

Abstract
Emotional eating has often been linked to overweight and/or obesity. Multiple group SEM analyses were conducted using cross-sectional data from 517 minority students in Los Angeles County. Results showed no differences in emotional eating between normal weight and overweight students. Perceived stress was indeed a significant correlate of emotional eating, independent of BMI status, as indicated by the lack of a modifying effect of BMI status. Findings highlight the fact that emotional eating is not an issue only for overweight and obese persons. This study shows that some children in this population at increased risk for obesity and related chronic disease have already incorporated emotional eating as a learned response to stress by the time that they enter adolescence.
Keywords: Emotional eating, perceived stress, adolescents, moderation, structural equation model, BMI
1. Introduction
Within the domain of emotional eating there is a subset of literature on stress-induced eating. Two models of thought exist within this body of literature, the General Effects and Individual Differences models (Greeno & Wing, 1994). The former has been tested predominantly in animals and the latter has exclusively been studied in humans. According to the General Effects Model, all organisms will increase intake in response to stress. The Individual Differences Model posits that certain factors of the individual will dictate whether or not stress leads to eating. One of the main hypotheses of the Individual Differences Model that has been tested is that obese individuals are more likely to engage in stress-induced eating than normal weight individuals (Greeno & Wing, 1994).
In their review of stress-induced eating, Greeno and Wing (1994) concluded that stress does indeed often lead to overeating, and that future studies should continue on the individual differences model and explore this phenomenon in samples with males, non-adult populations, and in non-lab settings. Michaud and colleagues (1990) found that stress increased food intake in a sample of French high school students and concluded that this behavior could bring about increased body weight over time. A lab study of 8–11 year olds reported the moderating effect of restraint on the association between stress and snacking, where those higher in restraint (conscious control of energy intake) were more likely to eat in the face of stress, which could lead to weight gain when restraint was broken (Roemich, Wright, & Epstein, 2002). Cartwright et al.’s (2003) examination of seventh graders in London revealed that higher perceived stress was related to higher consumption of fat and unhealthy amounts of snacking. The authors concluded that this behavior could result in obesity.
The theory from which most discussions of emotional eating stem is the Psychosomatic Theory of Obesity. According to this theory, food is used as an emotional defense in the face of negative affect, which causes overconsumption which, in turn, leads to obesity (Kaplan & Kaplan, 1957). In addition, it is posited that obese individuals excessively eat in response to these negative emotional states, while normal weight persons do not eat in the face of distress and instead employ other coping mechanisms (Faith, Allison, & Geliebter, 1997). For this reason, many emotional eating studies focus on obese persons.
However, support for the Psychosomatic Theory has not been consistent. Emotional eating was not related to body mass index (BMI) in a British adolescent sample, however findings did show that perceived fatness was related to emotional eating (Wardle et al., 1992). A study of binge-eating and obesity found that emotional eating was positively associated with binge-eating, and binge eating was predictive of obesity (but negative affect alone was not related to BMI) (Stice, Presnell, & Spangler, 2002). In a sample of 9–12 year olds from Belgium, Braet and van Strien (1997) found that overweight and obese children scored significantly higher on emotional eating than normal weight children.
Of the studies cited above, only two were conducted in the United States and none were conducted within minority populations. Latinos are a population at high risk for overweight and obesity (Hedley et al., 2004). Considering the focus on weight and body appearance in the U.S. and the high risk for overweight in Latino populations, it seems warranted to explore emotional eating as a potentially modifiable risk factor in this population.
In order to examine the Psychosomatic Theory and the Obesity Hypothesis of the Individual Differences Model of Stress-induced Eating in a minority adolescent population, a cross-sectional analysis of the moderating effects of BMI on the relationship between perceived stress and emotional eating was undertaken. According to theory, it is expected that perceived stress will be significantly associated with emotional eating in overweight and obese students only. This association is not expected to be significant for the normal weight group. The conceptual model for these analyses is presented in Figure 1. It was further anticipated that overweight participants would be more likely to emotionally eat than those of normal weight and for there to be a larger proportion of emotional eaters in the overweight group than the normal weight group.
Figure 1.
