

Abstract
Context:
Long-term effects of ankle bracing on lower extremity kinematics and kinetics are unknown. Ankle motion restriction may negatively affect the body's ability to attenuate ground reaction forces (GRFs).
Objective:
To evaluate the immediate and long-term effects of ankle bracing on lower extremity kinematics and GRFs during a jump landing.
Design:
Experimental mixed model (2 [group] × 2 [brace] × 2 [time]) with repeated measures.
Setting:
Sports medicine research laboratory.
Patients or Other Participants:
A total of 37 healthy subjects were assigned randomly to either the intervention (n = 11 men, 8 women; age = 19.63 ± 0.72 years, height = 176.05 ± 10.58 cm, mass = 71.50 ± 13.15 kg) or control group (n = 11 men, 7 women; age = 19.94 ± 1.44 years, height = 179.15 ± 8.81 cm, mass = 74.10 ± 10.33 kg).
Intervention(s):
The intervention group wore braces on both ankles and the control group did not wear braces during all recreational activities for an 8-week period.
Main Outcome Measure(s):
Initial ground contact angles, maximum joint angles, time to reach maximum joint angles, and joint range of motion for sagittal-plane knee and ankle motion were measured during a jump-landing task. Peak vertical GRF and the time to reach peak vertical GRF were assessed also.
Results:
While participants were wearing the brace, ankle plantar flexion at initial ground contact (brace = 35° ± 13°, no brace = 38° ± 15°, P = .024), maximum dorsiflexion (brace = 21° ± 7°, no brace = 22° ± 6°, P = .04), dorsiflexion range of motion (brace = 56° ± 14°, no brace = 59° ± 16°, P = .001), and knee flexion range of motion (brace = 79° ± 16°, no brace = 82° ± 16°, P = .036) decreased, whereas knee flexion at initial ground contact increased (brace = 12° ± 9°, no brace = 9° ± 9°, P = .0001). Wearing the brace for 8 weeks did not affect any of the outcome measures, and the brace caused no changes in vertical GRFs (P > .05).
Conclusions:
Although ankle sagittal-plane motion was restricted with the brace, knee flexion upon landing increased and peak vertical GRF did not change. The type of lace-up brace used in this study appeared to restrict ankle motion without increasing knee extension or vertical GRFs and without changing kinematics or kinetics over time.
Keywords: prophylactic; braces, external ankle supports; landings; injury prevention
Key Points.
Prolonged lace-up ankle brace use did not cause any changes in lower extremity kinematics or vertical ground reaction forces.
Ankle sagittal-plane motion was restricted and knee flexion at initial contact increased during a jump landing every time an ankle brace was worn.
Future researchers should evaluate if these findings are present with other types of external ankle supports and during other functional tasks.
Lateral ankle sprains are one of the most common injuries in sports, resulting in high cost1 and much time lost from normal activity.2,3 Verhagen et al3 observed that lateral ankle sprains accounted for 40% of all volleyball injuries, whereas Messina et al4 reported that 30% of all injuries in high school basketball players involved the ankle joint. In addition, the initial ankle-sprain episode has been shown to be a strong predisposing factor for recurrent ankle sprains, as well as chronic ankle joint instability and degeneration.3,5 Therefore, preventing the initial ankle sprain is essential.
One of the most common methods for preventing lateral ankle sprains is the use of external support, such as ankle taping or bracing. Prophylactic ankle bracing can decrease the incidence of lateral ankle sprains.5,6 The primary mechanism responsible for preventing ankle sprains is the ability of braces to restrict ankle inversion and eversion movements before landing from a jump.7 By controlling these motions, the ankle remains in a neutral position in the frontal plane during landing, thereby limiting stresses placed on the ankle ligaments.7
External ankle supports are designed to restrict frontal-plane motion in order to protect the ankle from injury; however, some methods of support also limit ankle sagittal-plane motion.8 During a jump landing, joint motions begin distally and progress proximally in order to dissipate energy.9,10 When normal motion or muscular function around the ankle is restricted, the entire lower extremity may be affected, and changes in normal movement patterns may occur. Because ankle braces restrict normal ankle motion, specifically ankle dorsiflexion and plantar flexion, they may have a detrimental effect on the lower extremity's ability to attenuate vertical ground reaction forces (VGRFs) during landing.11,12 During a jump landing, VGRFs as high as 6.2 times body weight have been reported.13 Therefore, a reduced ability to effectively dissipate force when landing from a jump may increase the risk of other lower extremity injuries. If ankle braces affect the ankle's ability to reduce ground reaction forces (GRFs), the effects also might be observed proximally at the knee. Although GRFs are known to stimulate bone repair and remodeling, excessive GRFs may be associated with an increased risk of injury to structures such as subchondral bone, cartilage, and soft tissue.9,14–17 The body's primary methods of attenuating these forces are through extensor and flexor moments about the hip, knee, and ankle joints.14 A number of investigators credited eccentrically controlled ankle dorsiflexion9,14,16–19 and knee flexion movements13,14,16–19 with reducing GRFs during landing.
