

Abstract
Although most eating occurs in a social context, the impact of peer influence on child food consumption and selection of healthy and unhealthy snacks has not been the object of systematic experimental study. The present experiment assessed the effects of peer interaction on energy intake and food choices in 18 overweight and 21 non-overweight youth. Participants had access to high and low-calorie food items and were provided with several games as alternatives to eating. On one occasion, participants were tested alone and on another occasion they were tested in dyads with an unfamiliar peer. Consistent with previous results, we found that overweight children ate substantially more when alone than when in the presence of a peer and also more when alone than the lean children in the same condition. Non-overweight youths' food intake was unaffected by the social context. Findings also indicated that the best predictor of whether participants consumed healthy snack foods was if the other youth in the dyad also consumed healthy snack foods. These findings suggest that the presence of peers can influence overweight children's energy intake and also influence healthier food selection in both overweight and non-overweight children.
Keywords: Social influence, Food selection, Children, Obesity
1. Introduction
Obesity results from positive energy balance in which energy intake exceeds expenditure. Snack foods are a major source of calories in most diets (Summerbell, Moody, Shanks, Stock, & Geissler, 1995) as they are often consumed in excess of energy needs. High energy density food consumption is cross-sectionally related to increased body weight (McCrory et al., 1999). A healthier substitute for snack foods would be to increase fruits and vegetables, which, in addition to reducing energy intake, may have positive health benefits (Block, Patterson, & Subar, 1992; Sacks et al., 1999). Thus, interventions that shift choice from high energy density snacks to healthier, lower energy density foods may reduce total energy intake, thereby enhancing the efficacy of obesity prevention and treatment.
A host of factors aside from physiological needs influence what children choose to eat. Noteworthy among these factors is the social environment (Birch & Fisher, 2000; Filozof & Gonzalez, 2000). Social influences and especially influence from parents and peers impact the development of children's food preferences. Research shows that which foods children choose to eat and how much they like them can be affected by the behavior of others. More precisely, studies indicate that children's preference for specific food items (e.g., a vegetable) can be increased as a result of repeated exposures to a peer or teacher eating the food (Addessi, Galloway, Visalberghi, & Birch, 2005; Birch, 1980; Duncker, 1938; Harper & Sanders, 1975; Hendy, 2002; Hendy & Raudenbush, 2000; Marinho, 1942).
Previous studies in our laboratory indicate that the presence of peers influences youth food intake. Our findings show that overweight youth eat substantially less when in company of peers than alone (Salvy, Coelho, Kieffer, & Epstein, in press) and eat more in the presence of overweight peers than in the presence of leaner peers (Salvy, Romero, Paluch, & Epstein, 2007). These findings suggest that the presence of peers can influence how much overweight children choose to eat. However, one area that has not been systematically studied is how the presence of peers influences child selection of nutrient-dense vs. energy-dense foods and whether peers promote healthier food selection in overweight and non-overweight children. Research shows that overweight youth are aware of weight stigmatization, (Neumark-Sztainer et al., 2002; Staffieri, 1967). A corollary of these prejudiced attitudes is that overweight individuals may suppress their food intake and also modify their food selection in front of others to avoid incurring the stigmas attributed to overweight individuals (Maykovich, 1978; Vartanian, Herman, & Polivy, 2007). Youth may also conform to others' level of intake because they believe that doing so will increase social approval (see Deutsch & Gerard, 1955 for the distinction between normative and informational conformity).
This study assesses how the presence of peers impacts food choices and food consumption in overweight and normal-weight youth. The aim is to understand differences in responses to the social and food environment between overweight and non-overweight youth, and to assess whether peer relationships can impact youths' eating behavior. We predicted that overweight participants would consume a greater number of kilocalories from energy-dense food items and eat an overall greater number of kilocalories when alone than when in the presence of another participant. We also predicted that normal-weight and overweight participants' consumption of healthy food items would predict the amount of healthy snacks the other participant in the dyad was eating. To our knowledge this is the first experimental study designed to examine the effects of peers on overweight and normal-weight youths' choices of healthy and unhealthy snacks.
2. Method
2.1. Overview and design
This study involved a mixed design with weight status (overweight vs. lean) as a between-subjects factor and social context (dyad vs. alone) as a within-subject factor. The order of the group and alone sessions was counterbalanced. Half of the participants were tested alone first and in group subsequently, while this order was reversed for the other half of the sample. For the dyad session, participants were tested in weight-discordant dyads (overweight participants paired with lean participants) or in weight-concordant dyad (lean/lean dyads and overweight/overweight dyads).
