

Abstract
Using the concept of vulnerable populations, we examine how disparities in health may be exacerbated by population-approach interventions.
We show, from an etiologic perspective, how life-course epidemiology, the concentration of risk factors, and the concept of fundamental causes of diseases may explain the differential capacity, throughout the risk-exposure distribution, to transform resources provided through population-approach interventions into health. From an intervention perspective, we argue that population-approach interventions may be compromised by inconsistencies between the social and cultural assumptions of public health practitioners and targeted groups.
We propose some intervention principles to mitigate the health disparities associated with population-approach interventions.
IN WESTERN SOCIETIES, significant efforts during the last half century to improve health systems have resulted in spectacular gains for a wide range of health indicators.1 A growing number of studies, however, show that these gains have not benefited everyone equally; inequalities in health seem to have increased, at least for some health outcomes.2–4 This unexpected consequence is particularly troublesome in the case of population-level interventions, which seek to improve the health of the entire population.
We distinguish between 3 intervention approaches: the populations-at-risk approach, based on Lalonde’s notion of the health field5; Rose’s population approach,6 which addresses the conditions shaping the distribution of individual risk in a population; and a vulnerable population approach that addresses the conditions that put social groups “at risk of risks”—that is, risks that generate exposure to other risks. By shifting the focus to whole populations, population-level interventions, which are based on Geoffrey Rose’s population approach, represented an advancement over a population-at-risk approach.
We propose, however, that interventions based on population approaches are not free from criticism and may have led to unintended exacerbations of health disparities. Using the concept of vulnerable populations, we attempt to explain how this can be so. We begin by reviewing the notion of “populations at risk” and its relationship to Rose’s population approach and then proceed with a critique of Rose’s approach based on the notion of vulnerable populations. We conclude by suggesting that interventions addressing the needs of vulnerable populations should be used as a complement to population approaches.
LALONDE’S NOTION OF “POPULATIONS AT RISK”
The Lalonde Report,5 published in Canada in 1974, constitutes a landmark in public health policy. The report was innovative in 2 key respects. First, it organized the understanding of the determinants of health in a new way by proposing the following 4 health fields: human biology, the social and physical environment, lifestyle, and health care organization. Second, it proposed that public health interventions should focus attention on that segment of the population with the highest level of risk exposure as indicated by health risk behaviors (e.g., smoking, alcohol consumption) or biological markers (e.g., body mass index, blood pressure). This second proposal was based on an analysis of the major causes of mortality and morbidity and the underlying reasons for their occurrence, which had been identified by large-scale longitudinal studies such as the Framingham study.7 It is important to note that according to Lalonde, populations at risk are composed of individuals who all showed an elevated risk for some specific disease. This segment of the population is now often referred to as the upper end of the risk distribution.
Since the 1970s, however, several critiques have been launched at Lalonde’s “populations-at-risk” approach. First, his profile of populations at risk was based on risk factors rooted in behaviors that he considered self-imposed, individual-level lifestyle choices. It was argued by others that the creation of targeted populations based on these criteria lead to victim blaming, thereby potentially stigmatizing these populations.8 In a second critique of the populations-at-risk approach, Syme noted that although interventions based on this approach might well diminish the risk profiles of those targeted by the intervention, the distribution of newly emerging risk in society remains unaffected by the intervention because it does not target change at the level of the societal forces that induce people to engage in high-risk behaviors in the first place.9 The persistence of these forces allows the conditions for new people to enter the at-risk population to replace those who have modified their high-risk behaviors.10 Also, in his rebuttal to high-risk approaches, Rose argued that a focus on populations at risk addresses neither the conditions influencing incidence nor the shape of each population’s distribution. Rose proposed a different strategy based on the conditions that lead to the distribution of individual risk in a given population, which is now known as the population approach.
ROSE’S POPULATION APPROACH
Rose’s population approach was based on 2 important premises: the distribution of risk exposure in a population is shaped by contextual conditions11 and most cases in a population are represented by individuals with an average level of risk exposure.6 To illustrate the validity of his first premise, he famously demonstrated, using multiple empirical studies, that the causes of cases (of individual-level disease) are not the same as the causes of incidence (of population-level disease). An insightful example, provided by Cronin,12 shows that although the shape of the age-distribution graph of homicides per million per annum across the lifespan of males is the same for England and Wales and for Chicago, the incidence of homicide in Chicago is 30 times higher. Thus, although the biological factors (such as age) underlying the individual cases might be the same for the two areas (the causes of cases of disease), what shapes the distributions (the causes of incidence) is different. With regard to the second premise, Rose demonstrated, again empirically, that although the excess risk for each individual at low or average risk exposure is small, so many are exposed to it that in absolute terms the effect is large. He therefore argued that focusing efforts on the entire population and not just on high-risk individuals would be most effective in diminishing negative outcomes.