Research11,12,20 investigating the effect of ankle bracing during dynamic activities on lower extremity kinematics and kinetics has been limited. These authors all examined the immediate effects of ankle bracing; however, athletes often wear ankle braces for extended periods of time and may experience long-term effects. Clinicians and athletes have expressed concern that wearing prophylactic ankle braces for extended periods of time might weaken the surrounding musculature or might alter landing mechanics. One set of authors21 did find an increased reflexive response in the peroneus longus muscle after volunteers wore ankle braces for 8 weeks. To our knowledge, no groups have examined the long-term effects of prophylactic ankle bracing on lower extremity kinematics and VGRFs. Therefore, our purpose was to investigate the effects of immediate and prolonged prophylactic ankle bracing during regular physical activity on ankle and knee sagittal-plane motions and VGRFs during a jump-landing task.
Methods
Design
We used a randomized controlled design to compare the effects of ankle bracing on sagittal-plane ankle and knee kinematics and VGRFs. Three independent variables assessed differences among 10 dependent variables. The independent variables included group (brace or control: between-subjects variable), test (pretest or posttest: within-subjects variable), and brace condition (no brace or brace: within-subjects variable). The 10 dependent variables were joint angles at initial contact (°), maximum joint angles (°), time to maximum joint angles (milliseconds), and joint displacement (°) for knee and ankle sagittal-plane motion, as well as peak VGRF (percentage of body weight) and time to reach peak VGRF (milliseconds).
Participants
Forty-two recreational volleyball and basketball athletes (22 men, 20 women; age range = 18 to 22 years) volunteered to participate in this study. We assigned participants to either the intervention or control group through random selection without replacement by sex and sport. Random selection took place upon arrival at the initial testing session, and a coin flip determined group assignment.
Exclusion criteria included any recent (3 days of physical activity lost within the past month) lower extremity injury, any current symptoms of lower extremity injury, any previous lower extremity surgery, or the use of external ankle support on a regular basis before testing. Participants were not permitted to use any type of ankle bracing or taping for 3 months before testing in order to be eligible for this study. All volunteers regularly took part in activities that involved repetitive landings, such as basketball or volleyball, for approximately 1 to 2 hours per day, 3 to 4 times per week.19
Inclusion criteria included having functionally stable ankles with no history of a severe ankle sprain as well as no subjective reports of instability, which was defined as frequent “rolling” or “giving way.” An ankle sprain was considered severe if the injury required a non–weight-bearing period of 3 days and restricted physical activity for at least 2 weeks.
Experimental Procedures
Participants reported to the research laboratory for 2 testing sessions. Upon arrival at the initial testing session, all volunteers completed an informed consent form that described the testing protocol, which was approved by the institutional review board. During both testing sessions, each participant wore a T-shirt, shorts, and his or her own basketball or volleyball shoes. Participants wore their own shoes versus standard shoes to control for the fact that those in the intervention group wore their own shoes with the ankle braces during the study.
Ankle and knee kinematic and VGRF data were collected by an electromagnetic motion analysis system (Flock of Birds; Ascension Technology Corp, Burlington, VT) controlled by Motion Monitor data acquisition computer software (version 7; Innovative Sports Training, Inc, Chicago, IL) used for collection of kinematic data from a nonconductive force plate (model 4060-NC, Bertec Corp, Columbus, OH) during a standardized jump-landing task (Figure 1). Participants were required to jump forward from a 30-cm–high box to the force plate located on the ground.22 The distance between the front of the box and the front of the force plate was standardized for each participant to half of measured body height. Participants were instructed to land with the dominant foot in the center of the force plate and the nondominant foot on the carpeted area beside the force plate. As soon as the participant landed, he or she was instructed to jump for maximal height. The dominant leg was defined as the leg used to kick a soccer ball for a maximal distance with the greatest amount of force.
Figure 1. The jump-landing task.