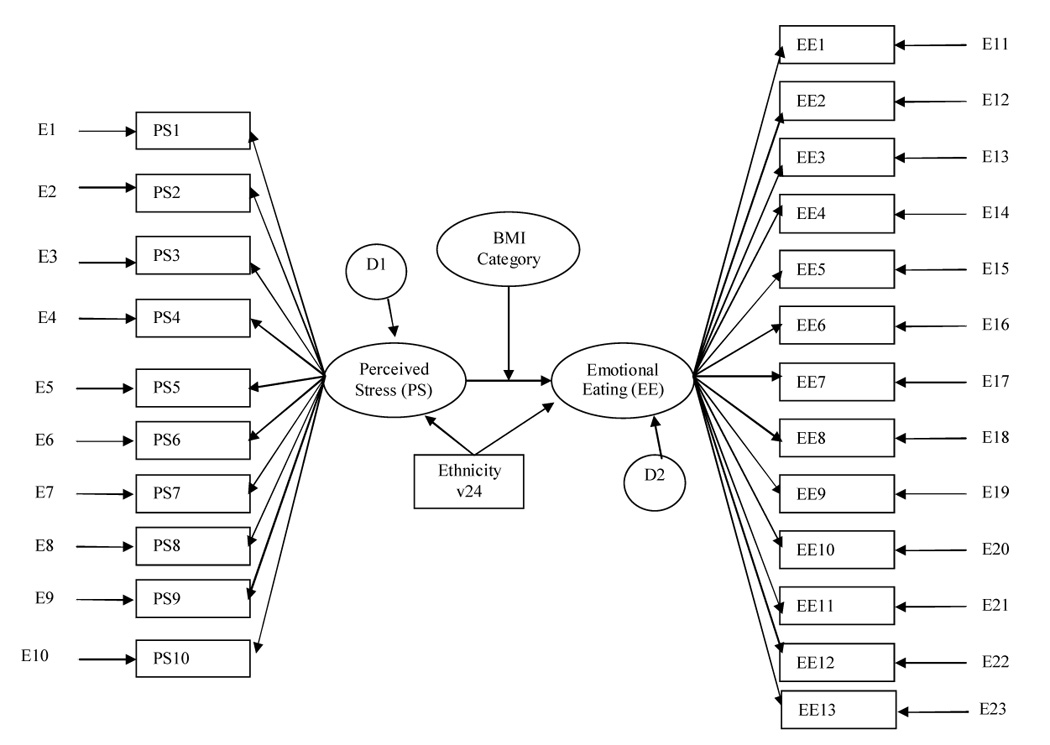
SEM moderation model
2. Method
2.1 Sample
Six-hundred and seventeen students from public and private Los Angeles County middle schools provided data for the present analysis. Students were primarily of Latino ethnicity and were in grades seven and eight. Confidential questionnaires were administered, assessing demographics, psychosocial factors and behavior, including perceived stress and emotional eating.
2.2 School selection
School selection aimed to obtain a predominantly Latino sample from the underlying Los Angeles County population. Data from the California Board of Education and Roman Catholic Archdiocese were employed to identify ethnic distributions of the school. A school sample representing the range of socioeconomic status was desired; therefore this data was also used in the selection criteria for schools in order to obtain a sample of mostly Latino students and a wide range of SES. Eight of nine schools that fit selection criteria agreed to participate. Just prior to the commencement of data collection, one school was unable to participate due to school district mandates for time spent in remedial reading, therefore, a total of seven schools participated in the study.
2.3 Student recruitment
Classrooms were identified by approaching instructors of physical education classes. Only one of the teachers approached was unable to participate due to scheduling issues. All students in the seventeen classes that agreed to participate were invited to take part in the study. The study was explained to potential participants and parental consent forms were distributed on the first day of recruitment. On the third day of recruitment, separate parent refusal forms were distributed to those that had not returned a parental permission consent form. On the fourth day, any remaining consent and refusal forms were collected, and surveys were distributed to those eligible to participate. Data collection continued the next day (day 5) at schools where extra time was needed to complete surveys.
Students were eligible to complete the full survey if they provided active parental consent and personal assent. If students did not return an active parent refusal and gave student assent, they were allowed to take an IRB approved abbreviated survey. Those that had active refusal or did not provide personal assent did not take part in the study. All parent forms were available in both English and Spanish. These consenting and all other procedures were approved by the University Institutional Review Board as well as appropriate school boards. Eighty-five percent of students provided either active (i.e., parent provided written consent) or implied (i.e., parent did not provide written refusal) consent to participate in the study.
