

Pulmonary aspergillosis occurs in parenchymal cavities or ectatic airways. Aspergillus is a ubiquitous dimorphic fungus. It rarely affects healthy people with an intact immune response, but those with preexisting structural lung disease, atopy, occupational exposure or impaired immunity are susceptible.1 Aspergillosis can remain asymptomatic or present with hemoptysis, which can be life-threatening. In this report, we describe a patient who presented with an aspergilloma arising in a cavitating adenocarcinoma of the right lung.
Case presentation
A 54-year-old man, a smoker who was otherwise healthy, presented with history of cough productive of brownish sputum for 4 weeks. There was no history of chest pain, shortness of breath, fever or chills, and he denied any history of hemoptysis or weight loss. On physical examination, he appeared healthy with normal findings on chest, cardiovascular, abdominal and neurologic examinations. Chest radiography revealed a mass in the right upper lung zone, and on CT, there was a cavitary lesion in the posterior segment of the right upper lung lobe, with a central homogeneous rounded density typical of an aspergilloma (Fig. 1). His antifungal serum antibodies were nonreactive.
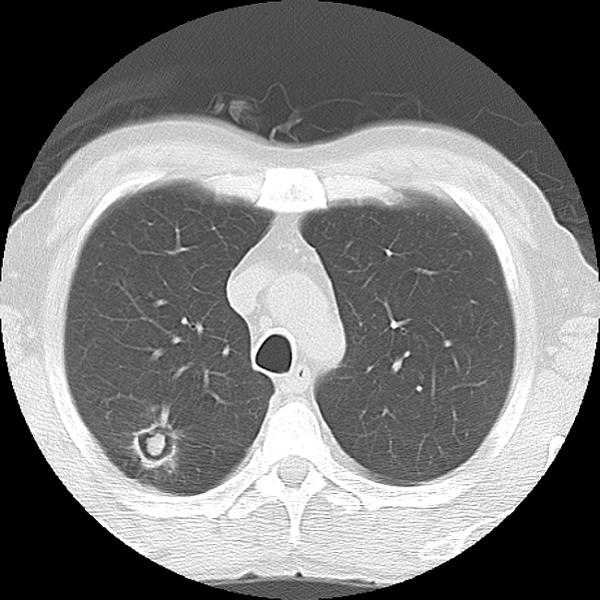
FIG. 1. CT scan at the level of the aortic arch shows evidence of a cavitated lesion in the posterior segment of the right upper lobe. The lesion contained about 1 cm of central soft tissue nidus, compatible with an aspergilloma.
Preoperative pulmonary function tests gave normal results. The patient underwent flexible bronchoscopy followed by right posterolateral thoracotomy. No abnormalities were found on bronchoscopic examination. On thoracotomy, a soft mass was palpable in the posterior segment of the right upper lobe, compatible with CT findings. Wedge excision of the lesion was followed by frozen section examination. This revealed the presence of an unsuspected poorly differentiated adenocarcinoma with central necrosis associated with fungal growth (Fig. 2). Right upper lobectomy and mediastinal lymph-node dissection were performed. The patient had an uncomplicated postoperative recovery. The final histologic finding confirmed the diagnosis of a T1N0 poorly differentiated adenocarcinoma.

FIG. 2. Histologic appearance from wedge resection of the upper right lung lobe demonstrates dichotomously branching hyphae, compatible with Aspergillus associated with adenocarcinoma (Gomori methenamine silver stain; original magnification 400×).
Discussion
Four distinctive patterns of Aspergillus-related lung diseases are recognized, as follows: saprophytic colonization, pulmonary aspergilloma, hypersensitivity-induced aspergillosis and invasive pulmonary aspergillosis.2 When a pre-existing cavity becomes colonized by a fungus, typically Aspergillus, a mycetoma (fungus ball or aspergilloma) forms, usually in the upper lung fields. It consists of branched, septated hyphae and blood cells.3 It is typically caused by Aspergillus fumigatus, although other species may be associated with its formation. The diagnosis is usually established radiologically by demonstrating the characteristic appearance of the fungus ball. Conditions associated with aspergilloma formation include tuberculosis, sarcoidosis, histoplasmosis, lung abscess, bronchiectasis, bullae, pulmonary infarcts, cystic fibrosis, HIV infection and cavitated squamous cell lung cancer.1
From 1959 to 1992, the most common preexisting condition was tuberculosis. Since then, the prevalence of pulmonary aspergilloma has declined.3 In one study, the prevalence of Aspergillus growth in patients with bronchogenic carcinoma was reported as being 14.2%,4 but only a few cases of combined aspergilloma and lung cancer have been reported in the literature.5 Most cases lacked one or both of the features of postinflammatory intracavitary aspergilloma: a loose fungus ball and antifungal serum antibodies. In some cases, the presence of lung cancer with aspergilloma was difficult to detect radiologically.5
In this report, the aspergilloma occurred in a healthy man who had no known preexisting risk factors and had an unsuspected cavitary adenocarcinoma. We suggest that when aspergilloma is found in healthy persons with no risk factors, lung cancer must be ruled out. We also believe that this is another indication for surgical treatment of a fungus ball.
Competing interests: None declared.
Accepted for publication July 19, 2006
Correspondence to: Dr. Harry Henteleff, Queen Elizabeth II Health Sciences Centre, 1278 Tower Rd., 7 south-010, Halifax NS B3H 2Y9; fax 902 473-5851; harry.henteleff@dal.ca
References
- 1.Bardana EJ. Pulmonary aspergillosis. In: Al-Doory Y, Wagner GE, editors. Aspergillosis. Springfield (IL): Charles C Thomas; 1985. p. 43-78.
- 2.Al-Alawi A, Rayan CF, Flint JD, et al. Aspergillus-related lung disease. Can Respir J 2005;12:377-87. [DOI] [PubMed]
- 3.Babatasi G, Massetti M, Chapelier A, et al. Surgical treatment of pulmonary aspergilloma: current outcome. J Thorac Cardiovasc Surg 2000;119:906-12. [DOI] [PubMed]
- 4.Malik A, Shahid M, Bhagava R. Prevalence of aspergillosis in bronchogenic carcinoma. Indian J Pathol Microbiol 2003;46:507-10. [PubMed]
- 5.Tomioka H, Iwasaki H, Okumura N, et al. Undiagnosed lung cancer complicated by intracavitary aspergillosis [abstract]. Nihon Kokyuki Gakkai Zasshi 1999;37:78-82. [PubMed]