Population approaches to intervention based on Rose’s ideas involve mass environmental control methods and interventions that attempt to alter some of society’s behavioral norms.11 A current example includes the denormalization of smoking through public bans. An underlying assumption of Rose’s approach is that, as shown in Figure 1 ▶, everyone’s risk exposure in the distribution is shifted to the left (i.e., reduced) by the same amount, regardless of one’s initial position in the risk exposure distribution.
FIGURE 1—
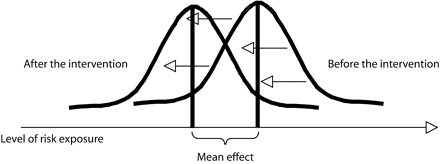
Hypothetical homogenous effect of a population-approach intervention on the distribution of risk in a population.
Note. Arrows indicate where the lines of the distribution would be after a population-level approach.
Some empirical examples demonstrate that the effects of population-approach interventions have not always fulfilled Rose’s expectations (Table 1 ▶). For example, among many populations exposed to population-approach interventions, there is an increase in the variation in the distribution of risk, where those who were formerly at lower exposure to risk derive more benefits from the interventions than those who were formerly at greater exposure to risk. This has been signaled of late in a growing literature on the social inequalities in smoking.16,17 As can be seen in Figure 2 ▶, the main overall effect of risk reduction in such a situation may mask a differential intervention effect on risk modified by the initial level of risk exposure. Assuming that the underlying relationship between risk exposure and the probability of developing an adverse outcome is not affected by the intervention, such a situation is potentially a powerful generator of health inequalities. Although we are well aware that Rose did not target inequalities in health in his strategy, we offer what we feel is a necessary complementary position to alleviate some of the unintended consequences of this approach on inequalities in health.
TABLE 1—
Effective Population Approach Interventions That Increased Health Disparities
| Intervention | Study | Resulting Disparity |
| Cervical cancer screening | Katz and Hofer 199413 | Women with higher incomes were more likely to be screened for cervical cancer in Ontario and the United States than those with lower incomes. |
| Neonatal intensive care and surfactant therapy to reduce rates of infant low birthweight | Victora et al. 200114 | New population-level interventions in Brazil increased inequity because they initially reached those who were already better off socioeconomically. |
| Health information campaigns regarding smoking | Federico et al. 200715 | Gaps in initiation rates among educational groups may be because of comprehensive information campaigns that were most effective among individuals with higher levels of education. |
FIGURE 2—
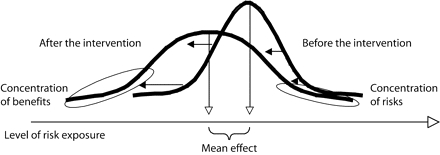
Illustration of a potential increase in the variation of risk following a population-approach intervention.
Source. Adapted from Rose.6(p74) Note. Arrows depict the shifting of the curve after a population-level approach. Circles indcate where the variation in risk is most flagrant.
THE NOTION OF VULNERABLE POPULATIONS
One of the major shortcomings of Rose’s approach is that it does not address the underlying mechanisms that lead to different distributions of risk exposure between socially defined groups within populations. Rose rejected Lalonde’s notion of the at-risk group as the primary target for public health interventions. We contend, however, that a focus on vulnerable populations is complementary to a population approach and necessary for addressing social inequalities in health.
The notion of vulnerable populations differs from that of populations at risk. A population at risk is defined by a higher measured exposure to a specific risk factor. All individuals in a population at risk show a higher risk exposure. A vulnerable population is a subgroup or subpopulation who, because of shared social characteristics, is at higher risk of risks. The notion of vulnerable populations refers to groups who, because of their position in the social strata, are commonly exposed to contextual conditions that distinguish them from the rest of the population. As a consequence, a vulnerable population’s distribution of risk exposure has a higher mean than that of the rest of the population.
Although they partly overlap, vulnerable populations are different from populations at risk (Table 2 ▶). The former are defined by shared social characteristics, whereas the latter are characterized by a homogeneously high level of exposure to a single risk factor. The distinction between exposure to single biologically based risk factors and sharing social characteristics is key. Virtually all of the examples used by Rose to illustrate his population approach were based on risk factors for chronic disease that he explained as being largely caused by biological, genetic, or environmental factors.
