

Abstract
Choroid plexus tumours are rare epithelial brain tumours and limited information is available regarding their biology and the best treatment. A meta-analysis was done to determine prognostic factors and the influence of various treatment modalities. A thorough review of the medical literature (1966–1998) revealed 566 well-documented choroid plexus tumours. These were entered into a database, which was analysed to determine prognostic factors and treatment modalities. Most patients with a supratentorial tumour were children, while the most common sites in adults were the fourth ventricle and the cerebellar pontine angle. Cerebellar pontine angle tumours were more frequently benign. Histology was the most important prognostic factor, as one, five, and 10-year projected survival rates were 90, 81, and 77% in choroid plexus-papilloma (n=353) compared to only 71, 41, and 35% in choroid plexus-carcinoma respectively (P<0.0005). Surgery was prognostically relevant for both choroid plexus-papilloma (P=0.0005) and choroid plexus-carcinoma (P=0.0001). Radiotherapy was associated with significantly better survival in choroid plexus-carcinomas. Eight of 22 documented choroid plexus-carcinomas responded to chemotherapy. Relapse after primary treatment was a poor prognostic factor in choroid plexus-carcinoma patients but not in choroid plexus-papilloma patients. Treatment of choroid plexus tumours should start with radical surgical resection. This should be followed by adjuvant treatment in case of choroid plexus-carcinoma, and a ‘wait and see’ approach in choroid plexus-papilloma.
British Journal of Cancer (2002) 87, 1086–1091. doi:10.1038/sj.bjc.6600609 www.bjcancer.com
© 2002 Cancer Research UK
Keywords: brain tumour, meta-analysis, prognostic factors, treatment, survival, irradiation
Choroid plexus tumours (CPTs) are relatively rare primary brain tumours arising from epithelial differentiated tissue. With an annual incidence of 0.3 cases per million (Janisch and Staneczek, 1988, 1989), these tumours account for only 0.4–0.8% of all brain tumours (Zülch, 1957). The most commonly reported locations are the ventricles. Nevertheless, extraventricular sites have been described (Kimura et al, 1992; Steven et al, 1996; Mottl et al, 1997; Nakano et al, 1997), too. Tumours are classified as choroid plexus-carcinoma (CPC, WHO grade III) (Kleihues and Canvanell, 2000), when they show nuclear pleomorphism, high nucleus to cytoplasm ratios, blurring of the papillary pattern, and necrosis (Paulus and Janisch, 1990). In addition, these tumours frequently express carcinoembryonic antigen (CEA) (Paulus and Janisch, 1990), and CD44 (Varga et al, 1996) which can also be detected as a marker in peripheral blood (Hashizume et al, 1995). Choroid plexus-papilloma (CPP, WHO grade I), the more differentiated tumours, expresses more frequently the markers pre-albumin (Matsushima et al, 1988) and the S100 protein. The average labelling indices with MIB1, a proliferation marker, were 14% in CPC and 3.7% in CPP (Vajtai et al, 1996). However, this histological classification is not clear cut. The possibility of a development from papilloma to carcinoma has been documented (Diengdoh and Shaw, 1993), and metastases occur not only in patients with CPC (Bennedback and Therkildsen, 1990; Kang et al, 1997) but also in patients with CPP (Leys et al, 1986; Domingues et al, 1991; Enomoto et al, 1991).
The current treatment of choroid plexus tumours is based on little evidence. None of the national paediatric oncology groups cover a population large enough to perform a randomised trial. In general it is believed that surgical resection is an important element of treatment. Postoperatively, infants with choroid plexus carcinoma are frequently treated with adjuvant chemotherapy and adult patients are treated with irradiation therapy. Patients with choroid plexus papilloma are mostly treated similar to those with low grade glioma. We performed a systematic literature review to assess prognostic factors and treatment efficacy in choroid plexus tumours as a basis for stimulating an international consensus to form the basis of an international trial working group mainly within the International Society for Paediatric Oncology (SIOP).
METHODS
The first step for this analysis was a literature search in the Medline database, including all publications up to January 1998. Search words used were ‘Choroid plexus’ or ‘CPT’ or ‘CPP’ limited to ‘human’. This yielded 4120 titles of which 1520 appeared promising to contain the information listed below. Reading the abstracts reduced this number to 551. However, reading those publications increased the number again, because the referee list of some of them contained publications, which had not been found in Medline. Some of those were chapters in textbooks (Rubinstein and Brucher, 1981; Kleihues et al, 1997). This yielded binally a total of 572 publications.
