjects:
Forty-one tournament participants (22 girls, 19 boys; 11–13 or 15–17 years old) who reported no history of knee sprain or surgery were recruited.
Measurements:
We used a Cybex II dynamometer to obtain isokinetic concentric peak torques relative to body mass (Nm/kg) at 60°/s for hamstrings and quadriceps bilaterally. From average peak torques, we determined ipsilateral hamstrings:quadriceps and homologous muscle-group ratios.
Results:
Correlations between hamstrings and quadriceps strength measures ranged from 0.78 to 0.97. Players 15–17 years old had greater relative hamstrings and quadriceps strength than 11- to 13-year-old athletes. Age and sex interacted significantly for quadriceps strength. The quadriceps strength of 15- to 17-year-old girls did not differ from that of 11- to 13-year-old girls, whereas 15- to 17-year-old boys had stronger quadriceps than 11- to 13-year-old boys. Boys 15–17 years old had greater quadriceps strength than girls 15–17 years old.
Conclusions:
This study is unique in providing normative data for the hamstrings and quadriceps strength of basketball players 11–13 and 15–17 years old. Age-related strength differences did not occur consistently between the sexes, as girls 11–13 and 15–17 years old had similar relative quadriceps strength.
Keywords: isokinetics, adolescents, injury prevention, quadriceps, hamstrings
Muscle strength is commonly emphasized in preventive and rehabilitative programs for athletes and other physically active people. It is one control factor that influences motor behavior1,2 and therefore potentially affects the risk of injury. Given the frequency of knee injuries in athletes,3–6 many researchers have focused on providing normative data for the knee periarticular muscles.7–9 Athletic trainers and other sports medicine professionals often assess muscle strength at isolated joints with isokinetic testing. Traditionally, athletic trainers have used ipsilateral hamstrings:quadriceps (H:Q) ratios, homologous hamstrings and quadriceps ratios, and normative joint-specific peak-torque data to assess muscular status. Although no consensus exists on age- and sex-appropriate standards for individual muscle-group strength, suggested concentric normative values for H:Q ratios at testing velocities of 60°/s are approximately 0.6 for torques that are not gravity corrected7–10 or about 0.5 when gravity corrected.8,11 Recommended differences in homologous hamstrings and quadriceps ratios are less than 0.1.7–9
Despite the extensive body of isokinetic literature, few studies have been specific to youth12–21—athletes or nonathletes—and even fewer have afforded muscle-strength comparisons of girls and boys.12,16,17,20 Comparing existing data is difficult because study procedures varied in testing speeds, normalization for body mass, and adjustments for the influence of gravity. It is especially surprising how few hamstrings and quadriceps strength data specific to basketball athletes have been published.12,22,23 First, basketball is the most common team sport in which Americans age 6 years and older participate.24 Second, attention to the greater risk of anterior cruciate ligament (ACL) injury for female basketball players and other non-collision–sport athletes at high school through the professional ranks has increased during the past 2 decades.3,4,6,25–30 According to National Collegiate Athletic Association studies,3,4 the rate of ACL injury is at least 3 times greater for women basketball players versus men. Many athletic trainers and sports medicine professionals believe strength, especially of the hamstrings, and H:Q ratios are important factors in this difference.14,18,25,26,31–33 To clarify whether strength and muscle ratios are informative about sex differences, it is important to have access to normative strength data for the hamstrings and quadriceps that characterize the at-risk population. Such data refine the athletic trainer's ability to design and implement injury-prevention programs and basketball-specific conditioning programs.
The purpose of our cross-sectional study was to assess the hamstrings and quadriceps strength characteristics of basketball players ages 11–13 and 15–17 years old (yo) competing in a national tournament. Besides contributing sport-specific normative data, we investigated whether developmental differences in strength existed that could be associated with sex or age. Prior researchers have documented increasing strength from childhood to young adulthood, with greater strength gains postpuberty for boys than for girls.8,17,21,34 Our hypotheses for hamstrings and quadriceps strength were that (1) players 15–17 yo would be relatively stronger than 11–13 yo players and (2) sex differences in relative strength would increase with age. The literature regarding muscle ratios is less clear. Although researchers have documented changes in ratios with training, an important observation for those who consider a higher ratio to be protective against knee injury, support for sex and age differences in ratios among similarly active samples is limited.12,14,20,23,35 Our hypothesis was that the ipsilateral H:Q and homologous muscle ratios of the study participants would be the same between the sexes and across ages.
METHODS
Preparation
During the 2 months before data collection, we trained research assistants on all aspects of participant recruitment and data collection. The first author (P.A.B., an ATC, PT, with more than 20 years' experience) had primary responsibility for isokinetic testing instruction. We gave copies of the testing protocol to the assistants, supervised several practice sessions, and had assistants work in pairs during actual data collection to facilitate protocol standardization.