2.4 Procedure
According to procedures outlined in data collection manuals and scripts, trained data collectors measured height and weight, and distributed and picked up all surveys. On average, the survey took approximately 45 minutes to complete, however data collection may have taken place across two class periods depending on length of the class period. All surveys were in English only; this is because students were assumed to be sufficiently proficient in English since all classes are taught only in English and, in our experience with Latino adolescents in Los Angeles, less that 1% of have chosen a Spanish language survey when given a choice. In the few cases where it was needed, schools did provide a translator if possible, otherwise data collectors could also translate. All surveys were completely confidential, identified only by a unique ID number.
2.5 Measures
Emotional eating
The subscale from van Strien’s (1986) Dutch Eating Behavior Questionnaire (DEBQ) was used to measure emotional eating. This scale assesses eating in response to specific and diffuse emotions with 13 items, using a 5-point Likert scale response format, ranging from “never” to “very often.” Scale scores are obtained by calculating the mean of responses (Cronbach α = 0.95).
Perceived stress
The Perceived Stress Scale was employed to assess perceived stress (Cohen, Kamarck, & Mermelstein, 1983). This scale was modified based on short interviews conducted with adolescents, where wording changes were made to increase understanding and 3 items were added. Therefore, a total of 17 items were included, with responses ranging from “never” to “very often” in a Likert response format. A sum of items is used as the perceived stress score (Cronbach α = 0.72). This scale was reduced to 10-items (rationale for obtaining a smaller number of items is explained below) in order to optimize structural equation model analysis. Reliability analyses showed that Cronbach’s alpha (α = 0.89) was better for this reduced scale.
Body Mass Index
A Tanita body composition analyzer (TBF-300A) was used to measure weight in kilograms. A standard measuring instrument (stadiometer) was used to measure height in centimeters (nearest whole number). Body Mass Index (BMI) was calculated from these measurements (weight in kilograms divided by height in meters squared). The 2000 Centers for Disease Control and Prevention (CDC) age and gender growth charts were used to calculate BMI percentiles (Pietrobelli et al., 1998). BMI percentiles are used in pediatric populations in lieu of BMI in order to take into account age and gender factors of BMI while children are still growing and developing. According to the CDC cut-points, those below the 5th percentile are underweight, while those at the 85th and below the 95th percentiles are considered at risk for overweight and those at or above the 95th percentile are categorized as overweight. Because there were very few underweight participants in this sample, they were excluded from analyses. BMI was categorized into normal weight vs. at risk for overweight and overweight participants combined (Wang, 2001). For ease of discussion, the latter group is referred to as the overweight group throughout this paper, although this should not indicate that those at risk for overweight should be labeled as overweight.
Ethnicity
Ethnic background of participants was determined using an ethnicity scale developed by Phinney (Phinney, 1992). This instrument presents a range of ethnicities and participants are asked to mark all that apply. If more than one ethnicity was checked off, the participant was categorized as Multi-ethnic. Ethnic groups with very small numbers were combined into an “Other” category. To obtain similar group sizes for analyses, groups were combined and coded as “Latino” and “non-Latino.”
2.6 Data analysis
Descriptive statistics for the sample were obtained by computing means and frequencies of demographic data. T-tests were used to test for mean differences between weight groups in perceived stress and emotional eating. Differences in the proportion of emotional eaters in the BMI groups were tested using chi-square analyses. Multilevel regression analyses were used to identify covariates to be included in the structural equation model (SEM) analyses. Exploratory factor analyses were used to reduce the number of items for each construct, as Bentler & Chou (1987) suggest limiting the number of variables in a data set in order to minimize issues of poor measurement structure, with caution not to exclude key variables.
Although moderation can be assessed via regression analyses, SEM offers an approach to obtain results with reduced bias. Due to measurement error not accounted for and inability to estimate reciprocal effects in regression analysis (potentially resulting in underestimated effect sizes), SEM is ideal because measurement error in the variables are statistically controlled, it allows for the measurement of reciprocal effects, and it assesses overall model fit (Peyrot, 1996). Model fit is important because it gives us information about the suitability of the model to our data. SEM allows for a simultaneous test of all variables in the model in order to assess model fit. If a good model fit is found, this offers support for the theorized model (Byrne, 1994).