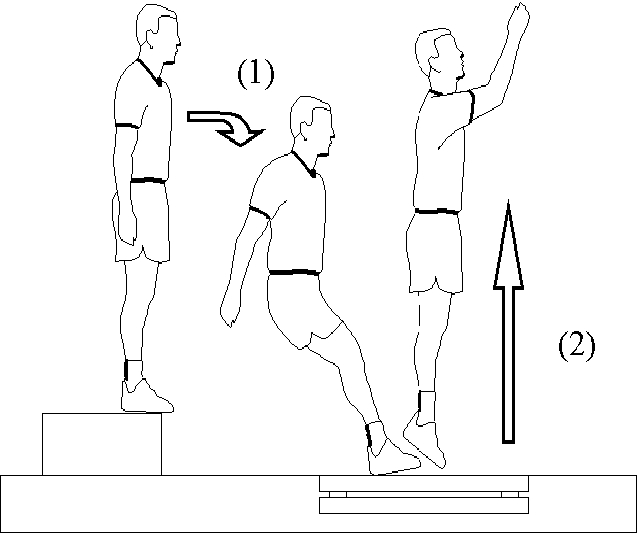
Instructions were then given to each participant regarding the general nature of the jump-landing task (jump forward from the box, land on the force plate, and jump up for maximal vertical height), and the researcher demonstrated the maneuver only once to minimize coaching effects. The participants were instructed to perform the jump-landing task in their preferred natural manner and not to be influenced by the demonstration of the investigator. Before any trials were recorded, each participant had 3 to 5 trials to practice the jump-landing task. The practice trials concluded when the participant correctly performed the jump-landing task and appeared comfortable with the task.
All participants were tested in 2 conditions during both testing sessions, with and without an ankle brace (Figure 2). The order of conditions was counterbalanced. For each condition, 5 acceptable trials were performed, with a 30-second rest period between trials to minimize fatigue effects. Trials were excluded if the participant did not land properly with 1 foot completely on the force plate, jumped vertically from the box instead of forward, or did not perform the jump-landing task correctly.
Figure 2. The intervention group wore the ASO Ankle Brace (Medical Specialties, Inc, Charlotte, NC) bilaterally during all physical activity through the intervention period. The brace also was worn bilaterally by all participants during both testing sessions.
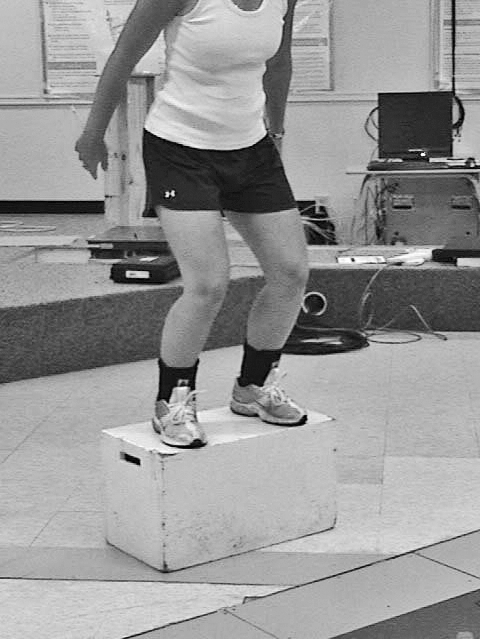
The intervention group was required to wear the ASO Ankle Brace (Medical Specialties Inc, Charlotte, NC) on both ankles during all recreational activity for 8 weeks after the first testing session. We chose the intervention period of 8 weeks based on previous research examining the effects of long-term ankle bracing on peroneal longus muscle latency over an 8-week intervention period.23 A group investigating the effects of ankle disk training on functional instability used a comparable intervention period.24
Compliance was maintained by weekly random checks at the participants' practices and self-report data. Participants completed an activity diary in which they recorded the week, number of activity days during the week, duration of activities, whether or not they used the ankle brace, and any lower extremity injury that may have occurred. A participant in either group was excluded from the study if he or she did not complete at least 2 days of activity per week. Participants in the intervention group were excluded from the study if they did not meet a compliance criterion of wearing the ankle braces 80% of the time (approximately 20/24 practices). Participants in both groups reported for testing before and after the 8-week period of ankle bracing. The second testing session (posttest) occurred within 1 week of concluding the intervention period and consisted of the same testing procedures as in the initial testing session (pretest).
The ASO Ankle Brace is a lace-up ankle brace with nylon straps that lock around the calcaneus, similar to heel locks in ankle taping. The brace is made of a nylon material with an elastic cuff closure. Each participant was fitted for the brace according to the manufacturer's guidelines based on shoe size. Participants in the intervention group were instructed on proper application of the ankle brace. Before each testing session, the brace was applied to each participant by the same certified athletic trainer according to the manufacturer's guidelines.
