

Introduction
Research consistently reconfirms the high risk of behavioral problems among children in foster care, where recent estimates suggest approximately 50% of the population has clinically significant behavior problems (Leslie, Hurlburt, Landsverk, Barth & Slyman, 2004). Although behavior problems have been linked to both foster care (Kortenkamp & Ehrle, 2005; Smithgall, Gladden, Yang & George, 2005) and a reduced likelihood of reunification and permanency (Fraser, Walton, Lewis, Pecora, & Walton, 1996; Landsverk, Davis, Ganger, Newton & Johnson, 1996; Smithgall et al., 2005) the behavior health of children following foster has been infrequently studied. The purpose of the current study is to test the effect of reunification following long term foster care on children’s behavioral health and explore some of the risks that might account for any differences in outcomes using data from the National Survey of Child and Adolescent Well-being (NSCAW).
Long term Foster Care
Ideally children in foster care benefit from safer living conditions, better parenting from foster caregivers (Minty, 1999), and supportive child welfare services. A few studies have documented a generally positive impact of foster care on children’s developmental outcomes and normative functioning (Colton, Aldgate, & Heath, 1990; Fanshel & Shinn, 1978; Horowitz, Balestracci, & Simms, 2001; Maluccio & Fein, 1985). Current U.S. policy supports the reunification of children with families following foster care when possible, and specifies time limits designed to speed permanency decisions for children and discourage unnecessarily long stays in foster care (P.L. 105-89; ASFA). Despite the policy support for reunification and permanency, many children remain in foster care for extended periods of time (Lowry, 2004). As of 2005, approximately 37 percent of children currently in foster care had stays of 2 years or longer (USDHHS, 2006). Although the population of children with longer foster care stays is over-represented in cross-sectional samples, these children represent a large population of children receiving foster care services at any given time.
A relatively long stay in foster care has specific implications for children and families that make this population important to distinguish in research and practice. For example, behavior problems have been linked to exit from foster care (Fraser et al., 1996; Landsverk et al., 1996). It is therefore reasonable to expect that the population of children who remain in long term foster care would evidence more behavior problems than the population of children with relatively short stays. A longer stay in foster care likely indicates lingering concerns about families’ progress on identified case goals and children’s safe return home (Leathers, 2002). Families who struggle to achieve reunification more frequently face multiple problems and risks as compared to families whose children experience briefer stays in foster care (Karoll & Poertner, 2003; Marsh, Ryan, Choi & Testa, 2006). Another reason to distinguish children in long term foster care is the actual physical separation between children and parents. Children continuously age and develop in foster care and therefore can bring new developmental challenges home with them as well as expectations and routines from their substitute parenting and home life experiences. For these reasons reunification represents a period of readjustment at which time parents may struggle reestablish or recreate parenting routines and roles, particularly if contact with children in foster care has been limited (Leathers, 2002).
Post-Reunification Outcomes
Two key studies have targeted the question of how behavioral outcomes are affected by reunification following foster care. Results based on a study conducted by Taussig et al. (2001), arguably the most recent and rigorous study of reunification to date, suggested that children who return home actually experience a myriad of problems as compared to children who remain in foster care, even when controlling for age and gender. After prospectively following a sample of 149 San Diego children for 6 years, children who were reunified after an average of 2 years in foster care had statistically significantly more problems on 9 of the 14 outcome indicators used in the study. Problems included more legal involvement, substance abuse, self destructive behaviors, as well as CBCL-measured internalizing and externalizing behavior problems.
The authors suggest several different possible explanations for the broad number of problems evidenced by the reunified youth in this study. First, parenting problems that brought children into care were not successfully addressed and youth were subsequently re-exposed to risky home environments. Other researchers who have studied re-entry into care following reunification have pointed out that children are often reunified without a resolution of the family issues that first brought them into the child welfare system (Fraser et al, 1996). Two prominent examples difficult problems facing child welfare involved families include parental psychopathology and family violence, either of which can contribute to child behavior problems (e.g. Connell & Goodman, 2003; Karoll & Poertner, 2003; Marsh et al., 2006; Mierkangas & Dierker, 1998; Patcher, Auinger, Palmer & Weitzman, 2006). Another possible explanation for the deterioration in behavioral health following reunification is that biological families are more commonly exposed to other socioeconomic risk factors, such as poverty and neighborhood problems, as compared to substitute caregivers. A return to fragile home environments, whether introduced by factors within or outside of the family, could erode any gains made in foster care. Finally, the stress of the reunification process itself may also trigger behavior problems as children and parents work to re-establish a home life together following long-term foster care.
