

Abstract
A phase II trial was performed to determine the antitumour efficacy and tolerance of combined paclitaxel and cisplatin with or without hematopoetic growth factor support in patients with advanced gastric cancer. Forty-five patients with histologically confirmed metastatic gastric cancer were entered in this trial. Treatment consisted of 2-weekly courses of paclitaxel 160 mg per m2 and cisplatin 60 mg per m2 both given on day 1. Depending on absolute neutrophil counts on the days of scheduled chemotherapeutic drug administration (1000–2000 per μl), a 5-day course of human granulocyte colony-stimulating factor 5 μg kg−1 per day was given subcutaneously; in addition, if haemoglobin was <12.0 mg dl−1, erythropoietin 10 000 IU was administered subcutaneously three times per week. The confirmed overall response rate (intent-to-treat) was 44%, including five complete (11%) and 15 partial remissions (33%). Twelve patients had stable disease (27%), 11 (24%) progressed while on chemotherapy, and two patients were not evaluable. The median time to response was 3 months, the median time to progression 7.0 months, and the median survival time was 11.2 months with 12 patients currently alive. Haematologic toxicity was common, though WHO grade 4 neutropenia occurred in only five patients (11%). Apart from total alopecia in 16 patients (36%), severe non-haematologic adverse reactions included grade 3 peripheral neuropathy in six (13%) and anaphylaxis in two patients. In addition, there was one patient each who experienced grade 3 emesis, diarrhea, and infection, respectively. Our data suggest that the combination of paclitaxel and cisplatin with or without G-CSF and/or erythropoietin has promising therapeutic activity in patients with advanced gastric cancer.
British Journal of Cancer (2002) 86, 1858–1863. doi:10.1038/sj.bjc.6600345 www.bjcancer.com
Keywords: palliative chemotherapy, paclitaxel, cisplatin, human granulocyte colony-stimulating factor, erythropoietin, gastric cancer
Despite its declining incidence in the Western world, gastric cancer is still amongst the most common malignancies (Landis et al, 1998). Cytotoxic chemotherapy has been widely used in patients with advanced or metastatic gastric cancer and has been demonstrated to be effective in the palliative management of this disease. In randomised trials, in fact, a significant improvement in overall survival and in quality of life was noted when compared to best supportive care alone (Pyrhonen et al, 1995; Scheithauer et al, 1995; Glimelius et al, 1997). Although several second generation combination regimens that have been developed in the 1980s–including epirubicin/adriamycin/cispatin (EAP), fluorouracil/adriamycin/methotrexate (FAMTX), etoposide/leukovorin/ fluorouracil (ELF), and infusional fluorouracil/cisplatin (FUP)–were reported to result in rather high objective response rates, randomised trials have generally failed to reproduce these data and thus demonstrate a substantial change in the natural course of advanced disease (Wils, 1996; Fuchs, 1997). Only the ECF-regimen (epirubicin, cisplatin and infusional fluorouracil) showed a superior response rate (46% vs 21%) and prolonged survival (8.9 vs 5.7 months) compared with FAMTX (Webb et al, 1997), and thus made it a sort of standard chemotherapy. Still, the identification of new agents and/or drug combinations with a superior therapeutic index remains a principal goal of investigational efforts. Because chemotherapy use in patients with disseminated disease, who fare particularly poorly, is aimed at producing palliative effects, the anticancer activity and side effects must be weighted carefully. The results of recently published trials in patients with metastatic gastric carcinomas have suggested that both cisplatin and paclitaxel are relatively active and well tolerated drugs. Cisplatin has been used in the treatment of gastric cancer in the neoadjuvant, adjuvant and palliative setting and various combination regimens have been reported to show response rates between 20–71% (Findlay et al, 1994; Wils, 1996; Morant, 2001). Paclitaxel is a novel antineoplastic drug with the unique cytotoxic mechanism of tubulin stabilisation and polymerisation (Arbuck, 1994). It has demonstrated broad clinical activity in a variety of malignancies both alone and in combination regimens. Antitumour activity of paclitaxel also has been shown in gastric cancer cell lines and in several phase I/II trials (Arbuck, 1994; Bokemeyer et al, 1997; Murad et al, 1999; Kollmannsberger et al, 2000; Safran et al, 2000). Paclitaxel is usually well tolerated with myelosuppression being the dose-limiting toxicity and patients receiving this agent can be treated on an outpatient basis.