Data Collection, Reduction, and Processing
The electromagnetic motion analysis system controlled by Motion Monitor data acquisition computer software was used for collection of kinematic data. For the 3-dimensional electromagnetic motion analysis system, the manufacturer reported a linear accuracy of 0.75 cm and angular accuracy of 0.5°. The main component of the motion analysis system is a standard-range direct-current transmitter with 3 orthogonal coils that generate an electromagnetic field. A standard-range transmitter produced electromagnetic changes in the field, which were recorded by electromagnetic sensors sampling at 144 Hz. These recordings were then transferred to a recording computer through hard wiring. Kinetic data from the force plate were synchronized, sampled at a rate of 1440 Hz, and converted into GRF data through the data acquisition computer software. The software processed the raw sensor data, and a Butterworth fourth-order, low-pass digital filter (zero phase lag) smoothed the data at a mean estimated optimum cutoff frequency of 14.5 Hz.25 The VGRFs were normalized for body weight (N), and the data were filtered with a fourth-order, low-pass Butterworth filter set at 100 Hz.
Electromagnetic sensors were attached to the dorsum of the foot (over the midshaft of the second and third metatarsals), anterior shaft of the tibia, lateral aspect of the femur, and base of the sacrum using double-sided tape and elastic wrap to prevent motion artifact. After unlacing the shoe, the tongue was pulled forward and fastened to the top of the shoe with double-sided tape to expose the dorsum of the foot to allow sensor placement. The shoe was then relaced to ensure proper fit. This procedure was performed to allow space for the sensor on the foot without contacting the ASO Ankle Brace or affecting the support provided by the shoe. The participants did not wear socks in order to permit the sensors to be firmly attached directly to the skin. The sensors on the tibia and femur were placed over areas with minimal muscle and soft tissue mass to minimize the effects of muscle contraction and skin movement on the kinematics data.
After application of the electromagnetic sensors, the participant's dominant leg was digitized. The participants stood in a neutral and relaxed position while we palpated bony landmarks and digitized them with a movable sensor attached to a wooden stylus. The digitized bony landmarks included the most prominent portions of the medial and lateral femoral condyles, medial and lateral malleoli, and the distal tip of the second phalanx. The Leardini et al26 method was used to digitize the center of the hip joint. The joint centers of the knee and ankle were defined as centroids between the medial and lateral femoral condyles and the medial and lateral malleoli, respectively. The femoral segment was defined by the centroid between the medial and lateral femoral condyles and the estimated hip joint center. The tibial segment was defined by the centroids of the knee and the ankle malleoli. The centroid between the medial and lateral malleoli and the point at the distal tip of the second phalange defined the foot segment. After the electromagnetic motion analysis system was set up, we recorded a static trial with the participant in a neutral standing position. Kinematic and kinetic data were reduced, and raw data were converted to the aligned anatomical coordinate axes. To describe joint motions in clinically relevant terms, joint motions were determined through a joint-coordinate system.27
We determined ankle plantar flexion and knee flexion angles at initial ground contact, maximum ankle and knee joint angles during the stance phase, time to reach maximum joint angles, and ankle and knee range of motion between initial ground contact and maximum joint angles. Initial ground contact was defined as the time the VGRF exceeded 5 N during the jump landing, whereas toe-off was defined as the moment when the VGRF dropped below 5 N. Stance phase was defined as the period between initial ground contact and toe-off. Kinetic data included the peak VGRF recorded during the stance phase, as well as the time to peak VGRF. The average for the 5 trials was used for each of the kinematic and kinetic variables during the jump-landing task. All processing was performed with customized software in MATLAB (The Mathworks, Natick, MA).
Statistical Analyses
We used a mixed-model, repeated-measures design with 1 between-subjects factor (control or intervention group) and 2 within-subjects factors (brace or no-brace condition, pretest or posttest). With a mixed-model multivariate analysis of variance (MANOVA), we compared differences between groups, testing times, and testing conditions for several of the dependent variables (knee and ankle angles at initial ground contact, maximum knee joint and ankle joint angles, knee and ankle displacement, and time to reach maximum knee joint and ankle joint angles). A second, separate mixed-model MANOVA was used for the kinetic dependent variables (peak VGRF and time to reach peak VGRF). Separate univariate analyses of variance were performed, if necessary, based on the results of the multivariate analysis of variance, and a 2-tailed independent t test compared participant demographics between groups. All data were analyzed with SPSS (version 14; SPSS Inc, Chicago, IL) with the a priori α level set at .05.
