

Abstract
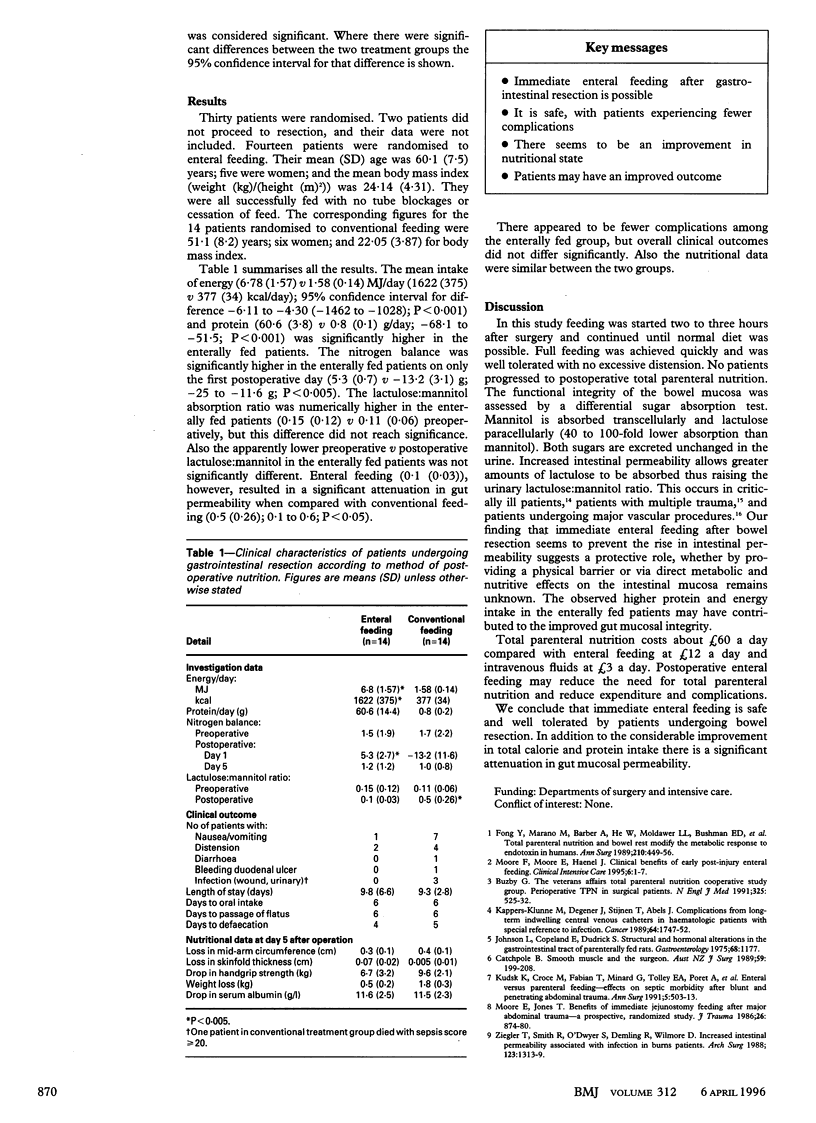
OBJECTIVES: To assess whether immediate post-operative enteral feeding in patients who have undergone gastrointestinal resection is safe and effective. DESIGN: Randomised trial of immediate post-operative enteral feeding through a nasojejunal tube v conventional postoperative intravenous fluids until the reintroduction of normal diet. SETTING: Teaching hospitals in London. SUBJECTS: 30 patients under the care of the participating consultant surgeon who were undergoing elective laparotomies with a view to gastrointestinal resection for quiescent, chronic gastrointestinal disease. Two patients did not proceed to resection. MAIN OUTCOME MEASURES: Nutritional state, nutritional intake and nitrogen balance, gut mucosal permeability measured by lactulose-mannitol differential sugar absorption test, complications, and outcome. RESULTS: Successful immediate enteral feeding was established in all 14 patients with a mean (SD) daily intake of 6.78 (1.57)MJ (1622 (375) kcal before reintroduction of oral diet compared with 1.58 (0.14) MJ (377 (34) kcal) for those on intravenous fluids (P < 0.0001). Urinary nitrogen balance on the first postoperative day was negative in those on intravenous fluids but positive in all 14 enterally fed patients (mean (SD) - 13.2 (11.6) g v 5.3 (2.7) g; P < 0.005). There was no difference by day 5. There was no change in gut mucosal permeability in the enterally fed group but a significant increase from the test ratios seen before the operation in those on intravenous fluids (0.11(0.06) v 0.15 (0.12); P < 0.005). There were also fewer postoperative complications in the enterally fed group (P < 0.005). CONCLUSIONS: Immediate postoperative enteral feeding in patients undergoing intestinal resection seems to be safe, prevents an increase in gut mucosal permeability, and produces a positive nitrogen balance.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- 2nd International Conference on Sepsis in the ICU. Maastricht, The Netherlands, 27-29 June, 1995. Abstracts. Clin Intensive Care. 1995;6(3 Suppl):1–22. [PubMed] [Google Scholar]
- Catchpole B. N. Smooth muscle and the surgeon. Aust N Z J Surg. 1989 Mar;59(3):199–208. doi: 10.1111/j.1445-2197.1989.tb01502.x. [DOI] [PubMed] [Google Scholar]
- Chiarelli A., Enzi G., Casadei A., Baggio B., Valerio A., Mazzoleni F. Very early nutrition supplementation in burned patients. Am J Clin Nutr. 1990 Jun;51(6):1035–1039. doi: 10.1093/ajcn/51.6.1035. [DOI] [PubMed] [Google Scholar]
- Elebute E. A., Stoner H. B. The grading of sepsis. Br J Surg. 1983 Jan;70(1):29–31. doi: 10.1002/bjs.1800700111. [DOI] [PubMed] [Google Scholar]