TABLE 2—
Three Different Public Health Approaches to Improving Health
| Intervention Approach | Objective | Target for Intervention | Critiquesa |
| Populations at risk (Lalonde5) | Prevent disease in those individuals at higher risk | Reduce the specific risk exposure for individuals at higher risk through behavioral (or biochemical) changes | Blames the victim; does not prevent other individuals from becoming at risk |
| Population approach (Rose6) | Increase overall population health | Shift distribution of population risk exposure toward a lower mean through changes in environmental conditions that lead to increased risk | May increase health inequalities |
| Vulnerable populations (this essay) | Decrease health inequalities between socially defined groups | Shift to a lower level the risk exposure distribution of socially defined groups through changes in social and environmental conditions that make groups at higher risk of risks | May lead to positive discrimination; may lead to stigmatization; may be less efficient in terms of population health |
aThe critiques directed at the populations-at-risk approach are empirically documented. The critique listed for the population approach is currently being researched, and those associated with vulnerable populations are speculative.
What we refer to as vulnerable populations, on the other hand, are populations that share social characteristics that put them at higher risk of risks. In Canada, for example, those vulnerable populations whose mean distributions of risk exposure are significantly higher than those of the general population are people of aboriginal descent, those with an income lower than the poverty threshold, and those who have not completed secondary education.18 Although on average people of aboriginal descent show a higher exposure to many risk factors, not everyone in this vulnerable group belongs to the high-risk population for any one risk factor.
The unintended adverse consequence for vulnerable populations of applying Rose’s approach is because of, we believe, a lack of attention to what has been referred to as the “fundamental cause.” According to Link and Phelan,19,20 risk factors and their accumulation are the expression of fundamental causes linked to one’s position in the social structure. These “causes” are the risks that generate exposure to other risks (e.g., low socioeconomic position, being of aboriginal descent, having a low level of education, etc.).
We argue that the fundamental cause mechanism works through 2 correlated pathways, the first of which relates to the life course. Kuh et al.21 showed that a person’s position in a health indicator distribution is the result of all previous experiences, including those that may not be directly related to health. Thus, for instance, not only are children who live in poor families at higher risk of conditions such as uncontrolled asthma (because of differential levels of medical care received as well as differentials in compliance), but the cumulative effect of poor health from childhood into adulthood seems to be higher for people from lower-income families.22,23 By not considering the life trajectory of risk exposure, Rose’s approach is blind to the crucial effect of the life course. The life course tells us that an individual’s position in a distribution is the end product of a life trajectory. Therefore, shifting a distribution implies curbing as many life trajectories as there are individuals in the distribution. There is no reason to assume that curbing individual adverse life trajectories is the same as shifting individual positions in a risk exposure distribution.
The second pathway relates to the concentration of risk. Moderate correlations between several risk factor exposures in the general population may mask highly differentiated experiences in specific subpopulations. Indeed, exposure to multiple risk factors and a greater number of comorbidities are more frequent in some vulnerable populations (e.g., populations with low socioeconomic positions, aboriginal peoples, etc.). By focusing on single risk factors, Rose’s approach cannot account for multiple risk exposure. Vulnerable populations, we argue, are those who concentrate numerous risk factors throughout their life course because of shared fundamental causes associated with their position in the social structure.
Population-approach interventions themselves seem to have abetted the augmentation of social inequalities in health through their unintended effect of concentrating risk in vulnerable populations. It appears from empirical observations that individuals from vulnerable populations are the least able to positively respond to population-approach interventions. This “inverse care law” states that those with the most resources at hand to adapt to new situations will be the first to derive maximum benefits from population-approach interventions.14,20 Population-approach interventions may also have unfortunate effects on vulnerable populations because of incongruities in social and cultural assumptions between public health practitioners and targeted groups.24–26 There is a growing disconnect, for example, between the assumptions that tobacco control practitioners take as self-evident (e.g., the preeminent importance of health, the value of knowledge as a determinant of health)27 and how smokers view their smoking and their health. A recent article by Bottoroff et al.,28 for instance, explores the important role that smoking plays in reinforcing dominant ideals of masculinity for men, particularly those becoming first-time fathers.