Recruitment and Subjects
We recruited study participants during the 2000 American Youth Basketball Tour (AYBTour) National Tournament, which included two 5-day sessions and drew 328 teams (199 boys' and 129 girls' teams) from throughout the Midwest. Session 1 was for players who had recently completed grades 4 through 8; session 2 involved players in grades 8 through 11. Registration was held the evening of day 1, pool games occurred all day on days 2 through 4, and tournament play occurred on day 5. Registration for session 2 occurred on day 5 of session 1. Tournament games consisted of two 20-minute halves played with a running clock. Rules required coaches to give all team members approximately equal playing time during every game.
We used the typical ages of peak height velocity (girls = 11.4–12.2 yo, boys = 13.4–14.4 yo), a key indicator of the onset of puberty,34 in combination with the age limits for tournament players in order to establish the study's age groups (11–13 yo and 15–17 yo). We excluded players 14 yo in order to provide a 1-year separation between groups, thereby increasing the likelihood that the younger players were prepubescent or peripubescent and the older players were postpubescent.
Recruitment and screening of participants began during session registration and continued through days 2 through 4. Researchers and research assistants had prominent tables at the registration site and the main gymnasium; circulated among all competition sites; wore distinctive clothing to enhance visibility; and informed as many players, coaches, and parents as possible, verbally and with flyers, about the study.
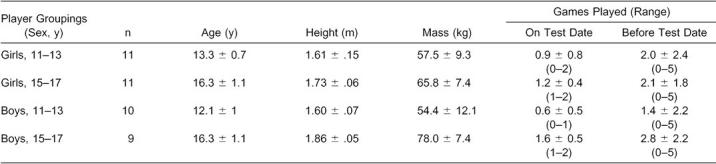
We verbally screened interested and qualified players with the assistance of their parents or guardians to assess their eligibility for the study. Qualified participants had no history of knee ligament sprain or knee surgery, no other injury or illness that would affect performance or measurements during the study, and were able to hop comfortably on each leg. To check the accuracy of self-reports, we inspected players for surgical scars about the knees and observed their skin and general behavior for indicators of illness or injury. Participants scheduled testing appointments after they passed screening and provided written consent. We ensured that players had at least an hour break between their last games and their testing sessions. Forty-one participants (22 girls, 19 boys) completed the study. Table 1 presents participants' characteristics, including number of games played before testing. We conducted the study in accordance with the policies of the Indiana University Bloomington Campus Committee for the Protection of Human Subjects.
Table 1.
Participants' Characteristics
Procedures
The first author (P.A.B.) calibrated the isokinetic dynamometer before each data-collection day. In order to normalize torques to body mass and adjust for the differential effects of gravity, we measured and recorded each player's height and mass. We sat players next to a Cybex II dynamometer and Chart Recorder (Lumex, Inc, Ronkonkoma, NY); secured them with thigh, pelvic, and chest straps; and had them fold their arms across their chests for testing. The shin pad was positioned as distally as possible without limiting ankle dorsiflexion. After instruction and familiarization trials (3–4 submaximal and 3–4 maximal-effort trials), players performed 6 trials of maximal concentric knee extension and flexion at 60°/s with each lower extremity. The side on which testing began was alternated from 1 player to the next to eliminate order effect. To maintain consistency among the research assistants involved in data collection, we provided no verbal encouragement during testing.8 For motivation, we relied on the initial instructions to push and pull as hard and fast as possible.
Data Processing and Analysis
Our basic research design was a 2 × 2 analysis of variance (ANOVA) with 2 levels each for sex and age. Given this design, an α of .05, and the expectation of a large effect size based on a study by Holmes and Alderink,16 we used the methods of Cohen36 to estimate that a minimum n of 7 per cell would provide power of 0.80.
We entered peak torques and corresponding angles from the chart recordings and the data into Excel 2000 (version 9.0, Microsoft Corp, Redmond, WA) spreadsheets for further processing. After converting these torques to newton meters and correcting for the effects of gravity, we normalized them relative to body mass (Nm/kg). Although several context-specific methods for assessing limb dominance37 exist, our focus on strength led us to select total leg strength7 as the determinant. The strength-dominant leg for each player was defined as the leg with the higher sum after adding the peak torques for all isokinetic trials within a leg (2 muscle groups × 6 trials = 12 trials). For each player, we used the average38 of the 6 trials per muscle group and leg to identify 8 dependent variables: hamstrings peak torque relative to body mass (PT/BM), quadriceps PT/BM, and H:Q ratios for the dominant (D) and nondominant (ND) legs; ND hamstrings to D hamstrings ratios (NDH:DH); and ND quadriceps to D quadriceps ratios (NDQ:DQ).