Another important study, conducted by Lau and colleagues (2003), followed a different sample of 218 San Diego children for approximately 2 years following a mean of 16 months in foster care. This study included measures of stressful family life events as a possible mechanism by which reunification might impact internalizing problems. Externalizing behavior problems were not described in this article. The findings in this study point to a more complex relationship between reunification and behavior problems than Taussig’s (2001) work suggests. Children who were reunified with their families in this study experienced less social isolation, but they also had more stressful family life events such as unstable living arrangements, illness, and conflict. Reunification, did not have a direct effect internalizing problems at follow-up, but was mediated through these stressful events. This study suggests that although children who are reunified benefit in some respects from their return home, they also risk exposure to family problems, which subsequently increase the risk for poor internalizing behavioral outcomes.
Research to date provides a provocative glimpse into the relationship between reunification and behavioral outcomes for children and suggests that reunification is associated with an increased risk for behavior problems. Other studies indicate that a child characteristics and case history also affect reunification and children’s behavioral health including children’s race, placement disruption, and age (e.g. Barber & Defalbbro, 2004; Wulczyn, Lery & Haight, 2006). Because many of the same factors that influence whether or not children are reunified with their families likewise influence children’s behavioral health, these indicators should be included in studies of outcomes following reunification. The current study seeks to add to the small body of research dedicated to reunification outcomes by examining risks associated with behavior problems, estimating the effect of reunification itself, and by including important child and case history variables.
Methods
Sample
The NSCAW sample of children was selected using a two-stage combined stratification and cluster design. In the first stage the U.S. was divided into nine strata. The majority of children in child welfare reside in eight states which constituted the first eight strata. The ninth and final stratum consisted of the remaining 42 states and the District of Columbia. Within each stratum individual areas served by a single Child Protective Service (CPS) agency constituted the primary sampling units (PSUs). The PSU sampling frame included all service areas with approximately 60 or more cases per year. The smaller service areas that were not included in the sampling frame constituted about 3% of all cases nationally. One hundred PSUs were randomly selected from each stratum using a probability-proportionate-to-size procedure. Of the 100 PSUs selected, eight were considered ineligible because they were in states requiring first contact to the target child’s caregiver to be made by a CPS worker, rather than an NSCAW field representative.
The long term foster care sample, which provided the data source for the current study, originally included 727 children. The primary study eligibility requirements for the long term foster care sample were: 1) out-of-home care for approximately 12 months at the time of sampling, 2) placement into out-of-home care preceded by an investigation of child maltreatment or a period of in-home services and, 3) out-of-home care at the time the sampling frame was produced. Only one child per household was included in the frame for sample selection. Eligible children were randomly sampled from children placed into care between July 1998 and February 1999. Therefore, children in this study had been in care somewhere between 8 and 18 months at sampling. This final sample was weighted, and these weights reflect both the probability of the PSU and the child’s selection. Children were followed across three waves including baseline, 18-month follow-up and 36-month follow-up. Children under the age of 2 were dropped from the current analysis because of the lack of an appropriate measure of behavior problems for very young children, resulting in a final sample of 604 children.
Measures
Behavior Problems
Behavior problems were measured using Achenbach’s (1991) Child Behavior Checklist (CBCL). The CBCL was completed by the current caregiver for the target child at baseline and at the 36-month follow-up. The reliability and validity of the CBCL is well-established and the measure has been used frequently throughout research on similar populations in both foster care and mental health studies (Leslie et al., 2000; Noser & Bickman, 2000). The clinical threshold, which is indicated by a score of 64 or higher, was used as a measure of clinical behavior problems. The total standardized scores of the CBCL were used to control for behavioral health at baseline.
Reunification and Stability
Reunification measures were derived from caseworker and caregiver reports. Reunification was measured as a dichotomous variable that captured whether or not the child was reunified at any given wave. Living arrangement stability was measured as the total number of living arrangements experienced by the child throughout the study duration based on caseworker reports. These include any moves within and between foster care and families of origin.
Family Risks
Risks were measured at baseline and 36-month follow-up. The mental health scale of the Short-Form Health Survey (SF-12) was used as a general measure of the current caregiver’s mental health at 36-month follow-up (Ware, Kosinski & Keller, 1996). A low score indicates poorer mental health. Low caregiver educational attainment was also measured by the caregivers’ report of whether or not they held a high school diploma or equivalent. The physical violence subscale of the Conflict Tactics Scale (CTS1) was used as an indicator of domestic violence (Straus, Hamby, Boney-McCoy & Sugarman, 1996). Caregivers who reported at least one incidence of assault in the past year were currently considered at risk for domestic violence. Government assistance was defined as the caregivers’ report of current household receipt either WIC (Women Infants and Children), TANF (Temporary Assistance for Needy Families), or food stamps assistance as a proxy measure of poverty. Neighborhood problems were measured by the caregivers’ report on a number of concerning community activities such as assaults and muggings, open drug dealing, and gang activity. Because only 10% percent of the sample reported having any of these neighborhood problems, the variable was dichotomized into the presence or absence of any neighborhood problem.