Favourable results were obtained when both drugs were combined in patients with ovarian cancer, advanced non-small cell lung cancer (NSCLC), head and neck- and oesophageal carcinomas (Ilson et al, 1998; Khuri et al, 2000; Gatzemeier et al, 2000; Pfisterer, 2000). Furthermore, two recently published phase II studies, investigating the combination of cisplatin with docetaxel, a semisynthetic taxoid, suggested a high antitumour activity with an overall response rate of 37 and 56%, respectively (Roth et al, 2000; Ridwelski et al, 2001).
The aim of the present study was thus to evaluate the antitumour activity and tolerance of paclitaxel plus cisplatin in chemotherapy-naive patients with disseminated gastric cancer. To minimise acute toxicities and counteract myelosuppression that was likely to constitute the dose-limiting toxicity with this combination, we decided to use a biweekly administration schedule of paclitaxel and cisplatin. A potentially improved therapeutic index despite dose intenification by using fractionated, i.e., weekly or biweekly drug dose regimens has been reported in other malignancies, including NSCLC (Brunn, 1997; Soerensen et al, 1997). The particular dose regimen used in this trial was based on the results of a previous phase I study in patients with advanced oesophageal cancer (Van der Gaast et al, 1997). In addition, to maintain the planned dose intensity, granulocyte colony-stimulating factor (G-CSF) was given depending on absolute neutrophil counts on the days of scheduled chemotherapeutic drug administration. Since recent data suggest that erythropoietin, apart from its ability to potentiate the effect of G-CSF, significantly improves quality of life in cancer patients receiving cisplatin and non-platinum chemotherapy with a possible beneficial effect in terms on overall survival, we decided to co-administer this haematopoetic growth factor in patients with haemoglobin levels below 12 mg μL−1 (Pierelli et al, 1999; Littlewood, 2001).
PATIENTS AND METHODS
Patients selection
Patients eligible for this study had histologically confirmed advanced gastric cancer (except carcinomas of the oesophagastric junction) with bidimensionally measurable disease not previously treated with palliative chemotherapy and not amenable to curative resection. All patients were required to be 75 years old or younger, to have a World Health Organisation (WHO) performance status of less than 3, to have an expected survival time of more than 12 weeks, and to have adequate bone marrow (absolute neutrophil count (ANC) ⩾2.000 per μL, and platelet count ⩾100 000 per μL), adequate renal (serum creatinine concentration <132 μmol, creatinine clearance ⩾70 ml min−1 as calculated by the Calvert formula), and adequate hepatic function (bilirubin and serum transaminase level <2 times the upper limit of normal). Patients were ineligible if they had a history of prior or concomitant malignancy, except for curatively treated nonmelanoma skin cancer or in situ cervical cancer. Female patients could not be pregnant or lactating. A prior history of atrial or ventricular arrhythmias and/or history of congestive heart failure, even when medically controlled, disqualified patients from study entry. Pre-existing motor or sensory neurologic symptoms ⩾WHO grade 2 were not allowed, nor were active infections or other serious underlying medical conditions that would impair the ability of the patient to receive protocol treatment. All patients gave written informed consent according to institutional regulations.
Treatment protocol
Chemotherapy consisted of paclitaxel (Taxol®, Bristol-Myers Squibb Company, Princeton, NJ, USA) 160 mg per m2, dissolved in 500 ml of normal saline and given as a 3 h infusion plus cisplatin 60 mg per m2, diluted in 500 ml normal saline and administered as 1 h infusion. Pre- and post-hydration with at least 2000 ml of intravenous fluid (normal saline or 5% dextrose per 24 h) were mandatory. The recommended prophylactic anti-emetic medication consisted of dexamethasone and 5-hydroxytryptamine-3 antagonists. Before paclitaxel administration, each patient received premedication including dexamethasone (20 mg orally, 12 and 6 h before paclitaxel), cimetidine (300 mg i.v., 30 min before paclitaxel), and diphenhydramine (50 mg i.v., 30 min before paclitaxel). Treatment courses were repeated every 2 weeks, and were to be continued in patients achieving complete or partial remission or stabilisation of disease for a total of 12 courses. Depending on absolute neutrophil counts on the days of scheduled chemotherapeutic drug administration (1000–2000 per μL), a 5-day course of human granulocyte colony-stimulating factor (G-CSF, Neupogen®, Amgen Europe, Netherlands) 5 μg kg−1 per day was given. In addition, if haemoglobin was <12.0 mg dl−1 erythropoietin 10 000 IU (ERYPO®, Janssen-Cilag Pharma, Austria) was administered s.c. three times per week until a haemoglobin level >13.5 mg dl−1 has been reached.