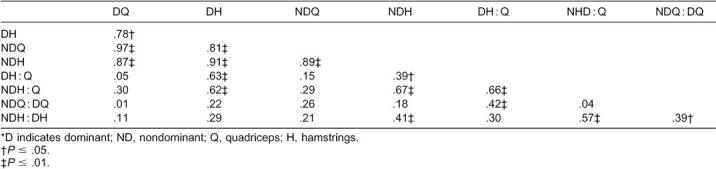
We used gravity-corrected and body-mass–normalized peak torques and ratios in the statistical analysis. Initially, we reviewed the Pearson product moment correlation matrix for the 8 dependent variables (Table 2). Because hamstrings and quadriceps average PT/BM for the D and ND legs were all highly correlated,39 we used separate 2 × 2 ANOVA designs with general linear-model univariate procedures to consider if there were sex- and age-group (11–13 yo and 15–17 yo) differences in these 4 measures. We set the familywise α at .05, and a Bonferroni adjustment was made to .0125 (.05/4 ANOVAs, 1 per dependent variable) to minimize the risk of a type I error.40 Similarly, we adopted this α criterion and Bonferroni adjustment strategy for any post hoc testing of interactions with independent-samples t tests. The homogeneity of the sample distributions was confirmed by monitoring the Levene test of equality of error variance for each ANOVA and t test. Because 4 of the 6 correlations among ratios were moderate,39 we used a 2 × 2 multivariate ANOVA (general linear model, multivariate procedures) to control for inflation of type I error while assessing for differences in 4 ratio measures (DH:Q, NDH:Q, NDH:DH, and NDQ:DQ) between sexes and age groups (11–13 yo and 15–17 yo).40 We designated α at .05 for this multivariate ANOVA and verified homogeneity with the Box test of equality of covariance matrices. SPSS for Windows software (version 11.0, SPSS Inc, Chicago, IL) was used for all statistical analyses.
Table 2.
Correlation Matrix of Relative Strength and Ratio Variables*
RESULTS
For the single muscle-group relative-strength measures, r values ranged from .78 to .97, suggesting that a player who is strong (or weak) in 1 muscle group is strong (or weak) in all 4 (Table 2). Correlations between ratios ranged from .04 to .66. Relative hamstrings strength and H:Q ratio correlations were moderate; those between relative quadriceps strength and H:Q ratio were low.39
Players in the 15–17 yo age group had significantly stronger average hamstrings PT/BM than 11–13 yo players (Table 3). For the D hamstrings, the 15–17 yo players' group mean was 35.8% higher than the 11–13 yo players' mean (F1,37 = 7.858, P = .008, η2 = .175). For the ND hamstrings, the 15–17 yo players' group mean was 40.8% greater than that of the 11–13 yo players (F1,37 = 9.335, P = .004, η2 = .201). Although boys overall were 12.4% (D) and 13.0% (ND) stronger than girls, differences between boys and girls in their average hamstrings PT/BM were not significant (D, F1,37 = 1.302, P = .261, η2 = .034; ND, F1,37 = 1.349, P = .253, η2 = .035). Girls 15–17 yo were 22.9% (D) and 21.1% (ND) stronger than girls 11–13 yo; older boys were 51.3% (D) and 65.8% (ND) stronger than the younger boys. The girls and boys 11–13 yo had similar hamstrings PT/BM, whereas boys 15–17 yo were 24.1% (D) and 30.2% (ND) stronger than girls of the same age. However, these sex- and age-related differences in average hamstrings PT/BM did not significantly interact (D, F1,37 = 1.188, P = .283, η2 = .031; ND, F1,37 = 2.278, P = .140, η2 = .058).
Table 3.
Average Hamstrings (H) Peak Torques, Quadriceps (Q) Peak Torques, Hamstrings:Quadriceps (H:Q) Ratios of Dominant (D) and Nondominant (ND) Legs, and Hamstrings (NDH:DH) and Quadriceps (NDQ:DQ) Ratios (Mean ± SE)
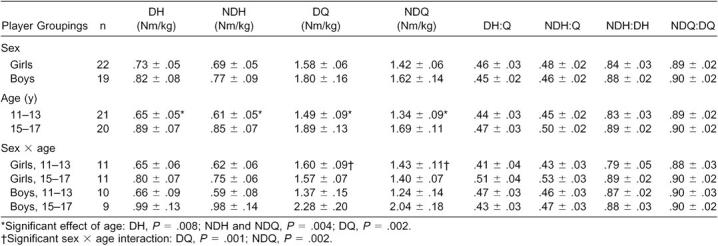
Similarly, a main effect of age for the average quadriceps PT/BM was observed (see Table 3). Players 15–17 yo were stronger than players 11–13 yo by 26.6% for the dominant leg (F1,37 = 11.144, P = .002, η2 = .231), and by 26.0% for the nondominant leg (F1,37 = 9.420, P = .004, η2 = .203). Although boys overall were 13.9% (D) and 14.5% (ND) stronger than girls, we found no main effect of sex for quadriceps strength (D, F1,37 = 3.473, P = .07, η2 = .086; ND, F1,37 = 3.252, P= .079, η2 = .081). We observed a significant sex × age interaction for both legs (D, F1,37 = 12.938, P = .001, η2 = .259; ND, F1,37 = 10.719, P = .002, η2 = .225; Figures 1 and 2). Four post hoc independent t tests were used to further evaluate this interaction (α = .0125). The relative quadriceps strength of girls did not differ with age (D, t20 = .286, P = .778; ND, t20 = .200, P = .843), whereas boys 15–17 yo were 66.3% (D, t17 = −3.677, P = .002) and 63.9% (ND, t17 = −3.521, P = .003) stronger than boys 11–13 yo. Although girls 11–13 yo were somewhat stronger than boys 11–13 yo, these differences were not significant (D, 16.6%, t19 = 1.334, P = .198; ND, 14.9%, t19 = 1.063, P = .301). Boys 15–17 yo had higher average quadriceps PT/BM than girls 15–17 yo (D, 45.7%, t10.134 = −3.306, P = .008; ND, 45.3%, t18 = −3.514, P = .002).