CONCLUSION
We have explored the pathways through which the laudable public health objectives of improving the health of the overall population may lead to increasing health disparities between various social groups. That the objective of improving population health may not necessarily be compatible with the objective of reducing health disparities is becoming acknowledged in an increasing number of health policies.29 One way to ensure that vulnerable populations are not left behind in the improvement of population health is to distinguish these objectives and design public health strategies that use both population and vulnerable population approaches to interventions. Many national jurisdictions have adopted policy recommendations that couple the reduction in health disparities with the improvement of overall population health. Such policies can be found in various reports, such as “Integrated Pan-Canadian Healthy Living Strategy,”30 the Swedish “Health on Equal Terms Public Health Policy,”31 and “Tackling Heath Inequalities: A Program for Action” in the United Kingdom.32
There remains the question of what a vulnerable population approach to intervention should look like. Although an authoritative answer is clearly outside the scope of this essay, a tentative answer would identify 2 characteristics for vulnerable population interventions. The first is that such interventions must be based on intersectoral approaches. Fundamental causes that create vulnerability are rooted in everyday life, and their alleviation lies mostly outside of the health sector (the prevention of illiteracy is one case in point). In such cases, the role of the health sector is not so much to invest directly in the transformation of social determinants as to take a leadership role and “engage with other sectors in health disparities’ reduction.”29 The second characteristic is that such interventions should be participatory. Given that one of our critiques of population approaches is that the targeted populations often have different concerns than those of public health promoters, an essential attribute of a vulnerable population approach would be its inclusion of members of vulnerable populations in the articulation of the problem and the development of the program and its evaluation. This is not to say that the vulnerable population approach should be the only one to involve the participation of populations, but it emphasizes that participation is a key intervention feature of this approach.33
Finally, no intervention approach can singly fulfill all public health goals. The more we intervene in the name of the public’s health, the more we learn about the positive and adverse effects of our strategies. A vulnerable population approach to public health is no exception, and it is likely to produce unintended effects. We can only speculate about such adverse effects, as shown in Table 2 ▶. We believe, however, that the notion of vulnerability, as distinct from that of being at risk, offers a useful framework to address the question of health inequalities.
Acknowledgments
L. Potvin holds the Chair on Community Approaches and Health Inequalities funded by the Canadian Health Services Research Foundation and the Canadian Institute of Health Research (CHSRF-CIHR-022605).
The authors are most grateful for insightful comments from Norman Frohlich and S. Leonard Syme.
Peer Reviewed
Contributors The authors were equally responsible for the conceptualization and writing of this essay.
References
- 1.Detels R, Breslow L. Current scope and concerns in public health. In: Detels R, McEwen J, Beaglehole R, Tanaka H, eds. The Scope of Public Health. 4th ed. Oxford, England: Oxford University Press; 2002:3–20. Oxford Textbook of Public Health; vol 1.
- 2.Goel V. Socioeconomic status and cancer incidence and survival. Cancer Prev Control. 1998;2:211–212. [PubMed] [Google Scholar]
- 3.Choinière R, Lafontaine P, Edwards AC. Distribution of cardiovascular disease risk factors by socioeconomic status among Canadian adults. CMAJ. 2001; 162:S13–S24. [PMC free article] [PubMed] [Google Scholar]
- 4.Heymann D. Infectious agents. In: Detels R, McEwen J, Beaglehole R, Tanaka H, eds. The Scope of Public Health. 4th ed. Oxford, England: Oxford University Press; 2002:171–194. Oxford Textbook of Public Health; vol 1.
- 5.Lalonde M. A new perspective on the health of Canadians. 1974. Available at: http://www.hc-sc.gc.ca/hcs-sss/alt_formats/hpb-dgps/pdf/pubs/1974-lalonde/lalonde_e.pdf. Accessed October 22, 2007.
- 6.Rose G. The Strategy of Preventive Medicine. Oxford, England: Oxford University Press; 1992.
- 7.Dawber TR. The Framingham Study: The Epidemiology of Atherosclerotic Disease. Cambridge, Mass: Harvard University Press; 1980.
- 8.Labonté R. Death of program, birth of metaphor: the development of health promotion in Canada. In: Pederson A, O’Neill M, Rootman I, eds. Health Promotion in Canada. Provincial, National & International Perspectives. Toronto, Ontario: W.B. Saunders; 1994:72–90.
- 9.Syme SL. The social environment and health. Daedalus. Fall 1994:79–86.
- 10.McKinlay JB. The promotion of health through planned sociopolitical change: challenges for research and policy. Soc Sci Med. 1993;36:109–117. [DOI] [PubMed] [Google Scholar]
- 11.Rose G. Sick individuals and sick populations. Int J Epidemiol. 1985;14: 32–38. [DOI] [PubMed] [Google Scholar]
- 12.Cronin H. The Ant and the Peacock. Cambridge, England: Cambridge University Press; 1991.