Control Variables and Covariates
Children’s sociodemographic variables for the analyses, which included the child’s race/ethnicity, gender, and age, were measured at baseline. These variables were derived from administrative data, caregiver, and child self-reports. Case history-related variables included maltreatment and days in foster care at baseline. The type of maltreatment allegedly experienced by the child was based on caseworkers’ report at baseline using a modified version of the Maltreatment Classification Scale (Manly, Cicchetti, & Barnett, 1994). The most severe form of maltreatment reported was used. Other control variables used for the propensity score matching model only included caseworkers’ report of the caregivers need for alcohol or drug services at baseline and the caregivers’ report of whether or not the child received mental health services at baseline.
Analyses
Analyses for the current paper were performed using Stata Statistical Software Release 9 (StataCorp, 2005). Stata’s survey commands were used to account for the sampling and weighting strategy of the NSCAW. Missing data are common for large scale studies that include long term follow-up, but published studies often ignore this problem. Multiple imputation (MI) was employed in the current study to proactively address missing data. In simulation studies MI generally outperforms other approaches such as listwise deletion and setting missing values to the mean, each of which can lead to bias and false identification significant differences (Croy & Novins, 2005). The MI technique was developed based on the seminal work of Rubin (1987) (for a recent and accessible discussion regarding the use of multiple imputation and other methods for missing variables see work by Croy & Novins, 2005).
MI is performed by creating multiple databases based on observed values. In the current study five fully imputed databases were created. Analyses are performed separately in each imputed dataset, and the final point estimates reported in the results are a statistical average of the results of analyses carried out with each of the datasets individually. Standard errors are calculated using an (Analysis of Variance) ANOVA-like formula that accounts for both sampling variation within modeled datasets as well as variability among datasets that reflects the models’ uncertainty. Royston’s (2004) MICE (multiple imputation by chained equations) procedure was used to impute each of the datasets. This procedure employs switching regression, an iterative multivariable regression technique. UVIS (univariate imputation sampling) is called multiple times by MICE to impute missing values in each specified variable based on a multiple regression modeled on specified predictors. Micombine commands are then used to produce model estimates incorporating the ANOVA-like procedure to produce reasonable standard errors.
Almost half of the variables used had no missing data (45.46%). The number of cases with missing data was different across variables. The variables with the most missing data were the current caregivers’ level of education at 36-month follow-up (19.32%) and caregivers’ need for drug related services at baseline (18.71%). All other variables were missing data for 13% or fewer cases. All variables included in the analysis were imputed. Please note that because the descriptive statistics in these analyses are produced using micombine multiple imputation commands, standard deviations are not reported for those analyses.
The percentage of children with behavior problems are first described by comparing two distinct groups of children, those who remained in foster care across all three waves and those children who were reunified and remained in home across all three waves. Examining the prevalence of behavior problems for these groups is used to identify general changes in rates over time. Differences in risks, including primary caregivers’ mental health, education, and domestic violence as well as neighborhood problems, household poverty, and living situation instability are then compared for children who were reunified by the 36-month follow-up and those who remained in foster care to identify risks that might explain differences in behavior problems.
Next, a propensity score model is presented to estimate the effect of reunification on behavioral problems. The propensity score matching technique is used to estimate the effect of a treatment by creating a comparison group matched on potentially confounding covariates. These covariates must either be measured before the treatment, or arguably be unaffected by the treatment (e.g. age or race). In this study, the treatment of interest is reunification for 18-months as measured by reunification at both 18-month and 36-month follow-up. Baseline covariates are used in the first step to create a balanced comparison group of children who remained in foster care across the same 18 months. Stata’s psmatch2 command was used to create the balanced groups. If acceptable balance is achieved on all covariates, then any differences between the two groups can arguably be attributed to the treatment. The covariates used in this analysis included all risk, demographic, and case history variables described above measured at baseline, as well as the caregivers’ need for alcohol or drug treatment services and the children’s use of mental health services. Balance was first achieved by using the first implicate to construct an optimal model. The model was applied to each of the implicates and weights were created in each to reflect the number of times each observation was matched in the final model using Stata’s micombine command.
Finally a logistic regression is presented to test the association between risks and behavior problems for children who have been reunified in order to identify potential targets of reunification interventions. Please note that no goodness of fit statistic is presented here. No test statistic was identified by this author that could successfully be applied to an imputed data set as well as a complex survey design.