A cover story was used in order to avoid demand effects that might arise had participants been told that the experimenters were interested in investigating their food intake. Youths were told that the experimenters were interested in their liking of games and different foods. Children had free access to several games that can be played alone or in dyads and to sizeable portions of healthy (i.e., carrots and grapes) and unhealthy snack foods (i.e., chips and cookies). This procedure makes it possible to examine the mutual influence “freely-eating” individuals have on one another rather than using a confederate accomplice to the experimenter (see also Clendenen, Herman, & Polivy, 1994; de Castro, 1991; Herman, Koenig-Nobert, Peterson, & Polivy, 2005 for similar methodologies). This paradigm does not involve working on a task which might influence the participants' intake, such as a forced tasting task in which participants are required to at least taste the food offered.
All procedures were approved by the Children & Youth Institutional Review Board of the University at Buffalo. All applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research.
2.2. Participants
Participants for this study included 21 normal-weight (=85th BMI percentile) and 18 overweight or at risk of overweight (>85th BMI percentile) males (n=18) and females (n=21) between 10–12 years of age (Table 1). Twenty-two participants were tested in weight-discordant dyads (overweight participants paired with lean participants), sixteen participants were tested in weight-concordant dyad (10 lean/lean participants and 6 overweight/overweight participants). One participant only came for the alone session.
Table 1.
Mean BMI percentile and age (SD) of participants across conditions
| Male |
Female |
|||
|---|---|---|---|---|
| Age | BMI % | Age | BMI % | |
| Overweight (n = 18) | 11.0 (0.7) | 95.4 (2.5) | 11.6 (0.7) | 94.3 (2.9) |
| Normal-weight (n = 21) | 11.1 (0.7) | 38.2 (19.7) | 11.6 (0.9) | 42.4 (20.0) |
Height and weight were measured by a trained staff. Youth weight was assessed with a digital scale calibrated daily and height was assessed using a SECA stadiometer. On the basis of the height and weight data, the BMI was calculated according to the following formula: BMI = kg/m2. The BMI-for-age percentile (z-score BMI, zBMI) was further used to interpret the BMI number because BMI is both age- and sex-specific for children and teens. These criteria are different from those used to interpret BMI for adults, which do not take into account age or sex. Age and sex are considered for children and because the amount of body fat changes with age and the amount of body fat differs between girls and boys (Kuczmarski et al., 2002). Youth were considered overweight or at risk for becoming overweight if they are above the 85th BMI percentile and were considered non-overweight if below the 85th BMI percentile for their age and sex (Ogden et al., 2002). These are the current guidelines for weight in children and adolescents set forth by the Centers for Disease Control (Kuczmarski et al., 2002).
Families were recruited from newspaper ads and from our database of families who have volunteered for previous laboratory studies. Parents were screened by phone for their child's height, weight, a brief medical history, and ethnic background. Children were excluded if they were below the 10th BMI percentile; had a cold or upper respiratory distress, which could influence olfactory and/or taste cues; current psychopathology or developmental disability; allergies to the study food; or were taking medications that could influence taste, appetite or olfactory sensory responsiveness (e.g. methylphenidate). If children met basic entry criteria, they were scheduled to come to the laboratory.
During the phone screening, parents were informed that the study would evaluate children's liking of different foods and games during two separate visits to the laboratory. It was explained that one session would involve another child of the same age and gender (dyad condition), while for the other session their child would be alone to eat the food offered and play the games (alone condition). It was also explained that children would have access to a variety of snack foods and drinks and would also have access to several leisure activities during the session. Parents were instructed that the study required participants to abstain from eating for at least 2 h before the experimental sessions. The nutritional information of the foods was provided upon request to allow parents to consider allergy or dietary concerns.
2.3. Procedure
Upon arrival to the laboratory, all children heard an “assent” script and were asked if they were willing to take part in the study; parents were also asked to read and provide written consent. Participants completed a same day recall of their food intake, with the help of their parents if needed, to ensure they had followed the eating recommendations and had refrained from consuming solid foods in the 2 h prior to their arrival. At the beginning of each session, participants completed a hunger scale and a scale assessing their liking of study foods. The participants and their parents were then shown the experimental room and they were asked to read and provide assent and consent.
