

Abstract
Background
This study investigates the feasibility of performing advanced minimally invasive surgery (MIS) in a nonspecialized practice environment.
Methods
We conducted a cross-sectional survey of all community general surgeons currently practising in Ontario.
Results
Few community surgeons perform a high volume (> 10 procedures per yr) of advanced MIS. Most (70%) believe it is important to acquire additional skills in advanced MIS. The most appropriate methods for learning advanced MIS are believed to be expert mentoring (79.7%), courses (77.2%) and a colleague mentor (63.9%). A total of 57.6% of respondents have attended a course in MIS while in practice, and most have access to a reasonable variety of instrumentation. Respondents believe that 57.6% of assistants, 54.8% of nurses and 43.4% of anaesthetists are relatively inexperienced with advanced MIS. Barriers to establishing advanced MIS include limited operating room access (50%), resources or equipment (45.2%) and limited expert mentoring (43.6%). Surgeons with less than 10 years of practice found lack of trained nursing staff (7.9% v. 4.2%, p = 0.01) and experienced assistants (12% v. 6.2%, p = 0.008) to be more important barriers than did those with over 10 years of practice, respectively.
Conclusion
Most general surgeons working in Ontario are self-taught with respect to MIS skills, and few perform a high volume of advanced MIS. Only one-half of all respondents have access to skilled MIS operating room nurses, surgical assistants or anesthesiology. Despite this, general surgeons perceive the greatest barriers to introducing advanced MIS procedures to be limited access to operating rooms, resources or equipment and limited mentoring. This study has shown that the role of the surgical team in advanced MIS may be underestimated by many general surgeons. These data have important implications in training general surgeons and in incorporating additional advanced MIS procedures into the armamentarium of general surgeons.
Abstract
Contexte
Cette étude porte sur la faisabilité d'une chirurgie à effraction minimale (CEM) avancée dans un milieu de pratique non spécialisé.
Méthodes
Nous avons effectué un sondage transversal auprès de tous les chirurgiens généraux communautaires actifs en Ontario.
Résultats
Peu de chirurgiens communautaires pratiquent un volume élevé de CEM avancées (> 10 interventions par année). La plupart (70 %) croient qu'il est important d'acquérir des compétences supplémentaires en CEM avancée. On croit que les méthodes qui conviennent le mieux pour apprendre la CEM avancée sont le mentorat par des experts (79,7 %), les cours (77,2 %) et le mentorat par un collègue (63,9 %). Au total, 57,6 % des répondants ont suivi un cours en CEM au cours de leur pratique et la plupart ont accès à un éventail raisonnable d'instruments. Les répondants croient que 57,6 % des adjoints, 54,8 % des infirmières et 43,4 % des anaesthetists ont relativement peu d'expérience en CEM avancée. Les obstacles à l'implantation de la CEM avancée comprennent l'accès limité aux salles d'opération (50 %) et le manque de ressources ou de matériel (45,2 %) et de mentorat par des experts (43,6 %). Par rapport aux chirurgiens qui comptent plus de 10 ans de pratique, ceux qui pratiquent depuis moins de 10 ans signalent davantage parmi les obstacles importants le manque de personnel infirmier dûment formé (4,2 % c. 7,9 %, respectivement; p = 0,01) et d'adjoints chevronnés (6,2 % c. 12 %, respectivement; p = 0,008).
Conclusion
La plupart des chirurgiens généraux qui travaillent en Ontario sont autodidactes quant aux compétences de CEM et peu d'entre eux pratiquent un volume élevé de CEM avancées. La moitié seulement des répondants ont accès à des infirmières de salle d'opération, des adjoints en chirurgie ou des anesthésiologistes qualifiés en CEM. Les chirurgiens généraux considèrent néanmoins que les obstacles les plus importants à l'implantation d'interventions de CEM avancée sont l'accès limité aux salles d'opération et le manque de ressources ou de matériel et de mentorat. Cette étude a démontré que beaucoup de chirurgiens généraux sous-estiment peut-être le rôle de l'équipe de chirurgie en CEM avancée. Ces données ont des répercussions importantes sur la formation de chirurgiens généraux et l'ajout d'interventions supplémentaires de CEM avancée à la panoplie des chirurgiens généraux.