The second step was to create a patient database from cases mentioned in the literature. Documented fields included first author, publication year, symptoms and signs, duration of symptoms until diagnosis, age at diagnosis, race, gender, histology, size of tumour, location, presence of metastases, type of surgery, type of radiotherapy, radiotherapy response, type of chemotherapy, chemo-response, tumour recurrence, observation time, and outcome. When tumours were diagnosed at autopsy or when patients died during the first surgery, they were encoded as observation time=0 and outcome=death. Patients published without any observation time and without outcome description were encoded as observation time=0, outcome=survival. Not all of these fields collected sufficient information for final analysis. Publications were excluded from the analysis when extractable information filled less than two fields of the database. In case of replicated publications from the same group, only the most recent publication was used for data-entry.
The database was first analysed using the technique of the stratified subgroup analyses with ‘SPSS®’ (SPSS Inc, San Francisco, CA, USA). First the qualitative parameters such as tumour location, histology, and gender were used to divide the database in various groups. χ2 or Fishers exact tests and ANOVA were used to assess the homogeneity for other parameters within these groups and subgroups. Survival was analysed using Kaplan–Meier estimates and compared with log rank tests. Cox regression analysis was then used to repeat analyses for the same questions.
RESULTS
After applying the exclusion criteria, 217 publications were left with sufficient information. The number of patients reported within each study was between one and 54 (Palazzi et al, 1989). This resulted in a database of 566 patients.
Gender, age at diagnosis, location, histology and metastases could be correlated to each other regardless if treatment or observation time data were sufficient. Surprisingly, none of these parameters was distributed homogeneously among groups defined by the others. In the total group, the male : female ratio was 1.2 : 1. Relating gender to location showed relatively more female patients with tumours located in the cerebellopontine angle (CPA, 29 observed, 20 expected). Age at diagnosis covered a large range from 0 years (foetus) to 72 years, but most of the patients were children, resulting in a median age at diagnosis of 3.5 years in the whole database. The most striking inhomogeneity was found when relating age to location (Figure 1). The age distribution shifted from younger to older patients the more caudal the tumour was located. This resulted in median ages of 1.5 years, 1.5 years, 22.5 years, and 35.5 years in the groups of tumours located in the lateral ventricle, third ventricle, fourth ventricle and CPA, respectively (P<0.005 ANOVA). In the total group, the number of CPP was higher than CPC (353 vs 207). When relating malignancy to location, the relative frequency of CPC was higher in lateral ventricles and CPP was more frequent in CPA-tumours (P<0.005). Overall 12% of patients presented with metastatic disease. This frequency was higher for those with CPC histology (P<0.0005) and with supratentorial location (P=0.04). However, numbers were too small for subgroup analyses of this variable. The metastases occurred predominantly along the cerebrospinal fluid pathways (Allen et al, 1992), other sites included abdomen (Geerts et al, 1996), bone (Valladares et al, 1980), and lung (Sheridan and Besser, 1994). Abdominal seeding has been described in patients with a ventricular-peritoneal shunt (Mccallum et al, 1988) and one case of metastasis to the tibia has been published (Hayakawa et al, 1979). The symptom duration of patients with tumours located in the cerebellopontine angle was longer than in other patients.
Figure 1.

Age distribution of choroid plexus tumours: Supratentorial tumours occur most frequently in infants (A) n=188, while the age distribution of infratentorial tumours is spread over all ages (B), n=71; P<0.005, Mann–Whitney U-test). This analysis included only patients with documented primary intracerebral locations.
When survival was used as endpoint, patients with observation time equaling 0 were excluded. This left 266 patients for analysis. In these patients, the prognostic relevance of the available variables were assessed. In an univariant analysis, histology was a significant prognostic factor (Figure 2). One, five, and 10 year projected survival rates of plexus carcinoma patients were 71, 41, 35% in comparison to CPP patients with 90, 81, 77%, respectively (Figure 2, P<0.0005 log-rank test). Some tumours were primarily described as ‘atypical choroid plexus papilloma’. In second surgeries or autopsies of these patients, a repeat histology was frequently reported as CPC. The survival curve of those ‘atypical CPP’ was between the curves of CPP and CPC, but the number of cases was too small for a meaningful analysis.