The experimental room included two areas: an eating area and a play area. The eating area was equipped with a table with a pitcher of water and the bowls of snack foods (described below). The play area included three bean bag chairs, board games, a DVD player, a video game console and age-appropriate movies, books, puzzles and video games. All activities could be played alone or with other children. These activities were provided as alternatives to eating so participants did not feel obligated to eat. Participants were instructed that they could alternate between the eating and the play areas.
Height and weight measurements were obtained by a trained staff at the end of the second session so that these measurements did not influence the data. Parents were also asked to complete a demographics questionnaire. Lastly, children and parents were debriefed and they received a $30 gift card for a shopping mall of their choice for their participation.
2.4. Foods
Participants had access to two energy-dense and two nutrient-dense foods (Table 2). These foods are liked by children within the age range studied in this experiment (Temple, Giacomelli, Roemmich, & Epstein, in press). These items were presented in large bowls (20-ounce) to avoid any reference to portion size cues which could have influenced youths' food intake. Each participant was given individual pre-weighed bowls of snacks. For the social session (i.e., dyads), they were asked not to share their bowls with the other participant. The bowls were replenished as needed to avoid limiting children's food consumption. Participants were also provided with 8 oz cups of fresh water and a 1.5 L pitcher of water to refill their cups as needed.
Table 2.
Characteristics of the experimental foods used in the experiment
| Foods | Portion (g) | Kilocalories | Fat (g) | Carbohydrates (g) | Protein (g) |
|---|---|---|---|---|---|
| Nutrient dense | |||||
| Baby carrots | 250 | 103 | <1 | 26 | 3 |
| Grapes | 250 | 178 | <1 | 44 | 2 |
| Energy dense | |||||
| Potato chips (Frito-lay™) | 80 | 429 | 29 | 43 | 6 |
| Mini Oreo cookies (Nabisco™) | 125 | 560 | 26 | 91 | 4 |
2.5. Analytic plan
This study evaluates how the presence of a peer impacts overweight and normal-weight youths' food selection and food consumption. The main variables of interest are the participants' total energy intake and the participant's energy intake of nutrient- and energy-dense foods in kilocalories. Treatment of these data requires accounting for multiple observations within individuals (i.e., two sessions) as well as dyadic analysis. The mutual influence violates the assumption of independence between observations required for analysis of variance.
Random-effect models (also called multilevel, hierarchical linear or mixed models) provide a useful approach to account for interdependence in multiple observations within individuals and in two-person relationships (Gibbons & Hedeker, 1994; Hedeker & Gibbons, 1994; Hedeker, Gibbons, & Flay, 1994). Mixed models assume that the data within clusters are dependent among the observations. This is determined by the covariances among the regression coefficients and can be characterized by a covariance function (Hedeker & Gibbons, 1996). The outcomes at the individual level are modeled taking into consideration the dependence of observations within individuals or within dyads (Hedeker, 2003). These models allow simultaneously estimating the parameters of the regression model and the variance components that account for the data clustering (Gibbons & Hedeker, 1994).
The data were stacked following the Double Entry Method developed by Kenny (Kenny, 1995; Kenny & Judd, 1986; Kenny, Kashy, & Cook, 2006). Each participant was entered twice: once as a “partner” and once as a “participant”, hence the name of double entry. Mixed model analyses, using SAS Software (SAS, 2002), were then used to analyze these data. Three separate models assessed the effects of participants' zBMI and participants gender as time invariant predictors, the peers' zBMI, the peers' consumption, the social condition and the order of the sessions (alone first vs. dyad first) as time variant variables, as well as interactions between these terms on the participants' total caloric intake, the consumption of high and the intake of low-energy density foods in kilocalories. For all models, predictors were first entered into the model and non-significant variables were removed to identify the best fitting model.
3. Results
3.1. Participant characteristics
There were no significant differences between groups for the amount eaten prior to coming to the laboratory, based on participants' same day food recalls, and no difference in hunger or liking of the study foods (all p's> .15). In this study, 18% of the sample was minority, with 7% African–American and 11% Hispanic or Latino.