Results
Of the original 42 recruited participants randomly assigned to either the intervention (n = 20) or control (n = 22) group, 1 intervention group volunteer and 4 control group volunteers were lost to follow-up. Participants were excluded from the study either for failing to meet the physical activity requirements of the study (2 control participants) or due to an injury (1 intervention participant: skin irritation; 2 control participants: anterior cruciate ligament sprain, tibial stress fracture) sustained during physical activity outside of testing. No intervention group participants were excluded from the study for failing to meet the compliance criteria. Thus, the data from 19 intervention group subjects (11 men, 8 women; age = 19.63 ± 0.72 years, height = 176.05 ± 10.58 cm, mass = 71.50 ± 13.15 kg) and 18 control group participants (11 men, 7 women; age = 19.94 ± 1.44 years, height = 179.15 ± 8.81 cm, mass = 74.10 ± 10.33 kg) were used for data analyses. No differences in age, height, or mass existed between groups (P > .05).
Kinematics
Means and SDs for joint angles at initial ground contact, peak joint angles, joint angle displacement, and time to reach peak joint angle are presented for the ankle and knee joints in Tables 1 and 2, respectively. No group-by-time-by-brace (F6,29 = 1.20, Wilks Λ = .77, P = .34, ηp2 = .23), group-by-time (F6,29 = 1.17, Λ = .77, P = .35, ηp2 = .23) , group-by-brace (F6,29 = 2.09, Λ = .70, P = .09, ηp2 = .30), or brace-by-time (F6,29 = 1.07, Λ = .79, P = .41, ηp2 = .21) interactions were observed with the MANOVA. A main effect for the brace condition was noted (F6,29 = 5.27, Λ = .48, P = .001, ηp2 = .52), but no other main effects were significant (time: F6,29 = 1.53, Λ = .72, P = .20, ηp2 = .28; group: F6,29 = .45, Λ = .92, P = .84, ηp2 = .08).
Table 1.
Ankle Kinematicsa

Table 2.
Knee Kinematicsa

With post hoc univariate analyses of variance, we compared differences between these variables based on the main effect for brace condition demonstrated by the MANOVA. We observed a difference in knee flexion angle at initial ground contact between the brace and no-brace conditions (brace condition = 12° ± 9°, no-brace condition = 9° ± 9°; F1,34 = 18.36, P = .0001, ηp2 = .35; Figure 3). Overall, participants demonstrated greater knee flexion at initial ground contact during the brace condition compared with the no-brace condition. Also, a decrease was seen in knee flexion joint displacement in the brace condition compared with the no-brace condition (brace condition = 79° ± 16°, no-brace condition = 82° ± 16°; F1,34 = 4.75, P = .04, ηp2 = .12). No differences existed between brace conditions for knee flexion maximum angle (F1,34 = .03, P = .86, ηp2 = .001) or time to reach maximum knee flexion (F1,34 = 3.27, P = .08, ηp2 = .09).
Figure 3. Knee flexion at initial ground contact during brace and no-brace conditions. aThe no-brace condition resulted in less knee flexion at initial ground contact (condition main effect).

We also observed a difference in ankle plantar flexion at initial contact (brace condition = 35° ± 13°, no-brace condition = 38° ± 15°; F1,34 = 5.59, P = .02, ηp2 = .14), maximum ankle dorsiflexion (brace condition = 21° ± 7°, no-brace condition = 22° ± 6°; F1,34 = 4.54, P = .04, ηp2 = .12), and ankle dorsiflexion range of motion (brace condition = 56° ± 14°, no-brace condition = 59° ± 16°; F1,34 = 13.15, P = .001, ηp2 = .28) between the brace conditions (Figure 4). No differences existed between brace conditions for the time to reach maximum ankle dorsiflexion (F1,34 = 1.19, P = .66, ηp2 = .006). Overall, individuals demonstrated reduced ankle sagittal-plane motion while wearing the ankle brace in comparison with the no-brace condition.
Figure 4. Sagittal-plane ankle-joint motion during brace and no-brace conditions. aThe brace condition resulted in less plantar flexion at initial contact, less maximum dorsiflexion, and less total joint displacement (condition main effect).

The only significant ankle and knee kinematic findings involved main effects for the ankle brace condition. Thus, ankle and knee kinematics were not affected after wearing an ankle brace for 8 weeks. The changes observed occurred with all participants every time an ankle brace was worn during both testing sessions.