Results
The unweighted baseline characteristics of the total sample are presented in Table 1. Children in this sample were just under a mean age of 8 years at baseline, were predominantly Black Non-Hispanic or White Non-Hispanic, and most frequently experienced neglect as the most severe type of maltreatment reported. Figure 1 presents the weighted percentage of children who had clinical levels of internalizing and externalizing behavior problems respectively by reunification pattern across the three waves. As expected, children who remain in foster care have more behavior problems overall. However, although children aged approximately three years over the course of the study and CBCL scores are positively associated with age, the percentage of children who remained in foster with clinical levels of behavior problems showed a small decrease across the 36 month period. In contrast, children who were reunified by the baseline interview and did not return to out of home care showed a distinct pattern that was particularly pronounced for internalizing problems. Children who went home and stayed home had a four fold increase in internalizing behavior problems from baseline to 18-month follow-up. Though the percentage of children with behavior problems at 36 month-follow up decreased, still twice as many children met or exceeded clinical levels at as compared to baseline.
Table 1.
Unweighted Baseling Sample Characteristics of Children in Long Term Foster Care by Reunification Pattern (n=604)
| Mean or Percentage
|
|
|---|---|
| Sociodemographics | |
| Age | 7.75 |
| Gender | |
| Male | 50.33 |
| Female | 49.67 |
| Race/Ethnicity | |
| White Non-Hispanic | 39.90 |
| Black Non-Hispanic | 46.69 |
| Other Non-Hispanic | 13.41 |
| Hispanic | 16.72 |
| Case History | |
| Most Severe Type of Maltreatment | |
| Sexual Abuse | 8.34 |
| Physical Abuse | 14.77 |
| Neglect | 55.70 |
| Other | 21.19 |
| Reunification Pattern | |
| No Reunification | 59.77 |
| Reunification at All Three Waves | 9.50 |
| Other | 30.73 |
Figure 1.
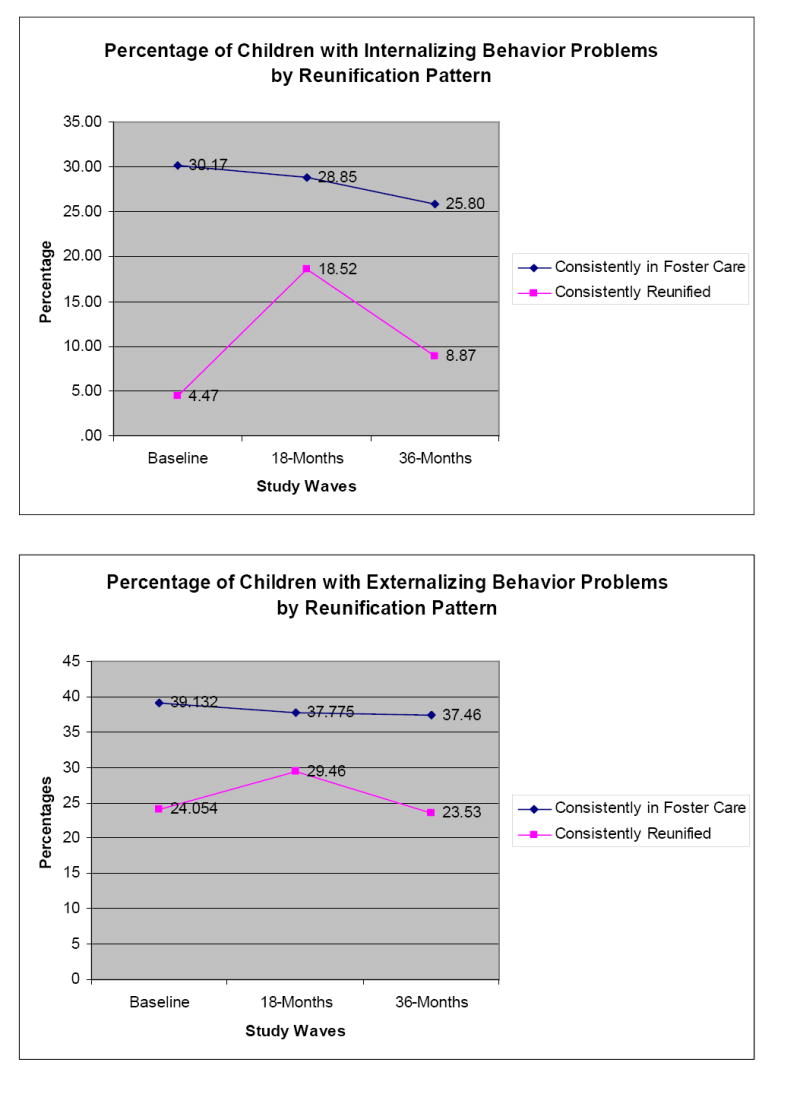
Weighted Sample Changes in Behavior Problems across Waves
Approximately 11% of children in the sample were reunified at both 18-month and 36 month follow-up. The exact number is not reported because the estimate varies by implicate. Reasonable balance was achieved for the propensity score matching model as there were no statistically significant differences between the two groups at baseline on any of the covariates except for children’s age and physical abuse using diagnostics based on the first implicate. Children in the matched control group, or those children who remained in foster care, were slightly younger (7.19 versus 7.82) and less commonly experienced physical abuse (11.73% versus 18.21%). A comparison of the balanced groups indicates that the estimated effect of a return home is a 14 percent reduction in the likelihood of having externalizing behavior problems (OR=.86), however this finding was non-significant. A similar non-significant effect was produced for internalizing behavior problems as well (OR=.89). The outcomes are similar when mean total standardized CBCL scores are used, indicating that reunification in and of itself does not have a statistically significant effect on behavior problems.