Figure 1.

Sex × age interaction for average quadriceps torques (Nm/kg) of dominant-leg strength ± SE. Sex × age, P = .001; age, P = .002. Boys 15–17 years old > boys 11–13 years old, P = .002. Boys 15–17 years old > girls 15–17 years old, P = .008.
Figure 2.

Sex × age interaction for average quadriceps torques (Nm/kg) of nondominant-leg strength ± SE. Sex × age, P = .002; age, P = .004. Boys 15–17 years old > boys 11–13 years old, P = .003. Boys 15–17 years old > girls 15–17 years old, P = .002.
Overall results of the multivariate ANOVA were not significant (sex, omnibus F3,37 = 0.681, P = .610, η2 = .074; age, omnibus F3,37 = 0.851, P = .503, η2 = .091; sex × age, omnibus F3,37 = 1.357, P = .269, η2 = .138). For both legs, participants had similar H:Q, NDH:DH, and NDQ:DQ ratios between the sexes and ages.
DISCUSSION
This study is one of two we know that present normative strength data for both boys and girls active in competitive basketball. This study is further distinguished by the inclusion of players 11–13 yo along with high school–aged players. Our results provide support for the hypothesis that players 15–17 yo have stronger hamstrings and quadriceps relative to body mass than players 11–13 yo. The finding of a sex × age interaction for the quadriceps supports our proposal that sex differences in relative strength increase with age; however, this was not the case for the hamstrings. The absence of differences in the H:Q and homologous muscle ratios of our players also suggests the hypotheses of no sex- or age-related differences or interactions for these measures are valid.
Collectively, the players 15–17 yo had significantly greater relative hamstrings and quadriceps strength than the athletes 11–13 yo. Although boys and girls did not differ when pooled across ages, we observed an interaction effect for relative quadriceps strength. This interaction was predominantly driven by the more than 60% higher relative quadriceps strength of the boys 15–17 yo versus the boys 11–13 yo, whereas, surprisingly, the girls' age groups did not differ. This was not the case for relative hamstrings strength, which was about 20% higher for girls 15–17 yo and more than 50% higher for boys 15–17 yo compared with the players 11–13 yo. Such sex- and age-related changes in relative strength occur concurrently with changes in mass. In our cross-sectional examination of these changes, boys 15–17 yo were 43.4% heavier than boys 11–13 yo; the girls' age groups only differed by 14.4%. Although normalization of strength to body mass facilitates comparisons across groups, it does not eliminate the observation of notably different patterns of change in relative strength for hamstrings versus quadriceps in the girls compared with the boys.
We found support for the hypotheses of no differences in ratios. The slightly higher H:Q ratios in girls 15–17 yo versus girls 11–13 yo likely reflect the higher relative hamstrings strength in the former group coupled with no difference in relative quadriceps strength. Relative strengths of the hamstrings and quadriceps were more discriminating measures than ratios in identifying sex- and age-related differences among our participants. Players with similar H:Q ratios could have differed considerably in relative strength. For example, a girl and boy 11 yo had similar dominant H:Q ratios of 0.55 and 0.51 but very different relative strengths of 0.61:1.11 for the girl and 1.10:2.17 for the boy. The correlations between measures support our view that relative strength is more informative than ratios about athletes' strength profiles. Correlations of relative strength between muscle groups were consistently high, whereas those between ratios or ratio and muscle group varied and were moderate at best.
We are not the first to report sex differences in quadriceps strength for either athletes or the general population. In 3 studies, Wojtys et al41–43 found men to have significantly greater relative quadriceps strength (tested at 60°/s) than women. In one study, they also identified differences in relative hamstrings strength.41 Their groups of young adults ranged from sedentary to elite in activity levels. Closer comparisons of our findings with other studies are limited due to the few studies of youth and female athletes12–16,18–22 and differences in isokinetic testing methods.