Figure 2.
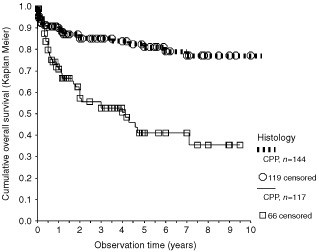
Survival of patients published as CPP with CPC patients. Only patients with observation times >0 and clear histological allocation were included. Symbols indicate end of observation times of surviving patient (=censored data). Statistically significant: P<0,0005, log rank test.
When analysing age at diagnosis, the poorest survival was noted for those over 40 years of age, followed by those under 10 years of age, with the best outcome for those aged 10–40 years (Figure 3). The gender and location parameters did not have prognostic relevance. In the total group of CPT, metastasis was a significant factor in survival time (P=0.02), however, metastases were more frequent in CPC, and in subgroup analyses the numbers became too small for meaningful analysis.
Figure 3.

Young children and patients over 59 years of age have a worse prognosis as compared to the age classes in between (P<0.0005 log rank test). This included patients, in whom the observation time was >0, and in whom age at diagnosis was documented. Survival rates were calculated as Kaplan–Meier estimates.
Treatment modalities analysed in this study included surgery, radiotherapy, and chemotherapy. Of those, surgery showed the most striking differences (Figure 4). CPP patients with complete resection had a 10-year survival rate of 85% (±10% standard deviation). This compared to 56% with less than gross total resection and to a one year survival rate of only 50% in patients after biopsy (P=0.002). CPC patients had a 2-year survival rate of 72% (±10%) vs 34% (±10%) for those with a gross total resection or an incomplete resection, respectively. For the analysis of irradiation, the variable ‘malignancy’ and ‘surgery’ were used to create subgroups. For CPC patients, those that received irradiation did better than those without irradiation in both subgroups, after complete and incomplete resection (Figure 5). In the subgroup of patients with CPC who had gross total resection, there were 25 patients who further received irradiation and 24 patients who did not receive irradiation. The comparison of these two groups showed a significant benefit for patients receiving irradiation (Wolff et al, 1999). The data of patients with incomplete resection are shown in Figure 5. The survival time of 19 patients receiving irradiation was significantly better (P=0.029) than that of nine patients not given irradiation. Response to chemotherapy was well documented in CPC (Table 1). The overall response rate was 8 of 22. With these limited data the impact of chemotherapy on survival could not be sufficiently analysed.
Figure 4.

In both, CPC, (A) and CPP (B), the type of surgery was a statistically significant prognostic factor (P=0.0001, and P<0.00005, respectively, log rank tests).
Figure 5.
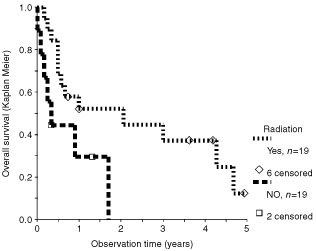
Influence of irradiation on survival with incompletely resected CPC. Inclusion factors for this analysis were: Observation time >0, histology CPC, surgery well documented, less than gross total resection. The difference in favour of irradiation is marginally statistically significant (P=0.029, log rank test).
Table 1. Response to multiagent chemotherapy in choroid plexus carcinoma.

Relapse after treatment was documented in 52 cases. It was not surprising that CPC patients who relapsed after treatment did poorly. The projected 2-year survival rate for these patients was 54%, as compared to 62% for CPC patients in which relapse was not mentioned. By contrast, CPP patients with documented relapse had the same survival as CPP patients without relapse. A further interesting difference between CPP and CPC came up when the year of publication was analysed with respect to prognosis. Surprisingly, there was no improvement of the CPC-prognosis over the years. By contrast the survival of CPP patients published after 1970 was superior to earlier publications (5-year survival rate: 83%, n=132 vs 35%, n=12, significant P<0.0005, log-rank test).
DISCUSSION
This systematic literature review was initiated to determine risk factors and the best management for choroid plexus tumours (CPT). However, a literature review cannot produce the level of evidence that one might wish for since there is no certain way to control publication bias. Whenever possible, clinical treatment decisions should be based on prospective randomised trials, but in the absence of those, a systematic literature review might provide the best possible evidence.