Kinetics
Means and SDs for the peak VGRF and the time to reach the peak VGRF during the jump-landing task are presented in Table 3. No group-by-time-by-brace (F2,33 = .165, Λ = .99, P = .85, ηp2 = .01), group-by-time (F2,33 = .09, Λ = .99, P = .92, ηp2 = .01) , group-by-brace (F2,33 = .79, Λ = .95, P = .46, ηp2 = .05), or brace-by-time (F2,33 = .33, Λ = .98, P = .72, ηp2 = .02) interactions or main effects (group: F2,33 = .39, Λ = .98, P = .68, ηp2 = .02; time: F2,33 = .41, Λ = .98, P = .67, ηp2 = .02; brace: F2,33 = 1.14, Λ = .94, P = .33, ηp2 = .06) were observed with the MANOVA. Therefore, the peak VGRF and the rate at which this force occurred were similar between groups in both the brace and no-brace conditions and during both testing sessions.
Table 3.
Kinetic Dataa

Discussion
Our most important finding was that prophylactic ankle bracing effectively limited sagittal-plane ankle motion, but VGRF was not affected, perhaps due to increases in knee flexion angle at initial contact when performing a jump-landing task. Although immediate changes occurred due to the ankle brace, no chronic alterations in knee and ankle kinematics or VGRFs were noted after wearing a prophylactic ankle brace for 8 weeks. The changes observed occurred with all participants each time an ankle brace was worn during both testing sessions.
Ankle brace use for an extended period of time, such as during an entire sport season, has been hypothesized to cause detrimental effects to the ankle musculature, ankle range of motion, and landing mechanics. Findings of previous authors21,23 examining the effect of long-term ankle brace use on peroneous longus muscle activity have not supported this notion. Cordova et al23 found no change in peroneus longus muscle latency after an 8-week period of ankle bracing, whereas Cordova and Ingersoll21 demonstrated increases in peroneus longus muscle reflex amplitude after a similar intervention. Our results agree with these previous results, because sagittal-plane knee and ankle kinematics and VGRFs did not change after an intervention period of wearing an ankle brace for 8 weeks. These results add to the current literature supporting prophylactic ankle brace use during a season.
Prophylactic ankle braces are used as a preventive measure to reduce ankle injuries during athletics5,6 and commonly are worn throughout an entire season. However, most authors of previous studies on ankle braces have only examined the immediate effects of wearing an ankle brace. In these short-term studies, researchers were not able to evaluate any breakdown in the mechanical properties of an ankle brace or if a person became accustomed to wearing the ankle brace and developed compensatory movement patterns. To our knowledge, we are the first to investigate the effects of prolonged ankle brace use on lower extremity kinematics and kinetics. The main effect for ankle brace condition on knee and ankle kinematics indicates that reductions in ankle dorsiflexion range of motion and increases in knee flexion angle at initial contact were only present when the participants were wearing the ankle brace. The lack of a brace-by-time interaction indicates that wearing the ankle brace for 8 weeks during physical activity did not affect these variables. Thus, any change that may have occurred in the ankle brace's mechanical stiffness over time did not seem to affect the ankle joint restrictions or landing patterns.
In a meta-analysis, Cordova et al8 showed that ankle braces can effectively restrict ankle motions. The authors of most of the studies in this meta-analysis investigated passive ankle motions and not the effects of ankle braces during functional tasks. Our findings agree with and extend the previous research investigating the influence of ankle braces on ankle motion, because we observed decreased ankle plantar flexion upon landing and reduced sagittal-plane motion throughout the jump-landing task when participants wore the ankle brace.8,11 Although ankle braces are designed to prevent excessive frontal-plane motion or to maintain the ankle in a neutral position before landing,7,28 our findings demonstrate that ankle braces effectively limited sagittal-plane ankle motion as well. The mechanism of injury for lateral ankle sprains is described as a combination of inversion, plantar flexion, and internal rotation.29 Therefore, the ankle brace's ability to limit sagittal-plane ankle motion may protect the ankle from these potentially hazardous positions, thus reducing the risk of lateral ankle sprains when wearing the ankle brace.
Restricting sagittal-plane ankle movement when wearing an ankle brace may help to prevent lateral ankle sprains, but ankle dorsiflexion motion is one of the primary ways in which GRFs are absorbed and dissipated when landing from a jump.14 By limiting ankle dorsiflexion during a jump landing, the body's center of mass may undergo less downward displacement when contacting the ground and may result in greater GRFs acting on the body. Due to this relationship, we originally hypothesized that restricted ankle dorsiflexion motion would impair the body's ability to absorb energy when landing from a jump and would result in greater GRFs acting on the body. Increased GRFs due to ankle braces may increase the risk for other lower extremity injuries and might provide a rationale for not using ankle braces. Contrary to our original hypothesis, no changes were noted in peak VGRF while participants wore the ankle brace in this study. Thus, ankle braces did not appear to affect VGRF magnitude; however, it is not clear if lower extremity joint loading was affected by use of the ankle braces, because we did not measure joint reaction forces or moments during landing.