In addressing the issue of nested data, multilevel SEM was considered for analyses. Intraclass correlation (ICC) coefficients provide an estimate of the degree of commonality in observations within a given unit, in this case school. Conventional single-level analytical approach is inadequate to obtain valid statistical results when the ICC is large. Murray and Blitstein (2003) have reported that the school-level ICCs for the majority of health behaviors is less than 0.05 indicating low degree of dependence in observations. Therefore, ICCs were calculated for variables in the model and all were found to be less than 0.05. Furthermore, techniques for multi-level SEM are still under development and not yet well understood. Therefore single level SEM was the method of analyses for this study.
Confirmatory factor analysis
The relationship of the indicators to their respective latent factors was empirically assessed through confirmatory factor analyses. Empirical data were used to statistically test the hypothesized model in order to confirm the adequacy of indicator variables used to represent the proposed latent factors. Factor loadings of indicator variables were expected to have high loadings on their respective factors and to be significant in order to show evidence of convergent validity. Following inspection of confirmatory factor analysis results to verify the presence of distinct constructs, causal pathways were inserted to delineate the relationship between perceived stress and emotional eating. Testing of the structural model was then performed.
Model fit
Assessment of model fit was performed using the goodness-of-fit χ2 test statistic as well as the comparative fit index (CFI) and the root mean squared error of approximation (RMSEA); a CFI of 0.9 or more and an RMSEA of < 0.05 is considered to be a good fit (Browne & Cudeck, 1993; Kline, 1998). The maximum-likelihood estimation procedure was employed as a global test of the model (Bentler, 1990). Distributions of all variables were checked for normality via kurtosis and skewness statistics. Robust estimates were obtained in order to deal with violations of the normal distribution assumption. The Lagrange Modifier (LM) test was utilized to identify parameters that would improve model fit. To preserve the theoretical factor structure of all the measures, only error covariances that were consistent with theory were added to the model.
Testing for model invariance
Good model fit was obtained for the two weight groups separately. Using the multiple group approach SEM procedure, these models were combined to test for invariance of factor loadings between the normal weight and overweight groups. Invariance of the factor loadings assures that factors can be treated the same between the two weight groups. Upon obtaining good model fit, invariance of the regression weight between the two groups was the focus of the test for moderation. In order to do this, the path between perceived stress and emotional eating was constrained to be equal across groups (Peyrot, 1996). If the model fit remained, there was no moderating effect, since this would indicate that the same model fits for both groups, with the same path coefficients. However, if the model fit was lost with this added constraint, this would mean that there was a significant weight status interaction. The Chi-square difference test was used to test the significance of the change in model fit.
3. Results
517 (84%) of the 617 students who participated in the survey had complete data on perceived stress and emotional eating and were of at least normal weight. There were significant differences between those with complete data vs. those without complete data; among those with complete data there were less boys (23.9% vs. 34.6%), and they scored higher on perceived stress (Mcomplete = 17.45, SD = 8.72; Mincomplete = 9.67, SD = 11.00; p = 0.005) and emotional eating (Mcomplete = 1.92, SD = 0.92; Mincomplete = 1.58, SD = 0.82; p < 0.001) than those with incomplete data. There were no significant differences in BMI percentile between those included in analyses and those excluded (p = 0.527). Table 1 and Figure 2 display sample characteristics.
Table 1.
Characteristics of the sample
| Variable | Overall | Normal weight | Overweight | ||||
|---|---|---|---|---|---|---|---|
| N = 517 | N=301 (58%) | N=216 (42%) | Range | ||||
| M | (SD) | M | (SD) | M | (SD) | ||
| Age | 12.51 | (0.66) | 12.54 | (0.68) | 12.47 | (0.63) | 11–15 |
| Femalea | 392 | (75.8) | 236 | (78.4) | 156 | (72.2) | |
| Ethnicitya | |||||||
| Asian/PI | 91 | (17.6) | 66 | (21.9) | 25 | (11.6) | (11.6) |
| Latino | 319 | (61.7) | 165 | (54.8) | 154 | (71.3) | |
| Multi-ethnic | 57 | (11.0) | 41 | (13.6) | 16 | (7.4) | |
| Other | 31 | (6.0) | 20 | (6.6) | 11 | (5.1) | |
| White | 19 | (3.7) | 9 | (3.0) | 10 | (4.6) | |
| Perceived Stress | 15.98 | (9.17) | 17.04 | (9.08) | 16.89 | (9.30) | 0–40 |
| Emotional Eating | 1.90 | (0.92) | 1.96 | (0.96) | 1.81 | (0.86) | 1–5 |
| BMI Percentile | 68.95 | (27.67) | 50.82 | (22.69) | 94.21 | (4.20) | 5.1–99.8 |
N (%)
Figure 2.