3.2. Total snack intake in kilocalories
Participants' total snack consumption was predicted by the interaction of zBMI by Condition, F(1,37)=5.95, p<0.05 (Fig. 1). Consistent with our prediction, differences of least square means revealed that when they were alone, overweight children consumed more kilocalories, M=519.41 SE=81.5, than when they were with an unfamiliar peer, M= 359.13, SE=50.29 (d=0.56; 95%CI: −0.13 to 1.24), more kilocalories than normal-weight children alone, M=319.87, SE=47.57 (d=0.70; 95%CI: 0.04 to 1.37), and also more than normal-weight children in group M=348.59, SE=52.71 (d=0.58; 95%CI: −0.08 to 1.24). Neither peers' zBMI nor the interaction of peers' zBMI by participants zBMI were significant predictors of participants' total energy intake (p=0.44 and p=0.59 respectively).
Fig. 1.
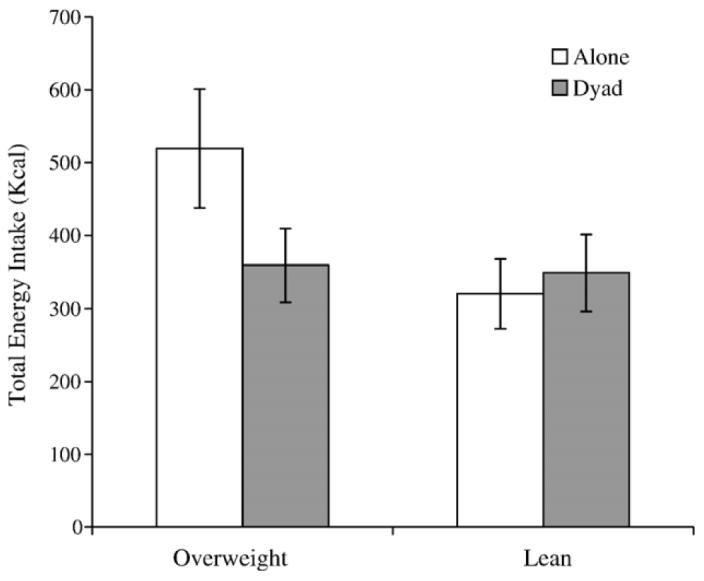
Amount of food consumed (SD) across conditions.
3.3. Healthy vs. unhealthy snack intake in kilocalories
Fig. 2. illustrates the participants' consumption of healthy snack foods. As predicted, participants' consumption of healthy snacks was predicted by their partner's consumption of healthy snack, F(1,36)=26.07, p<0.0001. Overweight children also consumed more energy from healthy snacks, M=117.52, SE=12.34, than normal-weight children, M=76.47, SE=10.38; F(1,36)=7.32, p<0.05 (d=0.60; 95%CI: −0.06 to 1.26). The only significant predictor of participants' consumption of unhealthy snacks was the interaction of participants' zBMI by Condition F(1,37)=6.08, p<0.05. When alone, overweight participants ate more energy from unhealthy snacks, M=398.91, SE=67.04, than when in the presence of a peer, M=244.58, SE=43.6 (d=0.64; 95%CI: −0.04 to 1.34) and also more than lean participants alone, M=248.88, SE=43.3 (d=0.62; 95%CI: −0.04 to 1.28). Participants' gender was not a significant predictor of healthy (p=0.11) or unhealthy (p=0.10) snack foods intake. Peers' weight status was not a significant predictor of participants' consumption of healthy snacks (p=0.63) or unhealthy snack intake (p= 0.64).
Fig. 2.
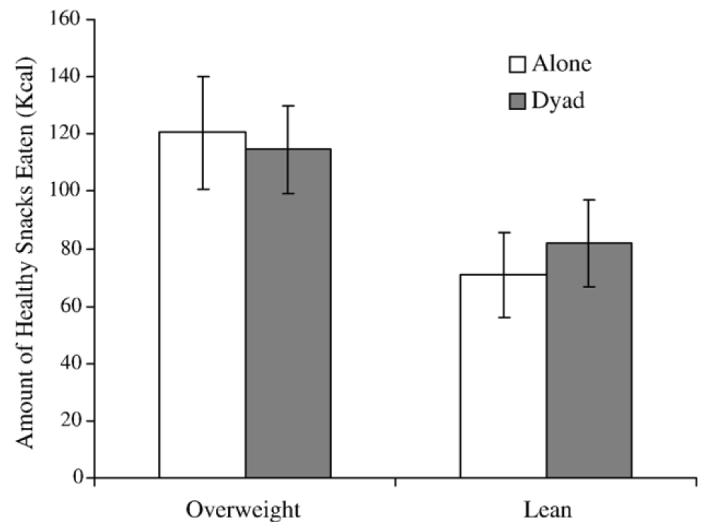
Amount of healthy snack foods consumed (SD) across conditions.