Our finding that VGRF was not affected by ankle bracing is in agreement with the findings of Hopper et al, 20 who investigated the effects of ankle bracing on VGRFs assessed during a single-leg landing. Riemann et al12 also reported no change in VGRF with the use of an ankle brace; however, the time to maximum force decreased during a brace condition, contradicting our findings. The disagreement between our results and this study may be due to the use of a different type of ankle brace and task performed.
Our most surprising result was the finding of increased knee flexion angle at initial contact when wearing the ankle brace. We believe that greater knee flexion when wearing the ankle brace offset the restrictions in ankle motion and allowed the VGRF to remain consistent between the brace and no-brace conditions. In addition to the ankle, knee flexion plays an important role in the body's ability to absorb energy during landing, because downward displacement of the body's center of mass is increased with greater knee flexion; according to the work-energy relationship, this should reduce the force acting on the body. Several authors14,17,18 have demonstrated an inverse relationship between knee flexion and VGRF. In our study, the knee appeared to compensate with more knee flexion at initial contact because ankle motion was reduced due to the ankle brace, thereby potentially keeping the magnitude and rate of VGRF relatively constant. Although knee flexion displacement (peak flexion to initial contact knee flexion) was reduced when the participants wore the ankle brace, peak knee flexion angle was unchanged. Therefore, the decrease in knee flexion displacement was most likely due to increased knee flexion upon landing and not different knee flexion amounts during the stance phase.
Benefits to wearing an ankle brace in terms of influencing anterior tibial shear force may be associated with our findings of increased knee flexion upon landing when wearing an ankle brace. Researchers have shown that knee flexion angle influences the magnitude of anterior tibial shear force acting at the knee. Decreased knee flexion angle results in a larger patellar tendon–tibial shaft angle, which results in greater anterior shear force during quadriceps muscle contraction.30 Also, the ability of the hamstrings muscles to offset anterior tibial shear forces is minimized when the knee is in a less-flexed position, thus compromising the dynamic stability provided by the hamstrings. Recent research by Yu et al31 indicates an inverse relationship between knee flexion angle and anterior tibial shear force magnitude, because individuals landing with less knee flexion experienced greater anterior tibial shear force. Considering that VGRFs were not affected with the wearing of an ankle brace, it is reasonable to suggest that increased knee flexion angle when wearing an ankle brace may result in less anterior tibial shear force at the knee. Future research is necessary to investigate the effect of ankle bracing on anterior tibial shear force during jump landings.
Limitations and Future Research
A limitation of this study is that only a single type of brace was employed for all testing and interventions. Thus, the results are limited to the ASO Ankle Brace that uses a lace-up design with a locking strap configuration. We chose this brace because it is a common prophylactic ankle brace and is considered to be comfortable, with no rigid supports. These factors may increase compliance with wearing an ankle brace. In addition, Cordova et al8 reported differences between this type of ankle brace and other semirigid braces in ankle sagittal-plane motion restriction. Therefore, we hypothesized that any changes in sagittal-plane motion would more likely be seen using a lace-up with strap configuration ankle brace than a semirigid brace.
Future investigation is needed to learn if the changes we observed also occur in other functional tasks, such as cutting maneuvers. In addition, more information about the effects of ankle bracing on muscle activity and muscle strength would be beneficial.
Clinical Significance
In conclusion, our results indicate that VGRFs were not increased by the immediate application of an ankle brace or after 8 weeks of wearing an ankle brace. Thus, potential loading consequences should not prohibit clinicians from using ankle braces as a preventive measure for ankle injury. Furthermore, our results suggest that prophylactic ankle bracing may have benefits in reducing forces at the knee joint by increasing knee flexion angle during landing. Only a small amount of knee flexion occurs at initial contact (8° to 15°) during a jump-landing task; therefore, a 2° or 3° change is a large percentage (13% to 25%) of the total motion. The altered knee and ankle motions only changed by a few degrees due to the ankle brace, but whether this degree of movement is clinically significant is unknown and should be further investigated.