We know of 3 groups of researchers who tested the hamstrings and quadriceps of athletic boys and girls at 60°/s. Anderson et al12 studied 100 high school varsity basketball girls and boys and identified greater relative strength of the hamstrings and quadriceps in boys. With a sample of 16 boys and 31 girls who were 15–18 yo and active in a variety of sports, Holmes and Alderink16 also reported boys had greater relative strength in both hamstrings and quadriceps. Tabin et al20 tested 60 athletic children 10–15 yo and confirmed their puberty status with the use of the Tanner scale. The prepubescent boys and girls had similar peak hamstrings and quadriceps torques normalized to lean body weight. Postpubescent boys and girls were similar in hamstrings strength, but boys were notably stronger in the quadriceps. Anderson et al12 found significant sex differences in H:Q ratios, whereas none occurred in the other 2 studies.16,20
Kanehisa et al17 did not investigate athletes but provided a different perspective on isokinetic quadriceps strength at 60°/s by normalizing to cross-sectional area of the quadriceps relative to thigh length. With a much wider age separation than our study, adults 18–25 yo versus boys and girls 6–9 yo, they reported main effects of age, no sex difference for the group 6–9 yo, but greater strength in the men. Collectively, these studies suggest that the presence of relative quadriceps weakness in girls versus boys after puberty is a robust phenomenon and not specific to the sample of basketball players we tested in this study.
Why the relative strength of girls 15–17 yo compared with girls 11–13 yo was greater in the hamstrings but not in the quadriceps is unclear. Physiologic changes associated with puberty, including those mediated by increasing levels of testosterone that are typically greater for boys than girls, would seemingly have similar effects on the mass and strength of both hamstrings and quadriceps and contribute to age-related strength differences.17,34 One proposition that may clarify the difference in relative hamstrings strength versus relative quadriceps strength is that after puberty, girls use different coordination strategies than boys, which place alternative strength demands on the musculature. Hewett44 suggested that prepubescent athletic girls use different jumping-landing coordination patterns than postpubescent athletic girls, and other authors41 noted sex differences in patterns of neuromuscular response to perturbation, which may result in different demands on these muscle groups. A second possibility that may affect girls' potential use of different coordination strategies is that athletic girls may have less cumulative exposure and experience playing basketball than age-matched boys. Without separating athletes by sex, Hahn et al45 correlated years of sport experience with absolute quadriceps strength. Correlations were significant for soccer and jogging but not for basketball. Simply playing basketball (or other sports) may not sufficiently strengthen the quadriceps. A third possibility is that athletic girls may be less involved with strength training than athletic boys due to sociocultural mores that discourage or delay strength training among girls. Also, if anecdotal reports from AYBTour coaches during this study are accurate, girls face less competition to make a team than boys and so may have less incentive to strength train. Girls may not be engaging in other performance-enhancing activities to the same degree as boys. Details about the onset of regular strength training and the types of training for athletic girls and boys need to be clarified. Demands on the antigravity muscles during basketball and other acceleration-deceleration sports to control body mass safely and effectively imply the need for adequate strength of the hip, knee, and ankle extensors and flexors. These proposals are speculative and illustrate the need for further study to better explain sex differences in strength and risk of injury.
Besides contributing to the movements needed for sport-related tasks, muscular contraction contributes to joint stiffness, which may protect against injury. Voluntary intrinsic torque production at the ankle directly relates to ankle stiffness,46 and decreased anterior tibial translation and increased knee-joint stiffness occur during active cocontraction of the musculature surrounding the knee.43,47 Joint compression combined with quadriceps force also stiffens the knee and limits anterior tibial translation.48 Wojtys et al43 found notable increased knee stiffness in response to cocontraction for men and women, although men achieved higher stiffness levels than women. Men also had greater relative quadriceps strength than women. Interestingly, sex—not relative hamstrings and quadriceps strength—predicted stiffness. Stronger musculature about the knee, along with other, unspecified sex-related factors, may increase stiffness and reduce the chance of ligamentous injury.
The importance of strength is a prominent feature of recent studies concerning ACL injury. Anderson et al12 identified a significant but low positive correlation between quadriceps total work tested at 60°/s and ACL cross-sectional area for high school basketball girls and boys. A similar correlation occurred between quadriceps strength and ACL cross-sectional area but only for girls. Their suggested association between greater quadriceps strength and larger, potentially stronger ACLs is consistent with adaptation to strain on the ACL from quadriceps-induced, nonpathologic anterior tibial translation. Lund-Hanssen et al18 compared the quadriceps and hamstrings strength of the healthy, uninvolved legs of women handball players with unilateral ACL injuries to a control group of handballers. Although strength measures were similar at 60°/s, the quadriceps torque at 240°/s for the healthy legs of the injured group was significantly less than that of the control group, which contributed to higher H:Q ratios for the healthy legs of the injured players. Based on isokinetic testing at 360°/s, Hewett et al14 reported increased absolute hamstrings strength and H:Q ratios but no changes in quadriceps strength among a group of teenage female volleyball athletes following a preseason conditioning program that emphasized plyometric jump training, weight training, and stretching. The apparent lack of improvement in quadriceps strength supports the notion that this muscle group needs targeted overload training to develop sufficient strength among girls. Hewett et al35 subsequently conducted a 1-year prospective study of knee injuries among female and male high school athletes following similar programs. The results suggested a beneficial effect of the training program in reducing knee injuries among athletic girls. However, the authors offered no data regarding the effects of their program on the strength of these athletes.