4. Discussion
This study examined how the presence of peers impacts food consumption of healthy and unhealthy snacks in overweight and normal-weight youth. Consistent with previous results, we found that overweight children ate substantially more when alone than when in the presence of a peer and also more when alone than the lean children in the same condition. Non-overweight youths' food intake was unaffected by the social context. Our findings also indicated that participants' consumption of healthy food items was predicted by whether the other participant in the dyad was also eating healthy snacks, whereas this was not the case for unhealthy snacks. To our knowledge, this is the first study to show a relationship between peers' consumption of healthy food.
Research shows that overweight youths are aware of weight stigmatization, (Neumark-Sztainer et al., 2002; Staffieri, 1967) and a corollary of these prejudiced attitudes is that overweight individuals may modify their food selection in front of others to avoid incurring the stigmas attributed to overweight individuals (e.g., Maykovich, 1978; Vartanian et al., 2007) and also because they believe that doing so will increase social approval (see Deutsch & Gerard, 1955 for the distinction between normative and informational conformity). The present results support this possibility in indicating that overweight participants consumed less unhealthy snacks in the presence of an unfamiliar peer than when alone. However, both normal-weight and overweight children's consumption of healthy food snacks was related to their partners' intake of healthy food snacks.
This study is not without limitations. First, all dyads were composed of unfamiliar peers. Had the dyads been composed of friends, the pattern of results may have differed. Research with adults indicates that the familiarity between co-eaters influences the amount of food consumed (Clendenen, Herman, & Polivy, 1994; Salvy, Jarrin, Paluch, Irfan, & Pliner, 2007). The fact that all groups were composed of strangers makes it impossible to determine whether the presence of others per se or the presence of an unfamiliar peer accounted for children's food consumption and selection. Second, although we had a heterogeneous sample in terms of ethnicity, the sample was relatively small. Therefore, these findings may not generalize to youth from other geographic regions and the limited scope of this study prevents generalizing beyond the children who participated in the study and replication with independent samples is necessary. Nevertheless, the data depict a coherent pattern of results which suggest new directions for research in the area of peer influence on overweight children's eating behavior.
Research on the impact of peer influences on eating may be relevant for understanding factors that influence food choice and therefore may have important implications for obesity treatment and prevention or for improving healthy eating for disease prevention. Over the last decades we have witnessed changes in the social context of eating, with a trend away from family meals towards grazing and eating alone. This increase in solitary eating has paralleled the increase in the obesity rate in children (Westenhoefer, 2002). Parents mediate the exposure and accessibility of food and also provide for modeling of eating behavior and teaching of portion size (Klesges, Stein, Eck, Isbell, & Klesges, 1991). Similarly, peers and friends may act as a guide of what is appropriate to eat and, in turn, operate as a brake and set the limit on youths' snack consumption (Herman, Fitzgerald, & Polivy, 2003). The present findings suggest that interventions involving peers may shift choice from high energy density snacks to healthier, lower energy density foods and reduce total energy intake, thereby enhancing the efficacy of obesity prevention and treatment. On the other hand, limited social interactions due to weight stigmatization and prejudicial attitudes may deprive overweight children from the normative influence of peers. Future research ought to test whether increased social involvement can be used as a tool for lifestyle changes in overweight children. Exploring social factors that influence the choice of snack foods and additional healthy nonfood alternatives, such as physical activity as well as alternative activities incompatible with eating, may be an important area of study for health psychology researchers (Epstein & Saelens, 2000).
Acknowledgement
This work was supported by National Institute of Child Health and Human Development grant RHD056059A awarded to Dr. Salvy.
Footnotes
Publisher's Disclaimer: This article was published in an Elsevier journal. The attached copy is furnished to the author for non-commercial research and education use, including for instruction at the author's institution, sharing with colleagues and providing to institution administration.