- 13.Katz SJ, Hofer TP. Socioeconomic disparities in preventive care persist despite universal coverage: breast and cervical cancer screening in Ontario and the United Kingdom. JAMA. 1994; 272:530–534. [PubMed] [Google Scholar]
- 14.Victora CG, Barros FC, Vaughan JP. The impact of health interventions on inequalities: infant and child health in Brazil. In: Leon D, Walt G, eds. Poverty, Inequality and Health. Oxford, England: Oxford University Press; 2001: 125–136.
- 15.Federico B, Costa G, Kunst AE. Educational inequalities in initiation, cessation, and prevalence of smoking among 3 Italian birth cohorts. Am J Public Health. 2007;97:838–845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Barbeau EM, Krieger N, Soobader MJ. Working class matters: socioeconomic disadvantage, race/ethnicity, gender, and smoking in NHIS 2000. Am J Public Health. 2004;94:269–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.The National Strategy: Moving Forward. The 2005 Progress Report on Tobacco Control. Prepared by the Tobacco Control Liaison Committee of the Federal-Provincial Territorial Advisory Committee on Population Health and Health Security in collaboration with non-governmental organizations, 2005. Available at: http://www.hc-sc.gc.ca/hl-vs/alt_formats/hecs-sesc/pdf/pubs/tobac-tabac/foward-avant/foward-avant_e.pdf. Accessed October 22, 2007.
- 18.Frohlich KL, Ross N, Richmond C. Health disparities in Canada today: evidence and pathways. Health Policy. 2006;79:132–143. [DOI] [PubMed] [Google Scholar]
- 19.Link BG, Phelan J. Social conditions as fundamental causes of diseases. J Health Soc Behav. 1995;(spec no.): 80–94. [PubMed]
- 20.Phelan J, Link B. Controlling disease and creating disparities: a fundamental cause perspective. J Gerontol B Psychol Sci Soc Sci. 2005;60(spec no.): 27–33. [DOI] [PubMed] [Google Scholar]
- 21.Kuh D, Power C, Blane D, Bartley M. Social pathways between childhood and adult health. In: Kuh D, Ben-Shlomo Y, eds. A Life Course Approach to Chronic Disease Epidemiology. Oxford, England: Oxford University Press; 1997:169–198.
- 22.Kuh D, Ben-Shlomo Y, eds. A Life Course Approach to Chronic Disease Epidemiology. Oxford, England: Oxford University Press; 1997.
- 23.Power C, Matthews S. Origins of health inequalities in a national population sample. Lancet. 1997;350: 1584–1589. [DOI] [PubMed] [Google Scholar]
- 24.Laurier E, McKie L, Goodwin N. Daily and lifecourse contexts of smoking. Sociol Health Illn. 2000;22:289–309. [Google Scholar]
- 25.Krumeich A, Weijts W, Reddy P, Meijer-Weitz A. The benefits of anthropological approaches for health promotion research and practice. Health Educ Res. 2001;16:121–130. [DOI] [PubMed] [Google Scholar]
- 26.Garcia A. Is health promotion relevant across cultures and the socioeconomic spectrum? Fam Community Health. 2005;29:20S–27S. [DOI] [PubMed] [Google Scholar]
- 27.Caplan R. The importance of social theory for health promotion: from description to reflexivity. Health Promot Int. 1993;8:147–157. [Google Scholar]
- 28.Bottoroff JL, Oliffe J, Kalaw C, Carey C, Mroz L. Men’s constructions of smoking in the context of women’s tobacco reduction during pregnancy and postpartum. Soc Sci Med. 2006;62: 3096–3108. [DOI] [PubMed] [Google Scholar]
- 29.Health Disparities Task Group of the Federal/Provincial/Territorial Advisory Committee on Population Health and Health Security. Reducing Health Disparities—Roles of the Health Sector. Discussion paper, 2005. Available at: http://www.phac-aspc.gc.ca/ph-sp/disparities/pdf06/disparities_recommended_policy.pdf. Accessed January 4, 2008.
- 30.Secretariat for the Healthy Living Network. The integrated pan-Canadian healthy living strategy, 2005. Available at: http://www.phac-aspc.gc.ca/hl-vs-strat/pdf/hls_e.pdf. Accessed October 18, 2007.
- 31.Hogstedt C, Lundgren B, Moberg H, Pettersson B, Ågren G. Forward. Scand J Public Health. 2004;32:3. [PubMed] [Google Scholar]
- 32.Tackling Health Inequalities: A Program for Action. London, England: UK Department of Health; 2003.
- 33.Potvin L. Managing uncertainty through participation. In: McQueen DM, Kickbusch I, Potvin L, Pelikan JM, Balbo L, Abel T, eds. Health & Modernity: The Role of Theory in Health Promotion. New York, NY: Springer; 2007:103–128.