The importance of our findings should be evaluated in light of the fact that players were tested during a tournament. Although participation durations were restricted by equal-play rules and the use of a running clock, fatigue may have inhibited some participants from providing maximal effort during testing. Alternatively, these conditions may more accurately reflect the strength characteristics of players during practice and competition. A second consideration is that we did not assess pubertal status directly but used typical ages of peak height velocity to separate participants into age groups. Although definitely identifying the pubertal status of participants is one approach to categorizing players, youth sports such as basketball typically form teams based on players' ages or grade levels. From that perspective, our use of age grouping may be a better match to the general practice of organizing teams for basketball players 11–17 yo. Third, the results of this study are specific to strength assessed at 60°/s. We selected this velocity to enhance reliability, as testing people naive to isokinetics at higher velocities makes ensuring maximal effort more challenging. Finally, the absence of main effects for sex and no sex × age interactions for the hamstrings may have been due to type II error. However, the power analysis suggested this risk was reasonably low. Additionally, the partial η2 values for effects of age for both hamstrings and quadriceps and the significant sex × age interactions for quadriceps ranged from 0.175 to 0.259 and corresponded to F values of approximately 0.46 to 0.58, suggesting large effect sizes.36
CONCLUSIONS
The results of this cross-sectional study of girls and boys playing competitive basketball include age effects for both the hamstrings and quadriceps and a sex × age interaction for the quadriceps. Although players 15–17 yo had stronger hamstrings and quadriceps relative to body mass than players 11–13 yo, overall, girls did not differ from boys. However, girls 15–17 yo had notably weaker quadriceps strength relative to body mass than their male counterparts. This may place girls at a disadvantage for safely managing the external forces inherent in their sport. We found no differences in H:Q ratios or homologous quadriceps and hamstrings ratios among these basketball players, which suggests such ratios do not sufficiently characterize muscular function. We recommend that strength assessments emphasize torques relative to body-mass measures, with ratios providing secondary information.
Our findings, although providing data on the hamstrings and quadriceps strength of youth basketball players, lead to questions about the role of relative hamstrings and quadriceps strength in ACL injury prevention. Researchers need to continue efforts to define adequate sport-specific strength levels that are sex and age appropriate. Because athletes at a minimum must control their own body mass during the acceleration and deceleration tasks common in basketball and other sports, we concur with Perrin8,9 that isokinetic torques should be reported relative to body mass (Nm/kg) following appropriate gravity correction. We also call for researchers to better understand the apparently widespread weakness specific to the relative quadriceps strength of women and girls after puberty compared with men and postpubescent boys. Another question is if increasing the relative quadriceps strength of girls and women, while not neglecting the strength of other muscles affecting the knee, would improve their ability to stiffen the knee. Additionally, prospective, longitudinal studies are needed to assess whether relative quadriceps strength, relative hamstrings strength, or H:Q ratios of athletic girls and women affect their incidence of ACL injuries. Normative data for groups are informative but insufficient to establish relationships with risk of injury. By having more information about athletes' strength profiles before injury, athletic trainers can better clarify these relationships.
Although no gold standard yet exists for the magnitude of quadriceps or hamstrings torques, we suggest that athletic trainers use available sport- and age-specific male normative data to guide the training of female athletes of the same age active in similar sports. Granted, most girls and boys differ notably in body composition and testosterone levels after puberty, with most boys being stronger than most girls within age and sport groupings. Yet it is alarming that girls 15–17 yo did not differ from girls 11–13 yo in relative quadriceps strength, whereas the relative quadriceps strength of boys 15–17 yo was more than 60% higher than boys 11–13 yo. We encourage athletic trainers and other sports medicine professionals to assist more athletic girls to strengthen their quadriceps and other lower extremity muscles in keeping with their changing mass and the demands of their sports. Well-designed and appropriately supervised strength-training programs need to be widely available to the large number of athletic girls as they enter and pass through puberty and not await the smaller population of collegiate women athletes.
ACKNOWLEDGMENTS
We thank Chris Gosheff, Alison Jones, Ryan McNeely, Amy Reinhart, Calvin Smallwood, and Freda Smith for their assistance during data collection; Indiana University (Bloomington, IN) President's Summer Undergraduate Research Initiative for financial support; the American Youth Basketball Tour Tournament staff (East Grand Rapids, MI) for their encouragement and cooperation during this study; and the Gatorade Division of the Quaker Oats Company (Chicago, IL) for in-kind support.