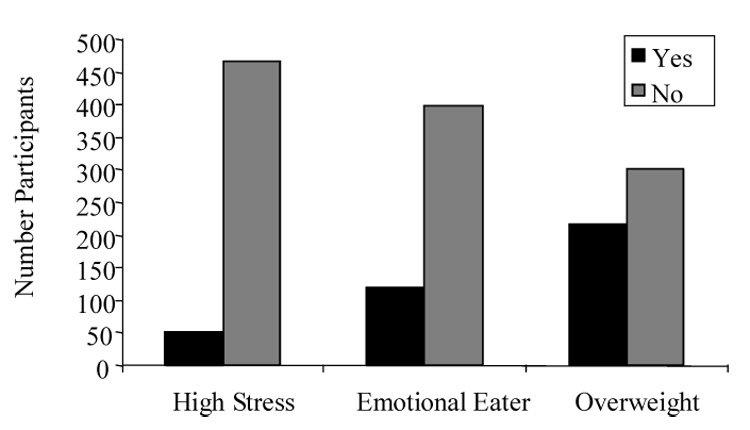
Stress, emotional eating and BMI status
T-tests revealed no significant differences in perceived stress (t = 0.19, p = 0.85) or emotional eating (t = 1.84, p = 0.07) between the normal weight group and the overweight group. Further, chi-square analyses revealed that there was a larger proportion of emotional eaters in the normal weight group than in the overweight group (χ2 = 4.24; p = 0.03). Twenty-six percent of normal weight participants were categorized as emotional eaters vs. 18% of overweight participants; 66% of those categorized as emotional eaters were of normal weight. Results from the regression analyses showed that ethnicity should be included in the SEM model analysis.
Factor analysis
The measurement model was tested using confirmatory factor analyses. Results show that all variables loaded high on their respective factors and all factor loadings were significant. This serves as evidence of construct and convergent validity. Distributions of all variables appeared to be normal, as kurtosis and skewness statistics were quite low. Nonetheless, robust estimates were also computed and showed no significant differences; therefore results from ML procedures were used.
Multiple group approach structural equation model analyses
Results of the development of the models are summarized in Table 2. The basic theoretical model was tested for normal weight and overweight groups separately. These base models did not yield a statistically satisfactory fit to the data nor good fit based on the fit indices. Therefore, model modification was guided by the LM test to obtain good model fit for the two groups.
Table 2.
Summary results of model development and tests of invariance
| Group | χ2 | df | p | CFI | RMSEA |
|---|---|---|---|---|---|
| Normal Weight | |||||
| MN0 | 478.85 | 250 | < .00001 | .934 | .055 |
| MN1 | 406.44 | 249 | < .00001 | .955 | .046 |
| Overweight | |||||
| MO0 | 417.41 | 250 | < .00001 | .915 | .056 |
| MO1 | 386.66 | 249 | < .00001 | .930 | .051 |
| MO2 | 377.91 | 248 | < .00001 | .934 | .049 |
| Combined | |||||
| M0 | 784.63 | 497 | < .00001 | .946 | .047 |
| M1 | 812.90 | 518 | < .00001 | .945 | .047 |
| M1-M0 | 28.27 | 21 | .1327 | ||
| M2 | 815.03 | 519 | < .00001 | .944 | .047 |
| M2-M1 | 2.13 | 1 | .1440 |
Note. MN0 and MO0 = basic theoretical models for normal weight (N = 301) and overweight (N = 216) groups, respectively. MN1 and MO1 = modified models with common correlated errors suggested by the LM test on MN0 and MO0, respectively. MO2 and MO3 = modified models with correlated errors suggested by the LM test on MO1. M0 = basic model combining normal and overweight groups. M1 = model with all factor loadings constrained to be equal across groups. M2 = model with all factor loadings and regression weight constrained to be equal across groups.