Toxicity and dosage modification guidelines
Adverse reactions were evaluated according to WHO standard criteria. Treatment could be delayed for up to 2 weeks if the ANC was lower than 1000 per μL and/or platelet count was lower than 75 000 per μL. Prolonged administrations of G-CSF (until the neutrophil count was ⩾2000 per μL) was recommended in the former group of patients. Drug doses were reduced by 25% in case of febrile neutropenia grade 4, if the lowest platelet count was less than 25 000 per μL, in case of grade 1 nephrotoxicity or grade 2 neuropathy, or if any severe (>WHO grade 2) non-haematologic toxicity was observed in the previous cycle. Paclitaxel was stopped in any case of grade 4 skin toxicity and grade 3 anaphylactic reaction. Both chemotherapeutic drugs were discontinued in the event of transitory ⩾ grade 2 renal toxicity or definitive decrease of creatinine clearance (<60 ml min−1), ⩾ grade 3 neuropathy, and if severe toxicity recurred despite dose attenuation. Similarly, any patient who required more than 2 weeks for full recovery of adverse reactions (except alopecia and mild neuropathy) was taken off study.
Pretreatment and follow-up evaluation
Pretreatment evaluation included a complete medical history and physical examination, routine haematology and biochemistry analyses, ECG, chest X-ray, and CT scans to define the extent of disease. Complete blood counts and differential counts were obtained weekly, and biochemical profiles were assessed before each treatment cycle. Measurable lesions were reassessed every 8 weeks by CT scan, X-ray, or any other technique that allows retrospective and independent evaluation.
Assessment of response
The primary efficacy endpoint of this trial was objective response rate, which was evaluated according to WHO standard criteria. In addition, complete remission (CR) of the primary tumour site was defined as a normal appearing stomach on CT-scan with complete resolution of the endoscopically visible tumour and a negative biopsy of the original site of the tumour. All tumour measurements were reviewed and confirmed by an independent panel of radiologists and oncologists. Secondary efficacy endpoints included the duration of response (measured from the onset of the best response to the date of disease progression), time to progression (calculated from the start of therapy to the time of progression or relapse) and overall survival.
Statistical methods
An ‘optimal two-stage design’ was chosen for this phase II trial (Gehan, 1961). If fewer than four responses were noted in the first 17 eligible patients, accrual would be halted. Because responses were observed, additional patients were enrolled to a final accrual of 45 patients to better estimate efficacy and characterise the toxicity profile. This sample size was considered sufficient to estimate 95% confidence intervals for the true response rate with a maximum width of 30%. For the response rate, 95% confidence intervals were calculated as previously described (Anderson et al, 1985). The distribution of time to death from the time of study entry was estimated by using the Kaplan–Meier product-limit method (Kaplan and Meier, 1958). All patients who were enrolled onto the study were included in the intent-to-treat analysis.
RESULTS
Patient characteristics
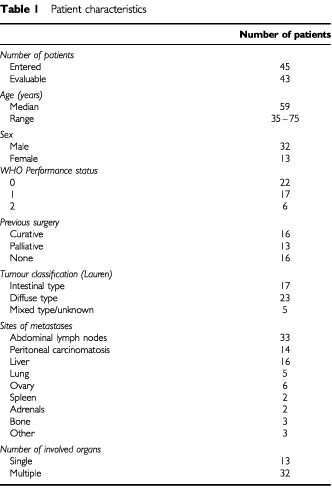
Between January 1999 and November 2000, a total of 45 patients took part in this trial. All of them were evaluable for toxicity and 43 patients for response assessment. Two patients who were considered non-measurable by the external review committee, were kept in the final intent-to-treat analysis of response. The demographic data, sites of metastatic tumour, and previous therapies are listed in Table 1. The median age of the 13 female and 32 male patients was 59 years (range, 35 to 75 years), and the median WHO performance status was 1 (range, 0–2). Except for 13 patients, all had multiple metastases involving two or more organ systems. Twenty-nine patients (64%) had disseminated disease at the time of first diagnosis, 13 of whom required palliative surgical interventions. The remaining 16 patients had metastatic disease recurrence after having undergone previous potential curative resection; the median interval from initial diagnosis to relapse was 11 (range, 3 to 131) months in these patients.