There is good evidence for the safety and efficacy of advanced minimally invasive surgery (MIS) for gastrointestinal disease. However, few studies have addressed the effectiveness of these procedures (i.e., reproducibility by most surgeons). Many general surgeons entering community practice have been exposed to a variety of MIS procedures during training and may wish to integrate advanced MIS techniques into their surgical practice. Others currently in practice may wish to obtain further training to offer advanced MIS procedures to their patients. It is unclear whether advanced MIS procedures developed by experts are reproducible in all hospital or practice settings where resources and facilities may differ from the institutions in which these techniques were developed. Early studies have shown the positive impact that a focused environment and trained laparoscopic team can have on the outcomes after laparoscopic cholecystectomy (LC).1
The effectiveness of advanced MIS will be determined by the feasibility of performing these technically complex procedures in a broad range of operating environments. Few studies have clearly addressed this issue in appropriate detail.2 Moreover, the potential barriers to incorporating advanced MIS into surgical practice must be clearly characterized.
This study investigates the feasibility of performing advanced MIS in a nonspecialized practice environment. The information from this study characterizes the potential barriers to introducing advanced MIS techniques into practice. Ultimately, we hope this survey will enhance our understanding of the feasibility of adopting advanced MIS by a broad range of gastrointestinal surgeons.
Methods
We conducted a descriptive, cross-sectional survey of all community general surgeons currently practising in Ontario. Based on a literature review, expert opinion and empirical data, a draft survey was developed. We explored the following issues in the survey: barriers to introducing advanced MIS in a community setting, feasibility of introducing advanced MIS procedures in all community hospitals and prerequisites to be met before a general surgeon in the community undertakes advanced MIS. We also explored the significance of each of the following parameters in successfully introducing and acquiring advanced MIS procedures in a community setting: previous MIS experience of the surgeon, expected volume of procedures, hospital resources, availability of assistants, instruction in advanced MIS and mentoring.
A focus group of 6 local experts reviewed a draft survey for validity and clarity. Consensus was reached on a final draft. A pilot assessment was performed at the 2002 Canadian Association of General Surgeons (CAGS) meeting in London, Ontario, involving 31 general surgeons attending an advanced MIS course. A mailing list was developed using a master list of Canadian surgeons obtained by MD Select. This list was limited to general surgeons practising in Ontario; the list was exported to Microsoft Excel, where it was filtered by appropriate fields to include only practising general surgeons. Three surveys were sent at 3-week intervals to all nonrespondents.
All data from returned surveys was entered into a database in spreadsheet format using Microsoft Excel and was imported into SPSS. We performed a descriptive analysis, and we used the chi-squared or Fisher's exact test for between-group comparisons, with p < 0.05 considered for statistical significance. The data were summarized to establish the factors perceived to be the most significant barriers to performing advanced MIS procedures. These inclu-ded surgeons' willingness to under-take training or mentoring and their “tolerance” of a learning curve and the instrumentation and resources available. We also established the factors that correlate with successes and failures in the performance of advanced MIS procedures in the community setting.
Results
A total of 475 surveys were mailed, with a response rate of 54.7% (260, 87% men). The majority of respondents were engaged in community surgery (203, 78%), most of whom had been in practice for over 10 years (60%), and 41.4% worked in a community with a population under 100 000.
Few community surgeons in Ontario are currently performing a high volume of advanced MIS (Fig. 1). There were no significant differences by years of practice or sex except for laparoscopic inguinal hernia repair (men: 14.2% v. women: 0%, p = 0.05). A total of 56.7% of surgeons believe they acquired their MIS skills while in surgical practice. Seventy percent believe it is important to acquire further skills in advanced MIS procedures, and 57.6% have attended a course in MIS while in practice (no difference by years of practice or sex). A total of 12.3% of respondents reported performing advanced MIS without formal instruction, and an additional 13.8% would consider this approach in their practice.