The etiology of some choroid plexus tumours has been linked to SV40 infections (Tabuchi et al, 1978a,b; Bergsagel et al, 1992; Lednicky et al, 1995; Martini et al, 1996), but it might also be influenced by other factors such as X-chromosome linked syndromes (Steichen-Gersdorf et al, 1993; Sybert et al, 1994; Kleihues, 1997). We found significant differences when relating gender to age at diagnosis, tumour location or pathology. Cerebello-pontine angle tumours were associated with older age, benign histology, and female gender. This could suggest a tumour entity linked to a tumour-suppressor gene located on the X-chromosome. Interestingly, the syndromes with defects on the X-chromosome were reported with choroid plexus papilloma (Hamano et al, 1991; Steichen-Gersdorf et al, 1993; Sybert et al, 1994; Trifiletti et al, 1995; Zajac et al, 1997). By contrast, the infant type of choroid plexus tumours was most frequently located in the lateral ventricles and had a male predominance. Interestingly, the report about SV40 in choroid plexus tumours described children only (Bergsagel et al, 1992). Based on this analysis we hypothesised that SV40 is more frequently found in infant tumours and that there is a distinctly different aetiology in adult choroid plexus tumours.
The definitive diagnosis of a choroid plexus-tumour can only be made histologically. The allocation to either CPP or CPC might be debatable in individual cases. In fact, others have found a significant number of tumours changing the allocated diagnosis, when reviewed in a reference centre (Berger et al, 1998). Despite this, our data show that the published histological diagnosis is a significant risk factor, even when reference pathology is missing in most cases. Surgery is therefore required for the diagnosis. Tumour resection is also a powerful therapeutical step. In both diagnoses, CPC and CPP, the prognosis was better in completely resected tumours. Especially in the case of CPC patients (Packer et al, 1992), the positive relevance of surgery appears to be greater than in most other brain tumours. This supports a second surgery when the post surgical radioimaging shows residual tumour.
In CPC patients adjuvant treatment should follow surgery. Response to irradiation has been demonstrated in at least five patients with residual tumour after surgery (Carrea and Polak, 1977; Naguib et al, 1981; Griffin et al, 1988; Hashizume et al, 1995; Wolff et al, 2001a,b). Based on our analysis, patients with gross total resection should indeed receive irradiation. We confirmed significant improved survival for patients with CPC who received irradiation in both subgroups (a) with residual tumour (Figure 5) and (b) after gross total resection (Wolff et al, 1999). However, radiation is to be avoided in young children, in whom long term sequelae are severe. This leaves chemotherapy as adjuvant modality for the majority of patients. Chemotherapy can result in shrinkage of CPC tissue (Table 1), and chemotherapy has been recommended by some authors (Duffner et al, 1995; Geerts et al, 1996), but the experience with this modality has been limited, and evidence for an impact on the number of long term surviving patients is still missing. The numbers are simply too small to provide such evidence. Similarly, the relative contribution of the various single agents to response cannot be evaluated. A clinical study addressing that question will need a patient population larger than any of the current national paediatric oncology groups. This should therefore be done in an intercontinental setting. The fact that prognosis of patients published prior to 1970 is unchanged to the prognosis in the most recent publications warrants the start of such an effort. Recurrence of CPC has to be judged incurable with conventional treatment, and is therefore an indication for experimental treatment.
CPP treatment should be different. Surgery appears to be the most important modality in plexus papilloma (Raimondi and Gutierrez, 1975; Schijman et al, 1990; Sharma et al, 1994; Tacconi et al, 1996; Costa et al, 1997). Guidetti and Spallone (1981) reported 50% survivors after surgery only already in 1981. In infants, plexus papillomas are the brain tumours with the best prognosis (Mcgirr et al, 1988; Tomita et al, 1988; Buetow et al, 1990). In contrast to CPC, there is no published evidence yet that adjuvant treatment has any impact on survival of CPP patients. Recurrences may occur as late as 11 years after diagnosis (Buetow et al, 1990), which is much later than predicted by the Collins rule (Valladares et al, 1980). However, in our analysis, the prognosis of patients with CPP is still good when these patients relapse. The better prognosis documented in publications after 1970 is most likely caused by improvement of surgical and intensive care techniques. Therefore, the data collected in this review further support a ‘wait and see’ policy after first tumour resection.