Table 1. Patient characteristics.
A total of 398 courses of study treatment were administered to the 45 patients. The median number of treatment cycles was 10 (range, 2 to 12), and the median duration of follow-up at the time of this analysis was 17 (range, 6–29) months.
Response to treatment
The overall response rate was 44.4% (95% confidence interval, 29.7 to 60.0%), including five (11.1%) complete and 15 (33.3%) partial remissions; the median duration of response was 6.5 months (range, 3 to 17 months). Twelve additional patients (26.6%) had disease stabilisation, and 11 (24.5%) progressed while on treatment. The median time to disease progression was 7 months (range, 1 to 20) and the median survival was 11.2 months (range, 1.5 to 21+) with 12 patients (26.7%) still being alive after a median follow-up time of 14 months. Sixteen patients, who failed paclitaxel/cisplatin or experienced tumour progression within 6 months after completion of chemotherapy, received second-line therapy. The most frequently used second-line regimens were fluorouracil/leucovorin plus etoposide (n=4) or epirubicin (n=5), and oxaliplatin/raltitrexed in seven patients.
Toxicity
Side effects associated with treatment are listed in Tables 2 and 3. Myelosuppression was the most commonly encountered toxicity, although according to the ANC-adapted use of G-CSF, the time to WBC/ANC recovery was generally short: 95% of the episodes of leukopenia/neutropenia were resolved within 7 days. Administration of G-CSF because of ANCs of 1000 to 2000 per μL on the day of scheduled chemotherapeutic drug administration, as indicated in the protocol, was effected in 26 patients (58%), after a median of 6 courses (range, 1 to 12). A total of 59 5-day courses of G-CSF were given with most of the patients (73%) receiving fewer than three courses. Leukocytopenia occurred in 39 patients (87%), and was grade 3 or 4 in five (11%) and two (4%) patients. Neutropenia was also observed in 39 cases (87%), and was grade 3 or 4 in 10 (22%) and five patients (11%), respectively. Five patients (11%) developed documented infection, one of whom required hospitalisation for intravenous antibiotics. Anaemia was commonly observed (69%) and was grade 3 in two patients (4%). Twenty-two patients (49%) received erythropoietin because their pretreatment haemoglobin value was or dropped below 12.0 mg dl−1 during chemotherapy and 17 of them (77%) responded to this haematopoetic growth factor support. Grade 1 or 2 thrombocytopenia was seen in only three patients.
Table 2. Highest grade of haematologic toxicity experienced (n=45).
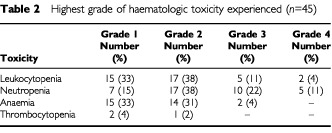
Table 3. Highest grade of nonhaematologic toxicity experienced (n=45).
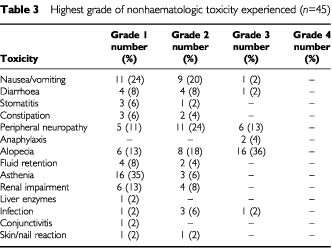
Nonhaematologic adverse reactions are listed in Table 3. Gastrointestinal symptoms were the most frequently encountered toxicities. Nausea and vomiting occurred in 21 patients (47%), symptoms however, were generally mild or moderate (grade 1, 2 or 3 in 24, 20 or 2%, respectively) and responsive to standard antiemetic therapy. Diarrhoea was noted in nine patients (20%) and was grade 3 in only one case. Constipation occurred in five patients, and grade 1 or 2 stomatitis in four. Twenty-two patients (49%) developed peripheral neuropathy, including 6 (13%) who experienced severe (WHO grade 3) symptoms. Two patients (4%) developed anaphylactic reactions despite adequate premedication. Skin reactions and nail changes were seen in two patients each, and minor fluid retention in six. Alopecia was noted in a total of 30 patients (67%), 16 of who had complete hair loss. Asthenia was reported by 19 (42%) patients. Transiently impaired liver and renal function were observed in one (2%) and 10 (22%) patients, respectively.