References
- Addessi E, Galloway AT, Visalberghi E, Birch LL. Specific social influences on the acceptance of novel foods in 2–5-year-old children. Appetite. 2005;45:264–271. doi: 10.1016/j.appet.2005.07.007. [DOI] [PubMed] [Google Scholar]
- Birch LL. Effects of peer models' food choices and eating behaviors on preschoolers' food preferences. Child Development. 1980;51:489–496. [Google Scholar]
- Birch LL, Fisher JO. Mothers' child-feeding practices influence daughters' eating and eight. American Journal of Clinical Nutrition. 2000;71:1054–1061. doi: 10.1093/ajcn/71.5.1054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Block G, Patterson B, Subar A. Fruits, vegetables, and cancer prevention: The epidemiological evidence. Nutrition and Cancer. 1992;18:1–29. doi: 10.1080/01635589209514201. [DOI] [PubMed] [Google Scholar]
- Clendenen VI, Herman CP, Polivy J. Social facilitation of eating among friends and strangers. Appetite. 1994;23:1–13. doi: 10.1006/appe.1994.1030. [DOI] [PubMed] [Google Scholar]
- de Castro JM. Social facilitation of the spontaneous meal size of humans occurs on both weekdays and weekends. Physiology & Behavior. 1991;49:1289–1291. doi: 10.1016/0031-9384(91)90365-u. [DOI] [PubMed] [Google Scholar]
- Deutsch M, Gerard H. A study of normative and informational influences upon individual judgment. Journal of Abnormal and Social Psychology. 1955;51:629–636. doi: 10.1037/h0046408. [DOI] [PubMed] [Google Scholar]
- Duncker K. Experimental modification of children's food preferences through social suggestion. Journal of Abnormal and Social Psychology. 1938;33:489–507. [Google Scholar]
- Epstein LH, Saelens BE. Behavioral economics of obesity: Food intake and energy expenditure. In: Bickel WK, Vuchinich RE, editors. Reframing health behavior change with behavioral economics. Lawrence Erlbaum Associates; Mahwah NJ: 2000. pp. 293–311. [Google Scholar]
- Filozof C, Gonzalez C. Predictors of weight gain: The biological–behavioural debate. Obesity Reviews. 2000;1:21–26. doi: 10.1046/j.1467-789x.2000.00005.x. [DOI] [PubMed] [Google Scholar]
- Gibbons RD, Hedeker D. Application of random-effects probit regression models. Journal of Consulting and Clinical Psychology. 1994;62:285–296. doi: 10.1037//0022-006x.62.2.285. [DOI] [PubMed] [Google Scholar]
- Harper LV, Sanders KM. The effects of adults' eating on young children's acceptance of unfamiliar foods. Journal of Experimental Child Psychology. 1975;20:206–214. [Google Scholar]
- Hedeker D. A mixed-effects multinomial logistic regression model. Statistics in Medicine. 2003;22:1433–1446. doi: 10.1002/sim.1522. [DOI] [PubMed] [Google Scholar]
- Hedeker D, Gibbons RD. A random-effects ordinal regression model for multilevel analysis. Biometrics. 1994;50:933–944. [PubMed] [Google Scholar]
- Hedeker D, Gibbons RD. MIXOR: A computer program for mixed-effects ordinal regression analysis. Computer Methods and Programs in Biomedicine. 1996;49:157–176. doi: 10.1016/0169-2607(96)01720-8. [DOI] [PubMed] [Google Scholar]
- Hedeker D, Gibbons RD, Flay BR. Random-effects regression models for clustered data with an example from smoking prevention research. Journal of Consulting and Clinical Psychology. 1994;62:757–765. doi: 10.1037//0022-006x.62.4.757. [DOI] [PubMed] [Google Scholar]
- Hendy HM. Effectiveness of trained peer models to encourage food acceptance in preschool children. Appetite. 2002;39:217–225. doi: 10.1006/appe.2002.0510. [DOI] [PubMed] [Google Scholar]
- Hendy HM, Raudenbush B. Effectiveness of teacher modeling to encourage food acceptance in preschool children. Appetite. 2000;34:61–76. doi: 10.1006/appe.1999.0286. [DOI] [PubMed] [Google Scholar]
- Herman CP, Fitzgerald NE, Polivy J. The influence of social norms on hunger ratings and eating. Appetite. 2003;41:15–20. doi: 10.1016/s0195-6663(03)00027-8. [DOI] [PubMed] [Google Scholar]
- Herman CP, Koenig-Nobert S, Peterson JB, Polivy J. Matching effects on eating: Do individual differences make a difference? Appetite. 2005;45:108–109. doi: 10.1016/j.appet.2005.03.013. [DOI] [PubMed] [Google Scholar]
- Kenny DA. The effect of nonindependence on significance testing in dyadic research. Personal Relationships. 1995;2:67–75. [Google Scholar]