In conclusion, the data generated in this meta-analysis supports the hypothesis of distinct choroid plexus tumour subtypes which differ in variables such as gender, age at diagnosis, prognosis, location and malignancy. The previously known importance of gross total resection was confirmed by this analysis. In addition, evidence was provided that adjuvant therapy increases survival in CPC patients. This work was initiated by an international consensing discussion, which has resulted in an international study to standardise and optimise the therapy.
Acknowledgments
A large case collection (Berger et al, 1998) was published after the analysed period. A repeat data analysis including these cases confirmed all key conclusions. The presented figures – except for Table 1 – were calculated with the original data, not including these cases. We thank S Clark, S Bullick and M Güllich for editing the manuscript.
References
- AllenJWisoffJHelsonLPearceJArensonE1992Choroid plexuscarcinoma – responses to chemotherapy alone in newly diagnosed young children J Neurooncol 126974 [DOI] [PubMed] [Google Scholar]
- BennedbaekOTherkildsenM1990Choroid plexuscarcinoma–report of a case with metastases within the central nervous system Acta Oncol 29241243 [DOI] [PubMed] [Google Scholar]
- BergerCThiessePLellouch-TubianaAKalifaCPierre-KahnABouffetE1998Choroid plexus carcinomas in childhood: clinical features and prognostic factors Neurosurgery 423470475 [DOI] [PubMed] [Google Scholar]
- BergsagelDJFinegoldMJButelJSKupskyWJGarceaRL1992DNA sequences similar to those of simian virus 40 in ependymomas and choroid plexus tumors of childhood N Engl J Med 326988993 [DOI] [PubMed] [Google Scholar]
- BuetowPCSmirniotopoulosJGDoneS1990Congenital brain tumor: a review of 45 cases Am J Neuroradiol 11793799 [PMC free article] [PubMed] [Google Scholar]
- CarreaRPolakM1977Preoperative radiotherapy in the management of posterior fossa choroid plexus papillomas Child's Brain 31224 [DOI] [PubMed] [Google Scholar]
- CostaJMLeyLClaramuntELafuenteJ1997Choroid plexus papillomas of the III ventricle in infants. Report of three cases Child's Nerv Syst 13244249 [DOI] [PubMed] [Google Scholar]
- DiengdohJVShawM1993Oncocytic variant of choroid plexus papilloma. Evolution from benign to malignant ‘oncocytoma’ Cancer 71855858 [DOI] [PubMed] [Google Scholar]
- DominguesRCTaverasJMReimerPRosenB1991Foramen magnum choroid plexus papilloma with drop metastases to the lumbar spine Am J Neuroradiol 12564565 [PMC free article] [PubMed] [Google Scholar]
- DuffnerPKKunLEBurgerPCHorowitzMECohenMESanfordRAKrischerJPMulhernRKJamesHERekateHL1995Postoperative chemotherapy and delayed radiation in infants and very young children with choroid plexuscarcinomas. The Pediatric Oncology Group Pediatr Neurosurg 22189196 [DOI] [PubMed] [Google Scholar]
- EnomotoHMizunoMKatsumataTDoiT1991Intracranial metastasis of a choroid plexus papilloma originating in the cerebellopontine angle region: a case report Surg Neurol 365458 [DOI] [PubMed] [Google Scholar]
- GeertsYGabreelsFLippensRMerxHWesselingP1996Choroid plexus carcinoma: a report of two cases and review of the literature Neuropediatrics 27143148 [DOI] [PubMed] [Google Scholar]
- GriffinBRStewartGRBergerMSGeyerJRO'DellMRostadS1988Choroid plexuscarcinoma of the fourth ventricle. Report of a case in an infant Pediatr Neurosci 14134139 [DOI] [PubMed] [Google Scholar]
- GuidettiBSpalloneA1981The surgical treatment of choroid plexus papilloma: the results of 27 years experience Neurosurg Rev 4129137 [DOI] [PubMed] [Google Scholar]