FIG. 1. Reported annual volume of minimally invasive surgery (MIS) procedures. LC = laparoscopic cholecystectomy; LA = laparoscopic appendectomy; LIHR = laparoscopic inguinal hernia repair; LVHR = laparoscopic ventral/incisional hernia repair; LF = laparoscopic fundoplication; LCS = laparoscopic colorectal surgery; LS = laparoscopic splenectomy.
According to Ontario surgeons, the most appropriate methods of instruction in advanced MIS for a surgeon in practice are expert mentoring (79.7%), courses (77.2%), a colleague mentor (63.9%), procedural videos (51.5%) and fellowship training (21.4%). Most respondents would accept increased operating time and personal stress during the learning curve for advanced MIS (96.1% and 84.2%, respectively) while some (16.7%) would accept increased procedural complications.
Most surgeons seem to have access to a reasonable range of instrumentation: a 30º laparoscope (90.1%), a spare laparoscope (96%), an endovascular stapler (86.6%), atraumatic forceps (84.8%), long graspers or scissors (85.6%), 2 monitors (57.4%) and video recording capabilities (57.3%).
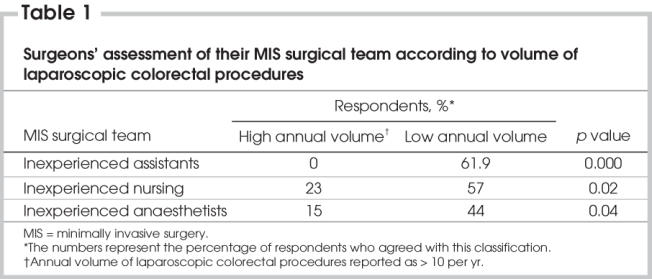
When asked to assess their surgical team regarding MIS skills, many surgeons responded that they are working with inexperienced assistants (57.6%), inexperienced nurses (54.8%) and inexperienced anaesthetists (43.4%). However, surgeons who reported performing a high annual volume of laparoscopic colorectal surgery (over 10 procedures per year) believe they have an experienced team of nurses, assistants and anaesthetists (Table 1).
Table 1
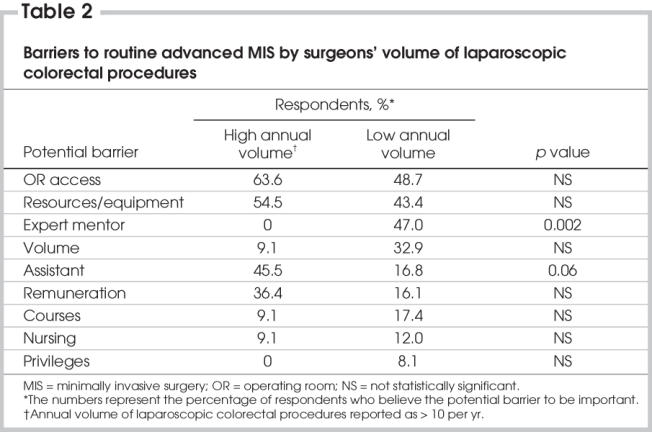
The most important barriers to incorporating advanced MIS procedures into surgical practice are shown in Figure 2. Surgeons with less than 10 years in practice differed from their more senior counterparts by ranking untrained nursing staff (7.9% v. 4.2%, p = 0.01) and inexperienced assistants (12% v. 6.2%, p = 0.008) as more important barriers. When surgeons were stratified according to their annual volume of laparoscopic colorectal procedures, those with a low annual volume believed more strongly that they require a mentor than their high-volume counterparts; high-volume surgeons think an inexperienced assistant is a significant barrier to the routine performance of advanced MIS procedures (Table 2).