Common correlated errors were identified from the LM test to begin modification. After the first modification, the model for the normal weight group showed satisfactory model fit, based on the fit indices. SEM Model 1 for the normal weight group yielded a χ2 = 406.44 (df = 249), p < .00001, CFI = .955, and RMSEA = 0.046. The LM test did not show any more common correlated errors, therefore the above SEM model was treated as the final model for the normal weight group, and was used for subsequent multiple group approach. One more correlated error, consistent with theory, was added to the model for the overweight group to obtain good model fit. The final SEM for the overweight group yielded a χ2 = 377.91 (df = 248), p < .00001, CFI = .934, and RMSEA = 0.049. Tests of model invariance followed.
A base model combining the final models for each the two groups was tested, yielding χ2 = 784.63 (df = 497), p < .00001, CFI = .946, and RMSEA = 0.047. An M1 model was then developed with all factor loadings constrained to be equal across groups, yielding χ2 = 812.90 (df = 518), p < .00001, CFI = .945, and RMSEA = 0.047. A likelihood ratio test on the change in chi-square was performed and there was no significant difference between the base model and the fully constrained M1 model (p = 0.13), therefore the fully constrained model was retained. Acceptance of M1 model indicated that the measurements are invariant between the two weight groups.
In order to test for the moderating effect of BMI category, the regression weight between the two factors was constrained to be equal across groups. The M2 model yielded χ2 = 815.03 (df = 519), p < 0.00001, CFI = .944, and RMSEA = 0.047. There was no change in chi-squares showing that there was no significant difference between Model 1 and Model 2 (p = 0.14). Therefore, the fully constrained Model 2 was retained as the final model; estimates for this model are presented in Table 3. These analyses indicate that perceived stress is significantly related to emotional eating, but that BMI was not a significant moderator of the relationship.
Table 3.
Parameters of final model
| Item | Factor Loading (SE)a | Error Variance (SE) | Reliabilityb | ||
|---|---|---|---|---|---|
| Normal weight | Over-weight | Normal weight | Over-weight | ||
| Perceived Stress | |||||
| PS1 | 1.000c | 0.828 (.073) | 0.942 (.097) | 0.553 | 0.568 |
| PS2 | 1.148 (.076) | 0.641 (.060) | 0.692 (.076) | 0.421 | 0.423 |
| PS3 | 1.226 (.082) | 0.874 (.080) | 0.791 (.087) | 0.465 | 0.423 |
| PS4 | 0.981 (.066) | 0.588 (.054) | 0.511 (.056) | 0.477 | 0.426 |
| PS5 | 1.101 (.077) | 0.775 (.070) | 0.878 (.093) | 0.488 | 0.502 |
| PS6 | 0.736 (.073) | 1.216 (.102) | 1.307 (.129) | 0.770 | 0.771 |
| PS7 | 1.234 (.077) | 0.529 (.053) | 0.581 (.067) | 0.341 | 0.347 |
| PS8 | 1.052 (.076) | 0.958 (.084) | 0.766 (.081) | 0.564 | 0.491 |
| PS9 | 0.997 (.080) | 1.125 (.097) | 1.237 (.126) | 0.628 | 0.635 |
| PS10 | 0.997 (.077) | 0.976 (.085) | 1.064 (.109) | 0.594 | 0.598 |
| Emotional Eating | |||||
| EE1 | 1.000c | 0.783 (.066) | 0.423 (.044) | 0.520 | 0.402 |
| EE2 | 0.908 (.069) | 1.208 (.101) | 1.008 (.100) | 0.669 | 0.660 |
| EE3 | 1.219 (.066) | 0.674 (.059) | 0.475 (.051) | 0.385 | 0.337 |
| EE4 | 1.111 (.060) | 0.556 (.048) | 0.405 (.043) | 0.384 | 0.343 |
| EE5 | 1.197 (.061) | 0.361 (.033) | 0.414 (.044) | 0.258 | 0.315 |
| EE6 | 1.021 (.058) | 0.522 (.045) | 0.454 (.047) | 0.409 | 0.409 |
| EE7 | 1.161 (.057) | 0.235 (.023) | 0.391 (.042) | 0.194 | 0.315 |
| EE8 | 1.070 (.059) | 0.547 (.048) | 0.406 (.043) | 0.398 | 0.360 |
| EE9 | 1.116 (.057) | 0.402 (.036) | 0.310 (.034) | 0.308 | 0.283 |
| EE10 | 0.930 (.053) | 0.434 (.038) | 0.480 (.049) | 0.409 | 0.469 |
| EE11 | 1.128 (.057) | 0.316 (.029) | 0.399 (.043) | 0.255 | 0.332 |
| EE12 | 1.220 (.063) | 0.385 (.035) | 0.583 (.061) | 0.264 | 0.383 |
| EE13 | 1.017 (.070) | 1.066 (.090) | 0.971 (.097) | 0.588 | 0.599 |
Corresponding factor loadings were constrained equal between the two weight groups. Only one factor loading now reported.