- HamanoKMatsubaraTShibataSHiranoCItoZAseYKusakariJTakitaH1991Aicardi syndrome accompanied by auditory disturbance and multiple brain tumors Brain Dev 13438441 [DOI] [PubMed] [Google Scholar]
- HashizumeAKodamaYHottaTYukiKTaniguchiEEguchiKYamasakiFKatayamaSYamaneTHadaY1995Choroid plexuscarcinoma in the lateral ventricle–case report Neurol Med Chir (Tokyo) 35742744 [DOI] [PubMed] [Google Scholar]
- HayakawaIFujiwaraKTsuchidaTAokiM1979Choroid plexuscarcinoma with metastasis to bone No Shinkei Geka 7815818 [PubMed] [Google Scholar]
- JanischWStaneczekW1988Epidemiology of tumors of the central nervous system–influence of the autopsy rate on the incidence rate Arch Geschwulstforsch 585155 [PubMed] [Google Scholar]
- JanischWStaneczekW1989Primary tumors of the choroid plexus. Frequency, localization and age Zentralbl Allg Pathol 135235240 [PubMed] [Google Scholar]
- KangHSWangKCKimYMKimIOKimSKChiJGChoBK1997Choroid plexus carcinoma in an infant J Korean Med Sci 12162167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- KimuraMTakayasuMSuzukiYNegoroMNagasakaTNakashimaNSugitaK1992Primary choroid plexus papilloma located in the suprasellar region: case report Neurosurgery 31563566 [DOI] [PubMed] [Google Scholar]
- KleihuesPCanvanellW2000Tumours of the Nervous SystemISBN 92832 1448X
- KleihuesPSchaubleBzur HausenAEsteveJOhgakiH1997Tumours associated with p53 germline mutations. A synopsis of 91 families Am J Pathol 150113 [PMC free article] [PubMed] [Google Scholar]
- LednickyJAGarceaRLBergsagelDJButelJS1995Natural simian virus 40 strains are present in human choroid plexus and ependymoma tumors Virology 212710717 [DOI] [PubMed] [Google Scholar]
- LeysDPasquierFLejeuneJPLesoinFPetitHDelandsheerJM1986Benign choroid plexus papilloma. 2 local recurrences and intraventricular seeding Neurochirurgie 32258261 [PubMed] [Google Scholar]
- MartiniFIaccheriLLazzarinLCarinciPCoralliniAGerosaMIuzzolinoPBarbanti-BrodanoGTognonM1996SV40 early region and large T antigen in human brain tumor, peripheral blood cell, and sperm fluids from healthy individuals Cancer Res 5648204825 [PubMed] [Google Scholar]
- MatsushimaTInoueTTakeshitaIFukuiMIwakiTKitamotoT1988Choroid plexus papilloma: an immunohistochemical study with particular reference to the coexpression of prealbumin Neurosurgery 23384389 [DOI] [PubMed] [Google Scholar]
- McCallumSCooperKFranksDN1988Choroid plexuscarcinoma. Cytologic identification of malignant cells in ascitic fluid Acta Cytol 32263266 [PubMed] [Google Scholar]
- McGirrSJEbersoldMJScheithauerBWQuastLMShawEG1988Choroid plexus papilloma: long-term follow-up results in a surgically treated series J Neurosurg 69843849 [DOI] [PubMed] [Google Scholar]
- MottlHKouteckyJ1997Treatment of spinal cord tumors in children Med Pediatr Oncol 29293295 [DOI] [PubMed] [Google Scholar]
- NaguibMGChouSNMastriA1981Radiation therapy of a choroid plexus papilloma of the cerebellopontine angle with bone involvement. Case report J Neurosurg 54245247 [DOI] [PubMed] [Google Scholar]
- NakanoIKondoAIwasakiK1997Choroid plexus papilloma in the posterior third ventricle: Case report Neurosurgery 4012791282 [DOI] [PubMed] [Google Scholar]
- PackerRJPerilongoGJohnsonDSuttonLNVezinaGZimmermanRARyanJReamanGSchutL1992Choroid plexuscarcinoma of childhood Cancer 695805851728390 [Google Scholar]
- PalazziMDi MarcoACampostriniFGrandinettiABontempiniL1989The role of radiotherapy in the management of choroid plexus neoplasms Tumori 75463469 [DOI] [PubMed] [Google Scholar]
- PaulusWJanischW1990Clinicopathologic correlations in epithelial choroid plexus neoplasm: a study of 52 cases Acta Neuropathol 80635641 [DOI] [PubMed] [Google Scholar]