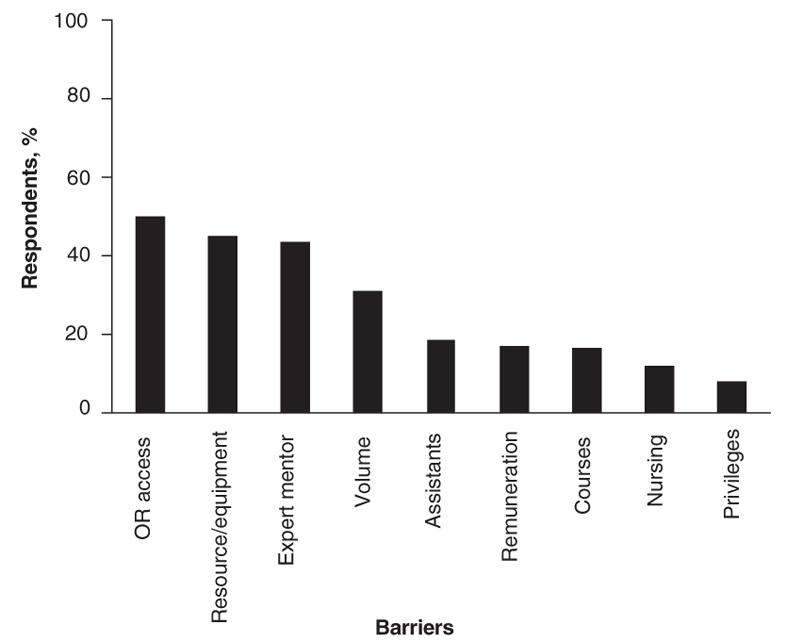
FIG. 2. The barriers to introducing advanced minimally invasive surgery into a community practice. OR = operating room.
Table 2
Discussion
The effectiveness of advanced MIS for gastrointestinal disease will be determined by the feasibility of completing these procedures in a broad range of practice settings. The technical complexity of the MIS operating suite has been recognized, and structured approaches have been suggested to promote efficiency.3,4 The positive impact that a trained laparoscopic team can have on the outcomes of laparoscopic cholecystectomy (LC) has been described.1 See and colleagues demonstrated that urologists are more likely to encounter problems in laparoscopic surgery after an instructional course if they have a variable surgical assistant.5 However, the overall impact of the surgical team on the success of incorporating advanced MIS into surgical practice has been poorly described.
Many outstanding questions need to be addressed to understand the feasibility of completing advanced MIS in varied hospital or practice settings. In addition, more research is required to understand what may constitute a barrier for surgeons who want to include advanced MIS techniques into their surgical practice. Empirically, we believe the determinants for successful introduction of advanced MIS techniques may be included in the following conceptual categories: the current training of the surgeon and their motivation to undergo training in advanced MIS techniques, the human resources available to the surgeon (nursing, assistants, anaesthetists) and the availability and selection of instrumentation and resources (including access to operating rooms).
In this study, we found that most general surgeons currently practising in Ontario are self-taught. Few perform a high volume of advanced MIS, but most plan to introduce advanced MIS procedures into their practice. Although several studies have been published on learning curves for individual MIS procedures, none clearly address the feasibility of introducing advanced MIS procedures into the community.6–8 Marusch and colleagues9 emphasized surgical experience as a requirement to performing advanced MIS procedures without describing how this experience should be acquired or whether there were other limiting factors to routinely performing advanced MIS. Voitk and others7,10 presented learning curves for selected MIS procedures in a community hospital with a group of experienced surgeons. There was limited discussion of the key factors that may affect the characteristics of a learning curve. Simons and colleagues11 addressed learning curves for advanced MIS procedures in previously trained MIS surgeons. Lishman12 outlined his impressions of the requirements for introducing MIS surgery into surgical practice in a discussion that was largely anecdotal and that presented little supporting data. The most appropriate method for introducing new techniques into surgical practice and credentialing surgeons in these techniques has yet to be established. A short course may introduce an advanced MIS procedure and allow a surgeon and his or her team to determine whether it is feasible to adopt the procedure into practice (i.e., human resources, training requirements, administrative support, adequate case volume).13 This course should be followed by a comprehensive approach to teaching that is rational and fulfills the needs of surgeon trainees. This will include determining the needs of surgical teams and providing appropriate education for the nurses, assistants and surgeons. A period of observation and planning at the mentor's institution should be followed by individualized training in MIS skills and a graded approach to training by the mentor for the relevant procedures. There are now training systems available (i.e., Fundamentals in Laparoscopic Surgery) and sophisticated training devices (Virtual Reality Procedural Training: Minimally Invasive Surgery Trainer, Surgical Education Platform) that may facilitate training and evaluation for surgeons in practice.14,15 Centralized mentoring (mentor's institution) and, finally, mentoring at the surgeon trainee's institution will complete the training program and should allow mentors to complete an appropriate evaluation and credentialing statement.