Drug exposure
The dose of both chemotherapeutic drugs was reduced in three patients due to (febrile) grade 4 neutropenia and in two patients because of (grade 1) nephrotocixity; dose modifications of paclitaxel according to progressive peripheral neuropathy were required in five additional patients. Fifteen patients (33%) had at least one treatment delay of 1 week at some time during therapy, and the total number of delayed courses was 29 (14%). The reasons for delayed courses were haematologic toxicity in 20 cases, neutropenic fever in four, transiently impaired renal function in one, deterioration in performance status in two, and personal reasons in two patients. Treatment was discontinuated prematurely in two patients because of anaphylaxis, in four patients due to grade 3 peripheral neuropathy (after six to 10 treatment courses), in one case because of intercurrent upper gastrointestinal tract bleeding, and in two additional patients for personal reasons.
Dose-intensity was calculated for each patient and for each drug. The mean given dose-intensity of the combination was 92% of the projected dose. The mean delivered dose of paclitaxel per week was 73.6 mg per m2 (range, 59.2 to 80 mg per m2) and the mean delivered dose of cisplatin per week was 27.6 mg per m2 (range, 22.2 to 30 mg per m2).
DISCUSSION
The continuing lack of substantial progress in the treatment of advanced gastric cancer, particularly in patients with poor performance status or compromised organ function, who are unlikely to tolerate potentially active but toxic regimens, has prompted investigators to evaluate new agents and/or drug combinations including docetaxel, paclitaxel, and irinotecan (Bokemeyer et al, 1997; Boku et al, 1999; Murad et al, 1999; Kollmannsberger et al, 2000; Roth et al, 2000; Ridwelski et al, 2001).
The present study, to our knowledge, is the first to report mature results on the efficacy and safety with the combination of paclitaxel plus cisplatin in patients with advanced gastric cancer. The rationale for their combined use were: (1) the documented activity of both drugs in gastric cancer when used as single agent (Wils, 1996); (2) the apparent synergistic efficacy and safety of this combination in patients with ovarian-, head and neck cancer, and NSCLC (Ilson et al, 1998; Gatzemeier et al, 2000; Khuri et al, 2000; Pfisterer, 2000); (3) as well as the encouraging results of two recently published reports of a combination of cisplatin and the semisynthetic taxoid docetaxel (Roth et al, 2000; Ridwelski et al, 2001).
With an intent-to treat response rate of 44%, including 11% complete remissions, a median progression free interval of 7 months, and median overall survival of 11.2 months, the results of the present multicenter phase II investigation suggest a marked antitumour activity of this combination in patients with metastatic gastric cancer. The non-randomised phase II study design, as we have learned in the past, does not allow to draw any firm conclusion nor any direct comparison with other regimens. In fact, other drug combinations with even higher objective response rates than observed in the present study have been described in the past, and have failed to show superiority in subsequent phase III trials (Kelsen et al, 1998; Vanhoefer et al, 2000). Therefore, results must be interpreted with caution, and warrant confirmation in a randomised trial setting. Still, the observed antitumour potential, which is in agreement with the previously mentioned phase II studies of Roth et al (2000) (RR 56%, median survival 9 months), and Ridwelski et al (2001) (RR 37%, median survival 10.4 months), suggests that taxane/cisplatin-based combination chemotherapy might be as active as second- or even third-generation regimens including ECF or the more intense and toxic PELF (Cascinu et al, 1997; Webb et al, 1997). Potential advantages of the described biweekly and other taxane+cisplatin combination regimens are related to the non-requirement of a central venous access and external infusional devices with their associated risks and costs (Lemmers et al, 1996; Kock et al, 1998).
As it concerns the tolerance of treatment, neutropenia was a commonly encountered adverse reaction associated with this regimen, and WHO grade 3 or 4 toxicity occurred in 15 patients (33%). Due to the actual ANC-adapted use of G-CSF, however, only 20 of 398 courses (5%) had to be delayed for haematologic toxicity reasons, and there was a low rate of febrile neutropenic episodes with only one patient requiring hospitalisation. The rather high rate/incidence of anaemia in our patient population was probably not only caused by therapy, but also influenced by the underlying malignant disease. Twenty-two patients received recombinant human erythropoietin according to the protocol and 17 of them (77%) responded to the haematopoetic growth factor support. In as much reversing anaemia in these patients has contributed to the favourable study outcome can not be determined. Clinical trials, however, have shown that correcting anaemia not only provides an objective improvement in the patients' well being, but may also improve response and possibly the duration of survival (Littlewood, 2001; Littlewood et al, 2001).