- RaimondiAJGutierrezFA1975Diagnosis and surgical treatment of choroid plexus papillomas Child's Brain 181115 [DOI] [PubMed] [Google Scholar]
- RubinsteinLJBrucherJM1981Focal ependymal differentiation in choroid plexus papillomas. An immunoperoxidase study Acta Neuropathol 532933 [DOI] [PubMed] [Google Scholar]
- SchijmanEMongesJRaimondiAJTomitaT1990Choroid plexus papillomas of the III ventricle in childhood. Their diagnosis and surgical management Child's Nerv Syst 6331334 [DOI] [PubMed] [Google Scholar]
- SharmaRRoutDGuptaAKRadhakrishmanVV1994Choroid plexus papillomas Br J Neurosurg 8169177 [DOI] [PubMed] [Google Scholar]
- SheridanMBesserM1994Fatal pulmonary embolism by tumor during resection of a choroid plexus papilloma: Case report Neurosurgery 345910912 [DOI] [PubMed] [Google Scholar]
- Steichen-GersdorfETrawogerRDubaHCMayrUFelberSUtermannG1993Hypomelanosis of Ito in a girl with plexus papilloma and translocation (X;17) Hum Genet 90611613 [DOI] [PubMed] [Google Scholar]
- StevenDAMcGinnGJMcClartyBM1996A choroid plexus papilloma arising from an incidental pineal cyst Am J Neuroradiol 17939942 [PMC free article] [PubMed] [Google Scholar]
- SybertVPPagonRA1994Hypomelanosis of Ito in a girl with plexus papilloma and translocation (X;17) Hum Genet 93227. [DOI] [PubMed] [Google Scholar]
- TabuchiKKirschWMLowMGaskinDVan BuskirkJMaaS1978aScreening of human brain tumors for SV40-related T antigen Int J Cancer 211217 [DOI] [PubMed] [Google Scholar]
- TabuchiKKirschWMVan BuskirkJJ1978bImmunocytochemical evidence of SV 40-related T antigen in two human brain tumours of ependymal origin Acta Neurochir 43239249 [DOI] [PubMed] [Google Scholar]
- TacconiLDelfiniRCantoreG1996Choroid plexus papilloma: consideration of a surgical series of 33 cases Acta Neurochir 138802810 [DOI] [PubMed] [Google Scholar]
- TomitaTMcLoneDGFlanneryAM1988Choroid plexus papillomas of neonate, infants and children Pediatr Neurosci 142330 [DOI] [PubMed] [Google Scholar]
- TrifilettiRRIncorporaGPolizziACocuzzaMDBolanEAParanoE1995Aicardi syndrome with multiple tumor: a case report with literature review Brain Dev 17283285 [DOI] [PubMed] [Google Scholar]
- VajtaiIVargaZAguzziA1996MIB-1 immunoreactivity reveals different labeling in low-grade and in malignant epithelial neoplasms of the choroid plexus Histopathology 29147151 [PubMed] [Google Scholar]
- ValladaresJBPerryRHKalbagRM1980Malignant choroid plexus papilloma with extraneural metastasis. Case report J Neurosurg 52251255 [DOI] [PubMed] [Google Scholar]
- VargaZVajtaiIMarinoSSchaubleBYonekawaYAguzziA1996Tubular adenoma of the choroid plexus: evidence for glandular differentiation of the neuroepithelium Pathol Res Pract 192840844 [DOI] [PubMed] [Google Scholar]
- WolffJEASajediMCoppesMJAndersonRAEgelerRM1999Radiation therapy and survival in choroid plexus carcinoma Lancet 3532126. [DOI] [PubMed] [Google Scholar]
- WolffJEAMylesTEgelerRMPintoAKloiberT2001Detection of choroid plexus carcinoma with Tc-99m sestamibi: case report and review of the literature Med Ped Oncol 36323325 [DOI] [PubMed] [Google Scholar]
- WolffJEMylesTPintoARigelJEAngyalfiSKloiberR2001Detection of choroid plexus carcinoma with Tc-99m sestamibi: case report and review of the literature Med Pediatr Oncol 36323325 [DOI] [PubMed] [Google Scholar]
- ZajacVKirchhoffTLevyERHorsleySWMillerASteichen-GersdorfEMonacoAP1997Characterization of X;17(q12;p13) translocation breakpoints in a female patient with hypomelanosis of Ito and choroid plexus papilloma Eur J Hum Genet 56168 [PubMed] [Google Scholar]
- ZülchKJ1957Brain tumors, their biology and pathology1st editionNew York: Springer-Verlag [Google Scholar]