- Kenny DA, Judd CA. Consequences of violating the independence assumption in analysis of variance. Psychological Bulletin. 1986;99:422–431. [Google Scholar]
- Kenny DA, Kashy DA, Cook WL. The analysis of dyadic data. Guilford Press; New York: 2006. [Google Scholar]
- Klesges RC, Stein RJ, Eck LH, Isbell TR, Klesges LM. Parental influence on food selection in young children and its relationships to childhood obesity. American Journal of Clinical Nutrition. 1991;53:859–864. doi: 10.1093/ajcn/53.4.859. [DOI] [PubMed] [Google Scholar]
- Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, et al. CDC Growth Charts for the United States: Methods and development. Vital and health statistics. 2002;11(246) (Vol. 11): Data from the national health survey. [PubMed] [Google Scholar]
- Marinho H. Social influence in the formation of enduring preferences. Journal of Abnormal and Social Psychology. 1942;37:448–468. [Google Scholar]
- Maykovich MK. Social constraints in eating patterns among the obese and overweight. Social Problems. 1978;25:453–460. [Google Scholar]
- McCrory MA, Fuss PJ, McCallum JE, Yao M, Vinken AG, Hays NP, et al. Dietary variety within food groups: Association with energy intake and body fatness in men and women. American Journal of Clinical Nutrition. 1999;69:440–447. doi: 10.1093/ajcn/69.3.440. [DOI] [PubMed] [Google Scholar]
- Neumark-Sztainer D, Falkner N, Story M, Perry C, Hannan PJ, Mulert S. Weight-teasing among adolescents: Correlations with weight status and disordered eating behaviors. International Journal of Obesity and Related Metabolic Disorders. 2002;26:123–131. doi: 10.1038/sj.ijo.0801853. [DOI] [PubMed] [Google Scholar]
- Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R, et al. Centers for Disease Control and Prevention 2000 growth charts for the United States: Improvements to the 1977 National Center for Health Statistics version. Pediatrics. 2002;109:45–60. doi: 10.1542/peds.109.1.45. [DOI] [PubMed] [Google Scholar]
- Sacks FM, Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, et al. A dietary approach to prevent hypertension: A review of the Dietary Approaches to Stop Hypertension (DASH) study. Clinical Cardiology. 1999;22(Suppl 7):III6–III10. doi: 10.1002/clc.4960221503. [DOI] [PubMed] [Google Scholar]
- Salvy SJ, Coelho JS, Kieffer E, Epstein LH. Effects of social contexts on overweight and normal-weight children's food intake. Physiology and Behavior. doi: 10.1016/j.physbeh.2007.06.014. in press. doi:10.1016/j.physbeh.2007.06.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salvy SJ, Jarrin D, Paluch R, Irfan N, Pliner P. Effects of social influence on eating in couples, friends and strangers. Appetite. 2007;49:92–99. doi: 10.1016/j.appet.2006.12.004. [DOI] [PubMed] [Google Scholar]
- Salvy SJ, Romero N, Paluch R, Epstein LH. Peer influence on pre-adolescent girls' snack intake: Effects of weight status. Appetite. 2007;49:177–182. doi: 10.1016/j.appet.2007.01.011. [DOI] [PubMed] [Google Scholar]
- SAS . SAS 9.1 (Version 9.1.3 Service Pack 4) SAS Institute Inc.; Cary, NC: 2002. [Google Scholar]
- Staffieri JR. A study of social stereotype of body image in children. Journal of Personality and Social Psychology. 1967;7:101–104. doi: 10.1037/h0021227. [DOI] [PubMed] [Google Scholar]
- Summerbell CD, Moody RC, Shanks J, Stock MJ, Geissler C. Sources of energy from meals versus snacks in 220 people in four age groups. European Journal of Clinical Nutrition. 1995;49:33–41. [PubMed] [Google Scholar]
- Temple JL, Giacomelli AM, Roemmich JN, Epstein LH. Dietary variety impairs habituation in children. Health Psychology. doi: 10.1037/0278-6133.27.1. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vartanian LR, Herman CP, Polivy J. Consumption stereotypes and impression management: How you are what you eat. Appetite. 2007;48:265–277. doi: 10.1016/j.appet.2006.10.008. [DOI] [PubMed] [Google Scholar]
- Westenhoefer J. Establishing dietary habits during childhood for long-term weight control. Annals of Nutrition & Metabolism. 2002;46:18–23. doi: 10.1159/000066396. [DOI] [PubMed] [Google Scholar]