

Abstract
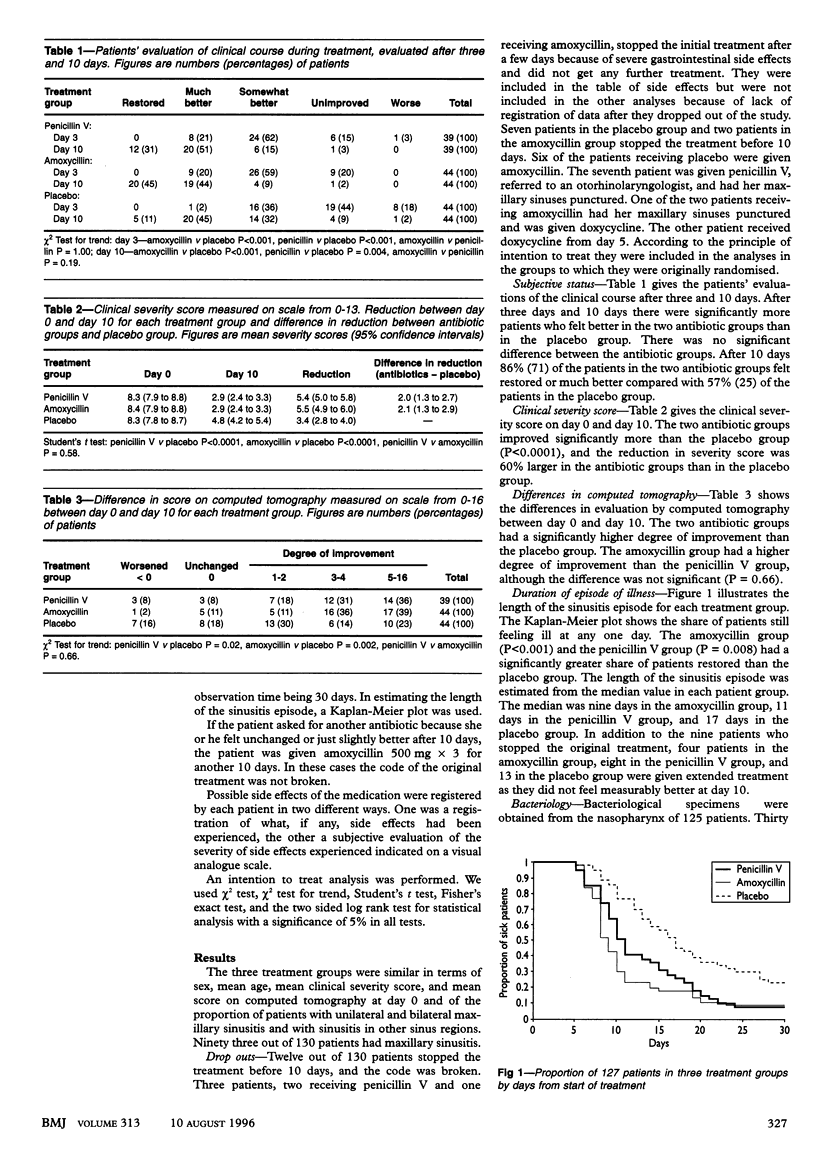
OBJECTIVES--To compare the effectiveness of penicillin V and amoxycillin with placebo in treatment of adult patients with acute sinusitis. DESIGN--Randomised, double blind, placebo controlled trial. SETTING--Norwegian general practice. SUBJECTS--130 adult patients with a clinical diagnosis of acute sinusitis confirmed by computed tomography. MAIN OUTCOME MEASURES--Subjective status after three and 10 days of treatment, difference in clinical severity score between day 0 and day 10 as evaluated by the general practitioner, difference in score from computed tomography on day 0 and day 10, and duration of sinusitis. RESULTS--Amoxycillin and penicillin V led to significantly faster and better recovery than placebo. By day 10, 71 patients receiving antibiotic treatment- (86%) considered themselves to be recovered or much better compared with 25 (57%) receiving placebo. The mean (95% confidence interval) reductions in clinical severity scores by day 10 were 5.4 (5.0 to 5.8) for penicillin V, 5.5 (4.9 to 6.0 for amoxycillin, and 3.4 (2.8 to 4.0) for placebo. For the antibiotic groups combined the number of patients with the greatest degree of improvement on computed tomography (scale 0-16)-that is, score 5-16 on day 10-was 31/83 (37%) compared with 10/44 (23%) receiving placebo. The median duration of the sinusitis was nine days in the amoxycillin group, 11 days in the penicillin V group, and 17 days in the placebo group. CONCLUSION--Penicillin V and amoxycillin are significantly more effective than placebo in the treatment of acute sinusitis.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Axelsson A., Chidekel N., Grebelius N., Jensen C. Treatment of acute maxillary sinusitis. A comparison of four different methods. Acta Otolaryngol. 1970 Jul;70(1):71–76. doi: 10.3109/00016487009181861. [DOI] [PubMed] [Google Scholar]
- Berg O., Carenfelt C. Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol. 1988 Mar-Apr;105(3-4):343–349. doi: 10.3109/00016488809097017. [DOI] [PubMed] [Google Scholar]
- Brett A. S. Does this patient have sinusitis? JAMA. 1994 Feb 16;271(7):502–503. [PubMed] [Google Scholar]
- Cooke L. D., Hadley D. M. MRI of the paranasal sinuses: incidental abnormalities and their relationship to symptoms. J Laryngol Otol. 1991 Apr;105(4):278–281. doi: 10.1017/s0022215100115609. [DOI] [PubMed] [Google Scholar]