Apart from anaphylactic reactions in two patients and grade 3 peripheral neurotoxicity in six, nonhaematologic adverse reactions were generally mild to moderate and fully reversible. Despite use/realisation of a high dose intensity of both chemotherapeutic drugs, in addition to a lower rate of neutropenia, also certain nonhaematologic toxicities such as arthralgia/myalgia, asthenia and gastrointestinal symptoms were less commonly seen when compared to other phase II/III studies of this particular drug combination in other disease entities (McGuire et al, 1996; Rose et al, 1999; Gatzemeier et al, 2000). Similarly, in the advanced gastric cancer trials of Roth et al (2000) and Ridwelski et al (2001), investigating docetaxel and cisplatin at a dose of 75–85 mg per m2 once every 3 weeks, a much higher rate of severe haematotoxicity (up to 57% of patients experienced grade 4 neutropenia), and grade 3 gastrointestinal adverse reactions (which occurred in about 9% in both trials) was noted.
In conclusion, the results of this trial indicate that the described biweekly combination regimen of paclitaxel plus cisplatin±G-CSF and/or erythropoietin is an effective and tolerable regimen for disseminated gastric cancer. It seems to have durable antitumour activity with an acceptable level of both haematologic and other organ toxicities. Compared with previous phase II/III investigations of this combination in other malignancies, the incidence of severe neutropenia as well as of certain other nonhaematologic adverse reactions seems to be lower. The difference might be explained by the ANC-adapted use of G-CSF±erythropoietin, the choice of the taxane, and/or the biweekly chemotherapeutic drug administration schedule. In view of the promising therapeutic index of the described regimen, further evaluation of this combination in patients with advanced disease as well as in the neoadjuvant setting, seems warranted. In these and/or other clinical trials in patients with gastric cancer receiving cytotoxic chemotherapy, it might also be of particular interest to try to define precisely the impact of correcting anaemia with erythropoietin in terms of quality of life and therapeutic outcome.
ACKNOWLEDGEMENTS
Supported in part by the Gesellschaft zur Erforschung der Biologie und Behandlung von Tumorkrankheiten.
References
- AndersonJRBernsteinLPikeMCl1985Approximate confidence intervals for probabilities of survival and quantiles in life-table analysis Biometrics 38407416 [PubMed] [Google Scholar]
- ArbuckSG1994Taxol (paclitaxel): future directions Ann Oncol 5S59S62 [PubMed] [Google Scholar]
- BokemeyerCHartmannJTLampeCSClemensMRQuietzschDForkmannLKanzL1997Paclitaxel and weekly 24-hour infusion of 5-fluorouracil/folinic acid in advanced gastric cancer Semin Oncol 24S19-96S19-100 [PubMed] [Google Scholar]
- BokuNOhtsuAShimadaYShiraoYSekiSSaitoHSakatYHyodoI1999Phase II study of a combination of irinotecan and cisplatin against metastatic gastric cancer J Clin Oncol 17319323 [DOI] [PubMed] [Google Scholar]
- BrunnPA1997Defining the role of paclitaxel in lung cancer: Summary of recent studies and implications for future directions Semin Oncol 24Suppl 12S12-153S12-162 [PubMed] [Google Scholar]
- CascinuSLabiancaRAlessandroniPMarcelliniMSilvaRRPanceraGTestaEMartignoniGBarniSFrontiniLZaniboniALuporininGCellerinoRCatalanoG1997Intensive weekly chemotherapy for advanced gastric cancer using fluorouracil, cisplatin, epidoxorubicin, 6S-leucovorin, glutathione, and filgrastim: a report from the Italian Group for the Study of Digestive Tract Cancer J Clin Oncol 15329933009363858 [Google Scholar]
- FindlayMCunninghamDNormanAMansiJNicholsonMHickishTNicolsonVNashASacksNFordHCarterRHillA1994A phase II study in advanced gastro-esophageal cancer using epirubicin and cisplatin in combination with continuous infusion 5-fluorouracil (ECF) Ann Oncol 5609616 [DOI] [PubMed] [Google Scholar]