In this study, respondents indicated that lack of a mentor was an important barrier to overcome in order to introduce advanced MIS into surgical practice (Fig. 2). Currently in Canada, there is no clear mechanism to facilitate access to expert mentors. National experts in MIS must accept the challenge to coordinate and facilitate a new training paradigm that is effective and feasible for surgeons in practice who wish to adopt advanced MIS procedures.
We have shown that recently trained surgeons may be more likely to introduce advanced MIS into practice. This may be a surrogate marker for an increase in advanced MIS occurring at academic training centres. Although this does not give insight into the clinical outcomes achieved by recent graduates, it demonstrates that, as the volume of advanced MIS increases at academic centres where residency training programs are centralized, the competence of graduates in advanced MIS may also increase.
Surgical practice as an advanced MIS surgeon differs dramatically from practice as an open surgeon. There is a distinct role change in the operating room because the surgeon has a greater reliance on his or her surgical team (Table 1, Table 2). Each member of the MIS team plays a more important role than in open surgery, largely due to the increased technical complexity of advanced MIS procedures.3,4,16 As a result, greater consideration must be given to training the entire surgical team in preparation for routine advanced MIS surgery for gastrointestinal disease.17 There is some evidence that specialized operating room teams lead to increased efficiency and improved job satisfaction, enhancing the recruitment and retention of nurses.18
Our data indicate that the feasibility of incorporating advanced MIS into practice may be determined largely by the surgical team. Inexperience of the surgical team may be the most significant barrier to introducing advanced MIS into practice (Table 1). More importantly, we have shown that the impact of a trained surgical team may not be clearly recognized by surgeons, especially those inexperienced in routine advanced MIS (Table 2). Surgeons seem to emphasize the significance of instrumentation and operating room access in the performance of routine advanced MIS. Despite this, most surgeons report that they have access to a reasonable selection of laparoscopic instrumentation. Further, the impression of restricted operating room access may be an artificial barrier, linked to concerns of reduced throughput during training of the MIS surgical team. The performance of routine advanced MIS by surgeons may require a shift in the traditional surgical paradigm: more technically complex procedures are completed with a marginal increase in operating time to achieve an important benefit for patients (less time in hospital, reduced wound complications and reduced morbidity overall).
Training of an MIS surgical team must include training for all team members in conjunction with the procedural training of the surgeon. If this challenge is met, it will be feasible for advanced MIS to be successfully performed on a wide scale by a variety of surgeons. If this challenge is not met, we predict that only select teams will complete routine advanced MIS in the surgical management of gastrointestinal disease through specialization or regionalization.
Acknowledgments
We thank the Surgical Outcomes Research Committee for assisting with data entry.
Presented at the 2004 Annual Meeting of Society of American Gastrointestinal and Endoscopic Surgeons, Denver, Colorado.
Competing interests: Dr. Birch has received speaker fees from Bard and consulting fees from Johnson & Johnson/Ethicon Endo-Surgery.