- Fong Y. M., Marano M. A., Barber A., He W., Moldawer L. L., Bushman E. D., Coyle S. M., Shires G. T., Lowry S. F. Total parenteral nutrition and bowel rest modify the metabolic response to endotoxin in humans. Ann Surg. 1989 Oct;210(4):449–457. doi: 10.1097/00000658-198910000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris C. E., Griffiths R. D., Freestone N., Billington D., Atherton S. T., Macmillan R. R. Intestinal permeability in the critically ill. Intensive Care Med. 1992;18(1):38–41. doi: 10.1007/BF01706424. [DOI] [PubMed] [Google Scholar]
- Kappers-Klunne M. C., Degener J. E., Stijnen T., Abels J. Complications from long-term indwelling central venous catheters in hematologic patients with special reference to infection. Cancer. 1989 Oct 15;64(8):1747–1752. doi: 10.1002/1097-0142(19891015)64:8<1747::aid-cncr2820640832>3.0.co;2-f. [DOI] [PubMed] [Google Scholar]
- Moore E. E., Jones T. N. Benefits of immediate jejunostomy feeding after major abdominal trauma--a prospective, randomized study. J Trauma. 1986 Oct;26(10):874–881. doi: 10.1097/00005373-198610000-00003. [DOI] [PubMed] [Google Scholar]
- O'Dwyer S. T., Michie H. R., Ziegler T. R., Revhaug A., Smith R. J., Wilmore D. W. A single dose of endotoxin increases intestinal permeability in healthy humans. Arch Surg. 1988 Dec;123(12):1459–1464. doi: 10.1001/archsurg.1988.01400360029003. [DOI] [PubMed] [Google Scholar]
- Perioperative total parenteral nutrition in surgical patients. The Veterans Affairs Total Parenteral Nutrition Cooperative Study Group. N Engl J Med. 1991 Aug 22;325(8):525–532. doi: 10.1056/NEJM199108223250801. [DOI] [PubMed] [Google Scholar]
- Roumen R. M., van der Vliet J. A., Wevers R. A., Goris R. J. Intestinal permeability is increased after major vascular surgery. J Vasc Surg. 1993 Apr;17(4):734–737. doi: 10.1067/mva.1993.41204. [DOI] [PubMed] [Google Scholar]
- Schroeder D., Gillanders L., Mahr K., Hill G. L. Effects of immediate postoperative enteral nutrition on body composition, muscle function, and wound healing. JPEN J Parenter Enteral Nutr. 1991 Jul-Aug;15(4):376–383. doi: 10.1177/0148607191015004376. [DOI] [PubMed] [Google Scholar]
- Webb A. R., Newman L. A., Taylor M., Keogh J. B. Hand grip dynamometry as a predictor of postoperative complications reappraisal using age standardized grip strengths. JPEN J Parenter Enteral Nutr. 1989 Jan-Feb;13(1):30–33. doi: 10.1177/014860718901300130. [DOI] [PubMed] [Google Scholar]
- Ziegler T. R., Smith R. J., O'Dwyer S. T., Demling R. H., Wilmore D. W. Increased intestinal permeability associated with infection in burn patients. Arch Surg. 1988 Nov;123(11):1313–1319. doi: 10.1001/archsurg.1988.01400350027003. [DOI] [PubMed] [Google Scholar]