- FuchsCS1997Chemotherapy for advanced gastric cancer: where do we stand? J Clin Oncol 1532993300 [DOI] [PubMed] [Google Scholar]
- GatzemeierUvon PawelJGottfriedMten VeldeGPMMattsonKDeMarinisFHarperPSalvatiFRobinetGLucentiABogaertsJGallantG2000Phase III comparative study of high dose cisplatin versus a combination of paclitaxel and cisplatin in patients with advanced non-small-cell lung cancer J Clin Oncol 1833903399 [DOI] [PubMed] [Google Scholar]
- GehanEA1961The determination of the number of patients required in a follow-up trial of a new chemotherapeutic agent J Chron Dis 13346353 [DOI] [PubMed] [Google Scholar]
- GlimeliusBEkströmKHoffmanKGrafWSjödénPOHaglundUSvensonCEnanderLKLinnéTSellströmHHeumanR1997Randomized comparison between chemotherapy plus supportive care in advanced gastric cancer Ann Oncol 8163168 [DOI] [PubMed] [Google Scholar]
- IlsonDHAjaniJBhallaKForastiereAHuangYPatelPMartinLDoneganJPazdurRReedCKelsenDP1998Phase II trial of paclitaxel, fluorouracil, cisplatin in patients with advanced carcinoma of the esophagus J Clin Oncol 1618261834 [DOI] [PubMed] [Google Scholar]
- KaplanELMeierP1958Non-parametric estimation from incomplete observations J Am Stat Assoc 53458481 [Google Scholar]
- KelsenDAtiqOSaltzLNiedzwieckiDGinnDChapmanDHeelanRLightdaleCVincguerraVBrennanM1998FAMTX versus etoposide, doxorubicin, and cisplatin: a random assignment trial in gastric cancer J Clin Oncol 10541548 [DOI] [PubMed] [Google Scholar]
- KhuriFRShinDMGlissonBSLippmanSMHongWK2000Treatment of patients with recurrent or metastatic squamous cell carcinoma of the head and neck: current status and future directions Semin Oncol 27Suppl 82533 [PubMed] [Google Scholar]
- KockHJPietschMKrauseUWilkeHEiglerFW1998Implantable vascular access systems: experience in 1500 patients with totally implanted central venous port systems World J Surg 221216 [DOI] [PubMed] [Google Scholar]
- KollmannsbergerCQuietzschDHaagCLingenfelserTSchroederMHartmannJTBaroniusWHempelVClemensMKanzLBokemeyerC2000A phase II study of paclitaxel, weekly, 24-hour continous infusion fluorouracil, folinic acid and cisplatin in patients with advanced gastric cancer Br J Cancer 83458462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- LandisSHMurrayTBoldenSWingoPA1998Cancer statistics CA Cancer J Clin 486299449931 [Google Scholar]
- LemmersNWGelsMESlijferDTPlukkerJTvan der GraafWTde LangenZJDrosteJHKoopsHSHoekstraHJ1996Complications of venous access ports in 132 patients with disseminated testicular cancer treated with polychemotherapy J Clin Oncol 1429162922 [DOI] [PubMed] [Google Scholar]
- LittlewoodTJ2001The impact of hemoglobin levels on treatment outcomes in patients with cancer Semin Oncol 2Suppl 84953 [DOI] [PubMed] [Google Scholar]
- LittlewoodTJBajettaENortierJWRVercammenERapaportB2001Effects of epoetin alfa on hematologic parameters and quality of life in cancer patients receiving nonplatinum chemotherapy: results of a randomized, double-blind, placebo-controlled trial J Clin Oncol 1928652874 [DOI] [PubMed] [Google Scholar]
- McGuireWPHoskinsWJBradyMFKuceraPRPartridgeEELookKYClarke-PearsonDLDavidsonM1996Cyclophosphamide and cisplatin compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian cancer N Engl J Med 33416 [DOI] [PubMed] [Google Scholar]
- MorantR2001Neoadjuvant and adjuvant chemotherapy of locally advanced stomach cancer Onkologie 24116121 [DOI] [PubMed] [Google Scholar]
- MuradAMPetroianuAGuimaraesRCAragaoBCCabralLOScalabuANetoAO1999Phase II trial of the combination of paclitaxel and 5-fluorouracil in the treatment of advanced gastric cancer: a novel, safe, and effective regimen Am J Clin Oncol 22580586 [DOI] [PubMed] [Google Scholar]