REFERENCES
- 1.Clark JE. A dynamical systems perspective on the development of complex adaptive skill. In: Dent-Read C, Zukow-Goldring P, editors. Evolving Explanations of Development: Ecological Approaches to Organism-Environment Systems. Washington, DC: American Psychological Association; 1997. pp. 383–406. [Google Scholar]
- 2.Keogh J, Sugden D. Movement Skill Development. New York, NY: Macmillan; 1985. [Google Scholar]
- 3.Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. Am J Sports Med. 1995;23:694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- 4.Arendt EA, Agel J, Dick R. Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train. 1999;34:86–92. [PMC free article] [PubMed] [Google Scholar]
- 5.Powell JW, Barber-Foss KD. Injury patterns in selected high school sports: a review of the 1995–1997 seasons. J Athl Train. 1999;34:277–284. [PMC free article] [PubMed] [Google Scholar]
- 6.Powell JW, Barber-Foss KD. Sex-related injury patterns among selected high school sports. Am J Sports Med. 2000;28:385–391. doi: 10.1177/03635465000280031801. [DOI] [PubMed] [Google Scholar]
- 7.Davies GJ. A Compendium of Isokinetics in Clinical Usage and Rehabilitation Techniques. 3rd ed. Onalaska, WI: S & S; 1987. [Google Scholar]
- 8.Perrin DH. Isokinetic Exercise and Assessment. Champaign, IL: Human Kinetics; 1993. [Google Scholar]
- 9.Perrin DH. Open chain isokinetic assessment and exercise of the knee. J Sport Rehabil. 1994;3:245–254. [Google Scholar]
- 10.Goslin BR, Charteris J. Isokinetic dynamometry: normative data for clinical use in lower extremity (knee) cases. Scand J Rehabil Med. 1979;11:105–109. [PubMed] [Google Scholar]
- 11.Appen L, Duncan PW. Strength relationship of the knee musculature: effects of gravity and sport. J Orthop Sports Phys Ther. 1986;7:232–235. [PubMed] [Google Scholar]
- 12.Anderson AF, Dome DC, Gautam S, Awh MH, Rennirt GW. Correlation of anthropometric measurements, strength, anterior cruciate ligament size, and intercondylar notch characteristics to sex differences in anterior cruciate ligament tear rates. Am J Sports Med. 2001;29:58–66. doi: 10.1177/03635465010290011501. [DOI] [PubMed] [Google Scholar]
- 13.Calmels P, Van Den Borne I, Nellen M, Domenach M, Minaire P, Drost M. A pilot study of knee isokinetic strength in young, highly trained, female gymnasts. Isokinet Exerc Sci. 1995;5:69–74. [Google Scholar]
- 14.Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]
- 15.Hildebrand KA, Mohtadi NGH, Kiefer GN, Tedford K, Massey A, Brant R. Thigh muscle strength in preadolescent girls. Clin J Sport Med. 1994;4:108–112. [Google Scholar]
- 16.Holmes JR, Alderink GJ. Isokinetic strength characteristics of the quadriceps femoris and hamstring muscles in high school students. Phys Ther. 1984;64:914–918. doi: 10.1093/ptj/64.6.914. [DOI] [PubMed] [Google Scholar]
- 17.Kanehisa H, Ikegawa S, Tsunoda N, Fukunaga T. Strength and cross-sectional area of knee extensor muscles in children. Eur J Appl Physiol. 1994;68:402–405. doi: 10.1007/BF00843736. [DOI] [PubMed] [Google Scholar]
- 18.Lund-Hanssen H, Gannon J, Engebretsen L, Holen K, Hammer S. Isokinetic muscle performance in healthy female handball players and players with a unilateral anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 1996;6:172–175. doi: 10.1111/j.1600-0838.1996.tb00085.x. [DOI] [PubMed] [Google Scholar]
- 19.Russell KW, Quinney HA, Hazlett CB, Hillis D. Knee muscle strength in elite male gymnasts. J Orthop Sports Phys Ther. 1995;22:10–17. doi: 10.2519/jospt.1995.22.1.10. [DOI] [PubMed] [Google Scholar]
- 20.Tabin GC, Gregg JR, Bonci T. Predictive leg strength values in immediately prepubescent and postpubescent athletes. Am J Sports Med. 1985;13:387–389. doi: 10.1177/036354658501300604. [DOI] [PubMed] [Google Scholar]
- 21.Weldon G, Snouse SL, Shultz S. Normative strength values for knee, shoulder, elbow and ankle for females ages 9–73 as determined by isokinetic testing. Athl Train J Natl Athl Train Assoc. 1988;23:325–331. 336, 337. [Google Scholar]
- 22.Berg K, Blanke D, Miller M. Muscular fitness profile of female college basketball players. J Orthop Sports Phys Ther. 1985;7:59–64. doi: 10.2519/jospt.1985.7.2.59. [DOI] [PubMed] [Google Scholar]
- 23.Rosene JM, Fogarty TD, Mahaffey BL. Isokinetic hamstrings: quadriceps ratios in intercollegiate athletes. J Athl Train. 2001;36:378–383. [PMC free article] [PubMed] [Google Scholar]
- 24.Sporting Goods Manufacturing Association. The SGMA report: sports participation topline report: statistical highlights from the superstudy of sports participation. Available at: http://www.sgma.com/reports/2002/report1018899362–6569.html. Accessed July 25, 2002.