Reliability is equal to 1 – R-squared.
Factor loading for first variable of each factor was fixed at one.
4. Discussion
This test of the effects of weight status on the relationship between perceived stress and emotional eating showed that BMI is not a moderator of this significant positive relationship. Furthermore, there were no differences found in level of emotional eating by overweight and normal weight participants; and the proportion of emotional eaters was higher in the normal weight group than in the overweight group. These findings are inconsistent with those that have found an association between weight and emotional eating, e.g., Ganley (1989). They do not support the conjectures of the Psychosomatic Theory nor of the Obesity hypothesis of the Individual Differences Model of Stress-induced Eating, nor with the a priori hypothesis stated for this paper. Results do lend further support though for the Individual Differences Model which states that individual differences account for why some people eat in the face of stress while others do not.
These findings indicate that the relationship between emotional eating and weight may be more complicated than previously thought. It seems that eating may be a coping strategy used by people of all weights, however those who keep their weight within the normal range may possess certain protective qualities or engage in other compensatory behaviors. For example, when one overeats due to stress, they may eat less the next day, or take a walk to make up for the extra caloric intake. Another possibility is that people of normal weight overeat to a lesser degree than people who are overweight, i.e. the amount of intake during overeating may differ between these groups. Yet another possibility is that persons in this sample have not yet become overweight, but if this emotional eating behavior continues, it may still lead to overweight. Future studies could make a substantial contribution to the literature through exploration of potential mediating factors of the relationship between BMI and emotional eating.
The fact that perceived stress and emotional eating scores were significantly higher for participants in these analyses than those not included in the analyses may have affected results of the study. These differences may have resulted if those scoring lower on stress were more likely to not experience negative emotions therefore may have skipped items on the emotional eating scale that they did not think applied to them. It is possible that those with lower scores on the constructs of interest may have been distributed across weight groups in such a way that, if included in analyses, may have made the relationship between perceived stress and emotional eating non-significant in one or both of the weight groups. However, this seems unlikely, and there were also no significant differences in BMI percentile between those with complete data vs. those that did not.
Causality cannot be deduced from these analyses due to their cross-sectional nature. It is quite plausible that emotional eating may lead to the experience of stress. However, as indicated by the definition of emotional eating, eating in response to negative affect, it makes theoretical sense to look at the association as perceived stress leading to emotional eating.
Another potential limitation of this study was that the psychological data are self-reported which can threaten the validity of the data. Because we used validated self-report instruments widely used in the literature we feel confident that we obtained good data from our participants. Data collectors also emphasized the confidentiality of all answers; therefore we do not believe that participants would not have accurately reported data.
An important strength of this study is that it addressed the issues of BMI and emotional eating in a predominantly Latino adolescent sample, a community at high risk for obesity (Hedley 2004). The analysis methods used also increase confidence in findings as SEM analyses provide estimates based on a simultaneous test of all model parameters with reduced measurement bias.
Findings further support the association between perceived stress and emotional eating, and highlight the fact that emotional eating is not an issue only for overweight and obese persons. This brings to light the importance of providing our youth with more adaptive coping skills than turning to food in the face of stress. Learning healthy coping strategies during this time period is crucial as this is a critical time point at which health behaviors begin to solidify and may track into adulthood. This study shows that some children in this population at increased risk for obesity and related chronic disease have already incorporated emotional eating as a learned response to stress by the time that they enter adolescence. Therefore, further investigation of means of ameliorating this problem eating behavior certainly seems warranted.