Accepted for publication Apr. 19, 2005
Correspondence to: Dr. Daniel W. Birch, Royal Alexandra Hospital, 10240 Kingsway, Edmonton AB T5H 3V9; fax 780 735-4771; dbirch@ualberta.ca
References
- 1.Kenyon TA, Lenker MP, Bax TW, et al. Cost and benefit of the trained laparoscopic team. A comparative study of a designated nursing team vs a nontrained team. Surg Endosc 1997;11:812-4. [DOI] [PubMed]
- 2.Chan SW, Hensman C, Waxman BP, et al. Technical developments and a team approach leads to an improved outcome: lessons learnt implementing laparoscopic splenectomy. ANZ J Surg 2002;72:523-7. [DOI] [PubMed]
- 3.Herron DM, Gagner M, Kenyon TL, et al. The minimally invasive surgical suite enters the 21st century. A discussion of critical design elements. Surg Endosc 2001;15: 415-22. [DOI] [PubMed]
- 4.Kenyon TA, Urbach DR, Speer JB, et al. Dedicated minimally invasive surgery suites increase operating room efficiency. Surg Endosc 2001;15:1140-3. [DOI] [PubMed]
- 5.See WA, Cooper CS, Fisher RJ. Predictors of laparoscopic complications after formal training in laparoscopic surgery. JAMA 1993;270:2689-92. [PubMed]
- 6.Occelli B, Narducci F, Lanvin D, et al. Learning curves for transperitoneal laparoscopic and extraperitoneal endoscopic paraaortic lymphadenectomy. J Am Assoc Gynecol Laparosc 2000;7:51-3. [DOI] [PubMed]
- 7.Voitk AJ. The learning curve in laparoscopic inguinal hernia repair for the community general surgeon. Can J Surg 1998;41:446-50. [PMC free article] [PubMed]
- 8.Perino A, Cucinella G, Venezia R, et al. Total laparoscopic hysterectomy versus total abdominal hysterectomy: an assessment of the learning curve in a prospective randomized study. Hum Reprod 1999;14:2996-9. [DOI] [PubMed]
- 9.Marusch F, Gastinger I, Schneider C, et al. Experience as a factor influencing the indications for laparoscopic colorectal surgery and the results. Surg Endosc 2001; 15:116-20. [DOI] [PubMed]
- 10.Voitk A, Joffe J. Alvarez, Rosenthal G. Factors contributing to laparoscopic failure during the learning curve for laparoscopic Nissen fundoplication in a community hospital. J Laparoendosc Adv Surg Tech A 1999;9:243-8. [DOI] [PubMed]
- 11.Simons AJ, Athone GJ, Ortega AE, et al. Laparoscopic assisted colectomy learning curve. Dis Colon Rectum 1995;38:600-3. [DOI] [PubMed]
- 12.Lishman IV. Laparoscopic surgery in peripheral hospitals. Aust Fam Physician 1994;23:383-93. [PubMed]
- 13.Birch DW, Sample C, Gupta R. The impact of a comprehensive course in advanced minimal access surgery on surgeon practice. Can J Surg 2007;50:9-12. [PMC free article] [PubMed]
- 14.Chaudhry A, Sutton C, Wood J, et al. Learning rate for laparoscopic surgical skills on MIST VR, a virtual reality simulator: quality of human-computer interface. Ann R Coll Surg Engl 1999;81:281-6. [PMC free article] [PubMed]
- 15.Peters JH, Fried GM, Swanstrom LL, et al. Development and validation of a comprehensive program of education and assessment of the basic fundamentals of laparoscopic surgery. Surgery 2004;135:21-7. [DOI] [PubMed]
- 16.Seus JD, Wood T. Reaping maximum benefits from minimally invasive surgery. J Healthc Mater Manage 1994;12:20-4. [PubMed]
- 17.Winer WK. The role of the operating room staff in operative laparoscopy. J Am Assoc Gynecol Laparosc 1993;1:86-8. [DOI] [PubMed]
- 18.Sprengel AD. Snell WE, Boissoneau R. Specialty surgical teams. Results of a study. AORN J 1993;58:1170-80. [DOI] [PubMed]