Table 2 presents the weighted differences in risks by whether or not children were reunified at the 36-month follow-up. Children who had returned home by the 36-month follow-up were exposed to significantly more risks than children who remained in foster care. The only non-significant difference was the number of changes in living situation. A logistic regression of internalizing behavior problems among children the 175 children who were reunified by 36-month follow-up on risks, demographics, case history, and length of time since reunification is presented in Table 3. Parents’ poorer mental health, male gender, and the experience of sexual abuse were all associated with an increased risk for internalizing behavior problems. Because none of the modeled variables were significantly related to externalizing behavior problems, the results for that model are not presented here.
Table 2.
Weighted Differences in Risks by Reunification (n=604)
| Reunified
|
Not
Reunified |
p-value
|
|
|---|---|---|---|
| Primary Caregiver | |||
| Mental Health | 49.53 | 53.45 | .00 |
| No High School Degree | 27.53 | 9.52 | .00 |
| Domestic Violence | 15.03 | 3.02 | .02 |
| Neighborhood Problems | 48.86 | 21.21 | .00 |
| Government Assistance | 18.03 | 6.63 | .00 |
| Living Situation Instability | 2.89 | 3.23 | .12 |
Please note that a higher score on the parents’ mental health measure indicates better mental health.
Table 3.
Weighted Logistic Regression of 36-Month Follow-up CBCL Scores among Children Who Have Been Reunified (n=175)
| CBCL Internalizing
|
||||
|---|---|---|---|---|
| OR
|
p
|
Confidence Interval
|
||
| Baseline CBCL Total Score | 1.09 | .06 | 1.00 | 1.19 |
| Reunified for 18 Months or Longer | .45 | .32 | .09 | 2.17 |
| Risks | ||||
| Mental Health | .92 | .04 | .85 | .99 |
| No High School Degree | 2.66 | .31 | .40 | 17.85 |
| Domestic Violence in Last Year | .35 | .29 | .05 | 2.53 |
| Changes in Living Situation | .39 | .06 | .14 | 1.05 |
| Neighborhood Problems | 1.34 | .75 | .21 | 8.49 |
| Government Assistance | 1.61 | .60 | 3.84 | .10 |
| Demographics and Case History | ||||
| Age | 1.11 | .20 | .94 | 1.32 |
| Male | 5.90 | .04 | 1.11 | 31.22 |
| Black | .32 | .13 | .07 | 1.41 |
| Physical Abuse | .53 | .59 | .05 | 5.51 |
| Sexual Abuse | .09 | .05 | .01 | 1.01 |
| Constant | .24 | .75 | .00 | 1699.88 |
Please note that a higher score on the parents’ mental health measure indicates better mental health.
Discussion
The four-and two-fold jump in internalizing problems from baseline to 18-month and 36-month follow-up respectively among children who were reunified, stands in contrast to the relatively stable rate of externalizing problems. Analyses presented here suggest this increase in prevalence of internalizing problems is, in part, due to reunified children’s exposure to risks, especially through their caregivers’ relatively poorer mental health, rather than any direct effect of reunification in and of itself. Although, children who remain in foster care in this sample are more likely to have behavior problems, and behavior problems are linked to age, their general risk for behavior problems is somewhat lessened over time. This study suggests that continued long term foster care does not inherently worsen this high-risk group’s behavioral health over time.
The results of this study differ from Taussig’s (2001) work, which suggests almost universally poor outcomes for reunified children as compared to those who remain in foster care across multiple domains. In this study, children who were reunified, even those who were reunified for three years, showed lower rates of behavior problems than children in foster care. The differences in findings could be explained by the variation in study methods. For example, the sample of children in this study came from multiple child welfare jurisdictions across the nation, whereas the earlier study was limited to a California sample. Differences in state and local policy and practice could influence long-term outcomes for children. Also, although both studies employed the CBCL, Taussig used the children’s reports rather than that of the caregivers used here; and caregivers may report fewer behavior problems as compared to their children (Stagner & Lewis, 1993). Furthermore, the current study also had a shorter post-reunification follow-up window. It is possible that increased behavior problems might be revealed over time for children who are reunified.