5. Acknowledgements
We would like to thank the funding agencies that have made this research possible: National Institutes of Health (NIH), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK, Grant # KO1 DK59293-01)
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Bentler P. Comparative fit indexes in structural models. Psychological Bulletin. 1990;107:238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Bentler PM, Chou C-P. Practical issues in structural modeling. Sociological Methods & Research. 1987;16:78–117. [Google Scholar]
- Browne M, Cudeck R. Alternative ways of assessing model fit. In: Bollen K, Long J, editors. Testing structural equation models. Newbury Park: Sage Publications; 1993. pp. 136–162. [Google Scholar]
- Byrne B. Structural Equation Modeling with EQS and EQS/Windows: Basic concepts, applications, and programming. Thousand Oaks: Sage Publications; 1994. [Google Scholar]
- Cartwright M, Wardle J, Steggles N, Simon AE, Croker H, Jarvis MJ. Stress and dietary practices in adolescents, Health Psychology. 2003;22:362–369. doi: 10.1037/0278-6133.22.4.362. [DOI] [PubMed] [Google Scholar]
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of Health & Social Behavior. 1983;24:385–396. [PubMed] [Google Scholar]
- Faith MS, Allison DB, Geliebter A. Emotional eating and obesity: Theoretical considerations and practical recommendations. In: Dalton S, editor. Overweight and weight management: The health professional's guide to understanding and practice. Gaithersburg, Md: Aspen Publishers; 1997. pp. 439–465. [Google Scholar]
- Ganley RM. Emotion and eating in obesity: A review of the literature. International Journal of Eating Disorders. 1989;8:343–361. [Google Scholar]
- Greeno CG, Wing RR. Stress-induced eating. Psychological Bulletin. 1994;115:444–464. doi: 10.1037/0033-2909.115.3.444. [DOI] [PubMed] [Google Scholar]
- Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002. Journal of the American Medical Association. 2004;291:2847–2850. doi: 10.1001/jama.291.23.2847. [see comment] [DOI] [PubMed] [Google Scholar]
- Kaplan HI, Kaplan H. The psychosomatic concept of obesity. Journal of Nervous & Mental Disease. 1957;125:181–200. doi: 10.1097/00005053-195704000-00004. [DOI] [PubMed] [Google Scholar]
- Kline R. Principles and Practices of Structural Equation Modeling. New York, NY: Guilford Press; 1998. [Google Scholar]
- Michaud CI, Kahn JP, Musse N, Burlet C, Nicolas JP, Mejean I. Relationships between a critical life event and eating behaviour in high school students. Stress Medicine. 1990;6:57–64. [Google Scholar]
- Murray DM, Blitstein JL. Methods to reduce teh impact of intraclass correlation in group-randomized trials. Evaluation Research. 2003;27:79–103. doi: 10.1177/0193841X02239019. [DOI] [PubMed] [Google Scholar]
- Peyrot M. Causal analysis: theory and application. Journal of Pediatric Psychology. 1996;21:3–24. doi: 10.1093/jpepsy/21.1.3. [DOI] [PubMed] [Google Scholar]
- Phinney JS. The multigroup ethnic identity measure: A new scale for use with diverse groups. Journal of Adolescent Research. 1992;7:156–176. [Google Scholar]
- Pietrobelli A, Faith M, Allison D, Gallagher D, Chiumello G, Heymsfield S. Body mass index as a measure of adiposity among children and adolescents: a validation study. Journal of Pediatrics. 1998;132:204–210. doi: 10.1016/s0022-3476(98)70433-0. [DOI] [PubMed] [Google Scholar]
- Roemich JN, Wright SM, Epstein LH. Dietary restraint and stress-induced snacking in youth. Obesity Research. 2002;10:1120–1126. doi: 10.1038/oby.2002.152. [DOI] [PubMed] [Google Scholar]
- Stice E, Presnell K, Spangler D. Risk factors for binge eating onset in adolescent girls: a 2-year prospective investigation. Health Psychology. 2002;21:131–138. [PubMed] [Google Scholar]
- van Strien T, Frijters JER, Bergers GPA, Defares PB. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. International Journal of Eating Disorders. 1986;5:295–315. [Google Scholar]
- Wang Y. Cross-national comparison of childhood obesity: the epidemic and the relationship between obesity and socioeconomic status. International Journal of Epidemiology. 2001;30:1129–1136. doi: 10.1093/ije/30.5.1129. [DOI] [PubMed] [Google Scholar]
- Wardle J, Marsland L, Sheikh Y, Quinn M, Fedoroff I, Ogden J. Eating style and eating behaviour in adolescents. Appetite. 1992;18:167–183. doi: 10.1016/0195-6663(92)90195-c. [DOI] [PubMed] [Google Scholar]