- PfistererJ2000Optimierung der primären Chemotherapie des fortgeschrittenen Ovarialkarzinoms Onkologie 233143 [Google Scholar]
- PierelliLPerilloAGreggiSSalernoGPaniciPBMenichellaGFattorossiALeoneGMancusoSScambiaG1999Erythropoietin addition to granulocyte colony-stimulating factor abrogates life-threatening neutropenia and increases peripheral-blood progenitor-cell mobilization after epirubicin, paclitaxel, and cisplatin combination chemotherapy: results of a randomized comparison J Clin Oncol 1712881295 [DOI] [PubMed] [Google Scholar]
- PyrhonenSKuitunenTNyandotoPKouriM1995Randomised comparison of fluorouracil, epidoxorubicin and methotrexate (FEMTX) plus supportive care with supportive care alone in patients with non-resectable gastric cancer Br J Cancer 71587591 [DOI] [PMC free article] [PubMed] [Google Scholar]
- RidwelskiKGebauerTFahlkeJKrönigHKettnerEMeyerFEichelmannKLippertH2001Combination chemotherapy with docetaxel and cisplatin for locally advanced and metastatic gastric cancer Ann Oncol 124751 [DOI] [PubMed] [Google Scholar]
- RosePGBlessingJAGershensonDMMcGeheeR1999Paclitaxel and cisplatin as first-line therapy in recurrent or advanced squamous cell carcinoma of the cervix: a Gynecologic Oncology Group Study J Clin Oncol 1726762680 [DOI] [PubMed] [Google Scholar]
- RothADMaibachRMartinelliGFazioNAaproMSPaganiOMorantRBornerMMHerrmannRHoneggerHCavalliFAlbertoPCastiglioneMGoldhirschAon behalf of the Swiss Group for Clinical Cancer Research (SAKK), Bern, Switzerland and the European Institute of Oncology (EIO), Milan, Italy2000Docetaxel (Taxotere)–Cisplatin (TC): an effective drug combination in gastric carcinoma Ann Oncol 11301306 [DOI] [PubMed] [Google Scholar]
- SafranHWaneboHJHeskethPJAkermanPIanittiDCioffiWDiPetWolfBKonessJMcAnawRMooreTChenMHRadie-KeaneK2000Paclitaxel and concurrent radiation for gastric cancer Int J Radiat Oncol Biol Phys 46889894 [DOI] [PubMed] [Google Scholar]
- ScheithauerWKornekGVZehBStögerFXSchenkTHejnaMDepischD1995Palliative chemotherapy versus supportive care in patients with metastatic gastric cancer: a randomized trial. Second International Conference on Biological Preventive Treatment Gastro Intestinal Malignancy, Köln, Germany P 68(abstr)
- SoerensenJBWedervangKDombernowskyP1997Preliminary results of a phase II study of paclitaxel and cisplatin in patients with non-small cell lung cancer Semin Oncol 24Suppl 121820 [PubMed] [Google Scholar]
- Van der GaastAKokTCVosRKerkhofsLSplinterAW1997A phase I dose finding study of a biweekly schedule of a fixed dose of cisplatin with increasing doses of paclitaxel in patients with advanced esophageal cancer Semin Oncol 24Suppl 198285 [PubMed] [Google Scholar]
- VanhoeferURougierPWilkeHDucreuxMLacaveAVan CutsemEPlankerMDos SantosJGPiedboisPPaillotBBodensteinHSchmollJHBleibergHNordlingerBCouvreurMLBaronBWilsJA2000Final results of a randomized phase III trial of sequential high-dose methotrexate, fluorouracil, and doxorubicin versus etoposide, leukovorin, and fluorouracil versus infusional fluororuracil and cisplatin in advanced gastric cancer: a trial of the European Organization for Research and Treatment of Cancer Gastrointestinal Tract Cancer Cooperative Group J Clin Oncol 1826482657 [DOI] [PubMed] [Google Scholar]
- WebbACunninghamDScarffeJHHarperPNormanAJoffeJKHughesMMansiJFindlayMHillAOatesJNicolsonMHickishTO'BrienMIvesonTWatsonMUnderhillCWardleyAMeehanM1997Randomized trial comparing epirubicin, cisplatin, and fluorouracil versus fluorouracil, doxorubicin, and methotrexate in advanced oesophagogastric cancer J Clin Oncol 15261267 [DOI] [PubMed] [Google Scholar]
- WilsJ1996The treatment of advanced gastric cancer Semin Oncol 23397406 [PubMed] [Google Scholar]