The results from this study do, however, support conclusions similar to those described by Lau and colleagues (2003). Reunification had no direct effect on behavior problems, but being reunified translates to an increased likelihood of exposure to other risks, which in turn directly effect children’s risk for internalizing problems. Externalizing problems often draw attention and intervention because of their disruptive nature and their association with placement disruption (Newton, Litrownik & Landsverk, 2000) and a reduced likelihood of reunification (Landsverk et al., 1996). This study underscores the importance of interventions aimed at identifying and addressing less obvious internalizing problems among foster care populations following reunification.
Findings from this study also support caregiver mental health as a target for intervention to improve behavioral health outcomes for children following reunification. This need is particularly salient in the context of increasing demands for evidence-based interventions and concerns about the quality of mental health and parenting services provided to children and family serving systems (e.g. Barth et al., 2005; Hoagwood, Burns, Kiser, Ringeisen & Schoenwald, 2001). Unfortunately, funding and delivery of post-reunification services are limited (Bass, Shields, & Behrman, 2004) despite some indication that such services can prevent reunification failures (Hess, 1987). Even though reunification itself was not linked to children’s behavior problems, the reunification experience could take a toll on caregivers’ mental health as they readjust to parenting roles. The elevated risk for behavior problems at the 18-month follow-up, which was particularly pronounced for internalizing problems, may reflect an extended period of readjustment for reunified children. Children who return home face more risks than they do in foster care on average; but other changes, such as moving from one school to another, ending relationships with foster family members, and adjusting to new family routines and parenting, could also have an effect on children’s behavior. Although reunification following long-term foster care can be counted as a success it, by definition, includes a number of potentially stressful changes for both children and families. In this study children who were reunified and those who were not reunified did not differ in the number of changes in their living situation. This is, in part, due to the inclusion of reunification itself as a change. Placement disruption is an often-discussed problem in foster care, and has been linked to subsequent behavior problems (Newton et al., 2000), but less is known about disruptions in family stability following foster care that may likewise have implications for children’s well-being.
Another potential direction for future study is the association between male gender and increased risk for internalizing problems. The finding that boys are nearly six times as likely to have internalizing behavior problems, all else being statistically equal, was unexpected. In this sample boys are, overall, more likely to have clinical levels of internalizing behavior problems across waves. This finding stands in contrast to recent research using a large community based sample (Sterba, Prinstein & Cox, 2007) through which researchers identified similar trajectories of internalizing behavior problems for boys and girls from age 2 to 11 years, but found that a higher proportion of girls are likely to evidence and maintain a relatively high level of internalizing problems.
Most limitations in the current study relate to the nature of the available NSCAW data. First, many of the measures may be biased due to self-report. For example, because so few caregivers reported current alcohol or substance use, this important risk factor was not a useful measure in the current study. Also, these data provide a broad strokes picture of patterns and relationships between risks, reunification and behavior problems through three waves of data are included. Few time points separated by several months provide only brief snapshots and reveal little about patterns and trajectories. Different patterns might be identified for children who have shorter stays in out of home care, and findings presented here should not be generalized to that population. Within this sample there is also variation in the total length of stay as children did not enter foster care at the same time. Finally, although MI was used as the best available option for missing data given the complex data set and simulation studies, this approach is not without its limitations. There is no guarantee that that data are missing at random, or that the model adequately conditioned using observed variables. Future studies will benefit from continuously improving methodological strategies to reduce and address missing data.
The question regarding the effect of reunification on children’s behavioral problems requires further study. Despite the social investment in reunification as a primary goal for child welfare, research has had relatively little to contribute to the understanding of outcomes for children following their return home (Wulczyn, 2004). Future research focused on reunification following foster care would be well-served to use qualitative, mediation and multi-level mixed methods approaches given the potential for interplay between timing, gender, and caregivers’ mental health. Ultimately outcomes related to reunification may likely depend on who reunifies, at what time, and with which supports. Truly longitudinal designs that are specifically built to track the ebb and flow of children’s behavioral problems in relation to family risks and problems following foster care are another essential next step to developing a better understanding of how to promote and maintain successful reunification.