- 25.Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2000;8:141–150. doi: 10.5435/00124635-200005000-00001. [DOI] [PubMed] [Google Scholar]
- 26.Harmon KG, Ireland ML. Gender differences in noncontact anterior cruciate ligament injuries. Clin Sports Med. 2000;19:287–302. doi: 10.1016/s0278-5919(05)70204-0. [DOI] [PubMed] [Google Scholar]
- 27.Malone TR, Hardaker WT, Garrett WE, Feagin JA, Bassett FH. Relationship of gender to anterior cruciate ligament injuries in intercollegiate basketball players. J South Orthop Assoc. 1993;2:36–39. [Google Scholar]
- 28.Messina DF, Farney WC, DeLee JC. The incidence of injury in Texas high school basketball: a prospective study among male and female athletes. Am J Sports Med. 1999;27:294–299. doi: 10.1177/03635465990270030401. [DOI] [PubMed] [Google Scholar]
- 29.Oliphant JG, Drawbert JP. Gender differences in anterior cruciate ligament injury rates in Wisconsin intercollegiate basketball. J Athl Train. 1996;31:245–247. [PMC free article] [PubMed] [Google Scholar]
- 30.Zelisko JA, Noble HB, Porter MA. Comparison of men's and women's professional basketball injuries. Am J Sports Med. 1982;10:297–299. doi: 10.1177/036354658201000507. [DOI] [PubMed] [Google Scholar]
- 31.Bonci CM. Assessment and evaluation of predisposing factors to anterior cruciate ligament injury. J Athl Train. 1999;34:155–164. [PMC free article] [PubMed] [Google Scholar]
- 32.More RC, Karras BT, Neiman R, Fritschy D, Woo S, Daniel DM. Hamstrings—an anterior cruciate ligament protagonist: an in vitro study. Am J Sports Med. 1993;21:231–237. doi: 10.1177/036354659302100212. [DOI] [PubMed] [Google Scholar]
- 33.Shultz SJ, Perrin DH. The role of dynamic hamstring activation in preventing knee ligament injury. Athl Ther Today. 1999;4(3):49–53. [Google Scholar]
- 34.Malina RM, Bouchard C. Growth, Maturation, and Physical Activity. Champaign, IL: Human Kinetics; 1991. [Google Scholar]
- 35.Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes: a prospective study. Am J Sports Med. 1999;27:699–706. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- 36.Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc; 1988. [Google Scholar]
- 37.Gabbard C, Hart S. A question of foot dominance. J Gen Psychol. 1996;123:289–296. doi: 10.1080/00221309.1996.9921281. [DOI] [PubMed] [Google Scholar]
- 38.Dvir Z, David G. Average or peak moment: which of the two is more suitable to represent isokinetic muscle strength? Isokinet Exerc Sci. 1995;5:93–97. [Google Scholar]
- 39.Hinkle DE, Wiersma W, Jurs SG. Applied Statistics for the Behavioral Sciences. 4th ed. Boston, MA: Houghton Mifflin; 1998. [Google Scholar]
- 40.Tabachnick BG, Fidell LS. Using Multivariate Statistics. 3rd ed. New York, NY: HarperCollins; 1996. [Google Scholar]
- 41.Huston LJ, Wojtys EM. Neuromuscular performance characteristics in elite female athletes. Am J Sports Med. 1996;24:427–436. doi: 10.1177/036354659602400405. [DOI] [PubMed] [Google Scholar]
- 42.Wojtys EM, Huston LJ. Neuromuscular performance in normal and anterior cruciate ligament-deficient lower extremities. Am J Sports Med. 1994;22:89–104. doi: 10.1177/036354659402200116. [DOI] [PubMed] [Google Scholar]
- 43.Wojtys EM, Ashton-Miller JA, Huston LJ. A gender-related difference in the contribution of the knee musculature to sagittal-plane shear stiffness in subjects with similar knee laxity. J Bone Joint Surg Am. 2002;84:10–16. doi: 10.2106/00004623-200201000-00002. [DOI] [PubMed] [Google Scholar]
- 44.Hewett TE. Biomechanical issues related to the gender bias in ACL injuries. Presented at: ACL Injuries: The Gender Question, A Research Retreat; April 7, 2001; Lexington, KY. [Google Scholar]
- 45.Hahn T, Foldspang A, Ingemann-Hansen T. Dynamic strength of the quadriceps muscle and sports activity. Br J Sports Med. 1999;33:117–120. doi: 10.1136/bjsm.33.2.117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mirbagheri MM, Barbeau H, Kearney RE. Intrinsic and reflex contributions to human ankle stiffness: variation with activation level and position. Exp Brain Res. 2000;135:423–436. doi: 10.1007/s002210000534. [DOI] [PubMed] [Google Scholar]
- 47.Markolf KL, Graff-Radford A, Amstutz HC. In vivo knee stability: a quantitative assessment using an instrumented clinical testing apparatus. J Bone Joint Surg Am. 1978;60:664–674. [PubMed] [Google Scholar]
- 48.Torzilli PA, Deng X, Warren RF. The effect of joint-compressive load and quadriceps muscle force on knee motion in the intact and anterior cruciate ligament-sectioned knee. Am J Sports Med. 1994;21:105–112. doi: 10.1177/036354659402200117. [DOI] [PubMed] [Google Scholar]