- Hansen J. G., Schmidt H., Rosborg J., Lund E. Predicting acute maxillary sinusitis in a general practice population. BMJ. 1995 Jul 22;311(6999):233–236. doi: 10.1136/bmj.311.6999.233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Havas T. E., Motbey J. A., Gullane P. J. Prevalence of incidental abnormalities on computed tomographic scans of the paranasal sinuses. Arch Otolaryngol Head Neck Surg. 1988 Aug;114(8):856–859. doi: 10.1001/archotol.1988.01860200040012. [DOI] [PubMed] [Google Scholar]
- Laine F. J., Smoker W. R. The ostiomeatal unit and endoscopic surgery: anatomy, variations, and imaging findings in inflammatory diseases. AJR Am J Roentgenol. 1992 Oct;159(4):849–857. doi: 10.2214/ajr.159.4.1529853. [DOI] [PubMed] [Google Scholar]
- Lund V. J., Mackay I. S. Staging in rhinosinusitus. Rhinology. 1993 Dec;31(4):183–184. [PubMed] [Google Scholar]
- Stammberger H. Endoscopic endonasal surgery--concepts in treatment of recurring rhinosinusitis. Part I. Anatomic and pathophysiologic considerations. Otolaryngol Head Neck Surg. 1986 Feb;94(2):143–147. doi: 10.1177/019459988609400202. [DOI] [PubMed] [Google Scholar]
- Söderström M., Blomberg J., Christensen P., Hovelius B. Erythromycin and phenoxymethylpenicillin (penicillin V) in the treatment of respiratory tract infections as related to microbiological findings and serum C-reactive protein. Scand J Infect Dis. 1991;23(3):347–354. doi: 10.3109/00365549109024322. [DOI] [PubMed] [Google Scholar]
- Wald E. R., Chiponis D., Ledesma-Medina J. Comparative effectiveness of amoxicillin and amoxicillin-clavulanate potassium in acute paranasal sinus infections in children: a double-blind, placebo-controlled trial. Pediatrics. 1986 Jun;77(6):795–800. [PubMed] [Google Scholar]
- Williams J. W., Jr, Simel D. L. Does this patient have sinusitis? Diagnosing acute sinusitis by history and physical examination. JAMA. 1993 Sep 8;270(10):1242–1246. [PubMed] [Google Scholar]
- de Melker R. A., Kuyvenhoven M. M. Management of upper respiratory tract infection in Dutch general practice. Br J Gen Pract. 1991 Dec;41(353):504–507. [PMC free article] [PubMed] [Google Scholar]
- van Duijn N. P., Brouwer H. J., Lamberts H. Use of symptoms and signs to diagnose maxillary sinusitis in general practice: comparison with ultrasonography. BMJ. 1992 Sep 19;305(6855):684–687. doi: 10.1136/bmj.305.6855.684. [DOI] [PMC free article] [PubMed] [Google Scholar]