Conclusion
Parents whose children are placed in foster care oftentimes receive supportive services from child welfare as well as a variety of other community providers to make reasonable efforts toward reunification. Reunification is further encouraged by policy mandates and state child welfare performance measures. However, few services and outcomes measures follow children and families after foster care. While their children are in foster care, parents may demonstrate that parenting and safety goals have been met and children are returned home. Unfortunately, over time and without continued support or enduring interventions, the problems and risks that bring families into contact with the child welfare system in the first place can threaten children’s behavioral health. Reunification interventions that are limited to families who have children currently in foster care placement, but do not provide post-reunification services, may not be sufficient. Without efforts to serve families before, during, and following foster care, opportunities to identify and address the behavior problems of one of the most vulnerable populations of children in U.S. are lost.
Acknowledgments
The preparation of this article was supported in part by the Center for Mental Health Services Research, at the George Warren Brown School of Social Work, Washington University in St. Louis; through awards from the National Institute of Mental Health (5P30 MH068579 and 05T32MH01996012), International Order of the Odd Fellows’ First National Christine Smith Scholarship for Research in Child and Family Services, Center for the Study of Social Work Research Dissertation Fellowship, and The New York Foundling Vincent J. Fontana Center for Child Protection Dissertation Grant. Thank you to Jennifer Hill for your skill at communicating complex statistical information.
Footnotes
Confidential: Not to be cited or quoted without the written permission of the author.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Achenbach TM. Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Burlington, VT: University Associates of Psychiatry; 1991. [Google Scholar]
- Barber JG, Delfabbro PH. Children in Foster Care. London: Taylor & Francis; 2004. [Google Scholar]
- Barth RP, Landsverk J, Chamberlain P, Reid JB, Rolls JA, Hurlburt MS, et al. Parent training programs in child welfare services: Planning for a more evidence based approach to serving biological parents. Research on Social Work Practice. 2005;15:353–371. [Google Scholar]
- Bass S, Shields MK, Behrman RE. Children, families, and foster care: Analysis and recommendations. Future Child. 2004;14(1):4–29. [PubMed] [Google Scholar]
- Colton M, Aldgate J, Heath A. Behavioral problems among children in and out of care. Social Work & Social Sciences Review. 1990;2:177–191. [Google Scholar]
- Conell AM, Goodman SH. Psychological Bulletin. 5. Vol. 128. 2002. The association between psychopathology in fathers versus mothers and children’s internalizing and externalizing behavior problems: A meta-analysis; pp. 746–773. [DOI] [PubMed] [Google Scholar]
- Croy CD, Novins DK. Methods for addressing missing data in psychiatric and developmental research. Journal of the American Academy of Child and Adolescent Psychiatry. 2005;44:1230–1240. doi: 10.1097/01.chi.0000181044.06337.6f. [DOI] [PubMed] [Google Scholar]
- Fanshel D, Shinn EB. Children in Foster Care: A Longitudinal Investigation. New York, NY: Columbia University Press; 1978. [Google Scholar]
- Fraser MW, Walton E, Lewis RE, Pecora PJ, Walton WK. An experiment in family reunification: Correlates of outcomes at one-year follow-up. Children and Youth Services Review. 1996;18:335–361. [Google Scholar]
- Hess PM. Parental visiting of children in foster care: Current knowledge and research agenda. Children and Youth Services Review. 1987;9(1):29–50. [Google Scholar]
- Hoagwood K, Burns BJ, Kiser L, Ringeisen H, Schoenwald SJ. Evidence-based practice in child and adolescent mental health services. Pyschiatric Services. 2001;52(9):1179–1189. doi: 10.1176/appi.ps.52.9.1179. [DOI] [PubMed] [Google Scholar]
- Horowitz SM, Balestracci KMB, Simms MD. Foster care placement improves children’s functioning. Archives of Pediatric & Adolescent Medicine. 2001;155:1255–1260. doi: 10.1001/archpedi.155.11.1255. [DOI] [PubMed] [Google Scholar]
- Karoll BR, Poertner J. Indicators for safe family reunification: How professionals differ. Journal of Sociology and Social Welfare. 2003;30(3):139–160. [Google Scholar]
- Kortenkamp K, Ehrle J. New Federalism National Survey of America’s Families. Washington, DC: Urban Institute; 2005. The well-being of children involved in the child welfare system: A national overview. [Google Scholar]
- Landsverk J, Davis I, Ganger W, Newton R, Johnson I. Impact of child psychological functioning on reunification from out of home care. Children and Youth Services Review. 1996;18(45):447–462. [Google Scholar]
- Lau AS, Litrownik AJ, Newton RR, Landsverk J. Going home: The complex effects of reunification on internalizing problems among children in foster care. Journal of Abnormal Child Psychology. 2003;31:345–358. doi: 10.1023/a:1023816000232. [DOI] [PubMed] [Google Scholar]
- Leathers S. Parental visiting and family reunification: Could inclusive practice make a difference? Child Welfare. 2002;81(4):595–616. [PubMed] [Google Scholar]
- Leslie LK, Hurlburt MS, Landsverk J, Barth RP, Slymen DJ. Outpatient mental health services for children in foster care: A national perspective. Child Abuse & Neglect. 2004;28:697–712. doi: 10.1016/j.chiabu.2004.01.004. [DOI] [PubMed] [Google Scholar]
- Leslie LK, Landsverk J, Ezzet-Lofstrom R, Tschann JM, Slyman DJ, Garland AF. Children in foster care: Factors influencing outpatient mental health service use. Child Abuse & Neglect. 2000;24:465–476. doi: 10.1016/s0145-2134(00)00116-2. [DOI] [PubMed] [Google Scholar]
- Lowry MR. Putting teeth into the AFSA: The need for statutory minimum standards. Children and Youth Services Review. 2004;26:1021–1031. [Google Scholar]
- Maluccio AN, Fein E. Growing up in foster care. Children and Youth Services Review. 1985;3:195–201. [Google Scholar]
- Manly JT, Cicchetti D, Barnett D. The impact of subtype, frequency, chronicity, and severity of child maltreatment on social competence and behavior problems. Development and Psychopathology. 1994;6:121–143. [Google Scholar]
- Marsh JC, Ryan JP, Choi S, Testa MF. Integrated services for families with multiple problems: Obstacles to family reunification. Children and Youth Services Review. 2006;28(9):1074–1087. [Google Scholar]
- Mierkangas KR, Dierker LC. Psychopathology among offspring of parents with substance abuse and/or anxiety disorders: A high-risk study. Journal of Child Psychology and Psychiatry. 1998;39(5):711–720. [PubMed] [Google Scholar]
- Minty B. Annotation: Outcomes in long-term foster family care. Journal of Child Psychology and Psychiatry. 1999;40:991–999. [PubMed] [Google Scholar]
- Newton RR, Litrownik AJ, Landsverk JA. Children and youth in foster care: Disentangling the relationship between problem behaviors and number of placements. Child Abuse & Neglect. 2000;24(10):1363–1374. doi: 10.1016/s0145-2134(00)00189-7. [DOI] [PubMed] [Google Scholar]
- Noser K, Bickman L. Quality indicators of children’s mental health services: Do they predict improved client outcomes? Journal of Emotional and Behavioral Disorders. 2000;8:9–18. [Google Scholar]
- Patcher LM, Auinger P, Palmer R, Weitzman M. Do parenting and the home environment, maternal depression, neighborhood, and chronic poverty affect child behavioral problems differently in different racial-ethnic groups? Pediatrics. 2006;117:1329–1338. doi: 10.1542/peds.2005-1784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Royston P. Multiple imputation of missing values. Stata Journal. 2004;4:227–241. [Google Scholar]
- Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York: Wiley; 1987. [Google Scholar]
- Smithgall C, Gladden RM, Yang D, George RM. Behavior Problems and Educational Disruptions among Children in Out-of-Home Care in Chicago. Chicago: Chapin Hall; 2005. [Google Scholar]
- Stagner C, Lewis M. Agreement of parents, teachers, and children on internalizing and externalizing behavior problems. Journal of Clinical Child Psychology. 1993;22(1):107–115. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 9. College Station, TX: StataCorp LP; 2005. [Google Scholar]
- Sterba SK, Prinstein MJ, Cox MJ. Trajectories of internalizing problems across childhood: Heterogeneity, external validity, and gender differences. Development and Psychopathology. 2007;19:345–366. doi: 10.1017/S0954579407070174. [DOI] [PubMed] [Google Scholar]
- Straus MA, Hamby SL, Boney-McCoy S, Sugarman DB. The revised Conflict Tactics Scale (CTS2): Development and preliminary psychometric data. Journal of Family Issues. 1996;17(3):283–316. [Google Scholar]
- Taussig HN, Clyman RB, Landsverk J. Children who return home from foster care: A 6-year prospective study of behavioral health outcomes in adolescence. Pediatrics. 2001;108:e10. doi: 10.1542/peds.108.1.e10. [DOI] [PubMed] [Google Scholar]
- USDHHS (United States Department of Health and Human Services) The AFCARS report. 2006 Downloaded August 6, 2007 from: http://www.acf.hhs.gov/programs/cb/stats_research/afcars/tar/report13.pdf.
- Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Medical Care. 1996;34(3):220–233. doi: 10.1097/00005650-199603000-00003. [DOI] [PubMed] [Google Scholar]
- Wulczyn F. Family reunification. Future of Children. 2004;14:95–113. [PubMed] [Google Scholar]
- Wulczyn F, Lery B, Haight J. Entry and Exit Disparities in the Tennessee Foster Care System. Chicago: Chapin Hall; 2006. [Google Scholar]