Acknowledgments
This study was funded by the National Athletic Trainers' Association Research & Education Foundation (Osternig Master's Grant), Dallas, TX. We thank Medical Specialties, Inc, for donating the ASO Ankle Braces used in this study.
Footnotes
Lindsay J. DiStefano, MA, LAT, ATC, and Darin A. Padua, PhD, ATC, contributed to conception and design; acquisition and analysis and interpretation of the data; and drafting, critical revision, and final approval of the article. Cathleen N. Brown, PhD, LAT, ATC, contributed to conception and design; acquisition and analysis and interpretation of the data; and critical revision and final approval of the article. Kevin M. Guskiewicz, PhD, ATC, FACSM, contributed to conception and design; analysis and interpretation of the data; and critical revision and final approval of the article.
References
- 1.Soboroff S.H, Pappius E.M, Komaroff A.L. Benefits, risks, and costs of alternative approaches to the evaluation and treatment of severe ankle sprain. Clin Orthop Relat Res. 1984;183:160–168. [PubMed] [Google Scholar]
- 2.McKay G.D, Goldie P.A, Payne W.R, Oakes B.W, Watson L.F. A prospective study of injuries in basketball: a total profile and comparison by gender and standard of competition. J Sci Med Sport. 2001;4(2):196–211. doi: 10.1016/s1440-2440(01)80030-x. [DOI] [PubMed] [Google Scholar]
- 3.Verhagen E.A, Van der Beek A.J, Bouter L.M, Bahr R.M, Van Mechelen W. A one-season prospective cohort study of volleyball injuries. Br J Sports Med. 2004;38(4):477–481. doi: 10.1136/bjsm.2003.005785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Messina D.F, Farney W.C, DeLee J.C. The incidence of injury in Texas high school basketball: a prospective study among male and female athletes. Am J Sports Med. 1999;27(3):294–299. doi: 10.1177/03635465990270030401. [DOI] [PubMed] [Google Scholar]
- 5.Surve I, Schwellnus M.P, Noakes T, Lombard C. A fivefold reduction in the incidence of recurrent ankle sprains in soccer players using the Sport-Stirrup orthosis. Am J Sports Med. 1994;22(5):601–606. doi: 10.1177/036354659402200506. [DOI] [PubMed] [Google Scholar]
- 6.Rovere G.D, Clarke T.J, Yates C.S, Burley K. Retrospective comparison of taping and ankle stabilizers in preventing ankle injuries. Am J Sports Med. 1988;16(3):228–233. doi: 10.1177/036354658801600305. [DOI] [PubMed] [Google Scholar]
- 7.Eils E, Rosenbaum D. The main function of ankle braces is to control the joint position before landing. Foot Ankle Int. 2003;24(3):263–268. doi: 10.1177/107110070302400312. [DOI] [PubMed] [Google Scholar]
- 8.Cordova M.L, Ingersoll C.D, LeBlanc M.J. Influence of ankle support on joint range of motion before and after exercise: a meta-analysis. J Orthop Sports Phys Ther. 2000;30(4):170–182. doi: 10.2519/jospt.2000.30.4.170. [DOI] [PubMed] [Google Scholar]
- 9.Gross T.S, Nelson R.C. The shock attenuation role of the ankle during landing from a vertical jump. Med Sci Sports Exerc. 1988;20(5):506–514. [PubMed] [Google Scholar]
- 10.Zhang S.N, Bates B.T, Dufek J.S. Contributions of lower extremity joints to energy dissipation during landings. Med Sci Sports Exerc. 2000;32(4):812–819. doi: 10.1097/00005768-200004000-00014. [DOI] [PubMed] [Google Scholar]
- 11.McCaw S.T, Cerullo J.F. Prophylactic ankle stabilizers affect ankle joint kinematics during drop landings. Med Sci Sports Exerc. 1999;31(5):702–707. doi: 10.1097/00005768-199905000-00013. [DOI] [PubMed] [Google Scholar]
- 12.Riemann B.L, Schmitz R.J, Gale M, McCaw S.T. Effect of ankle taping and bracing on vertical ground reaction forces during drop landings before and after treadmill jogging. J Orthop Sports Phys Ther. 2002;32(12):628–635. doi: 10.2519/jospt.2002.32.12.628. [DOI] [PubMed] [Google Scholar]
- 13.Salci Y, Kentel B.B, Heycan C, Akin S, Korkusuz F. Comparison of landing maneuvers between male and female college volleyball players. Clin Biomech (Bristol, Avon) 2004;19(6):622–628. doi: 10.1016/j.clinbiomech.2004.03.006. [DOI] [PubMed] [Google Scholar]
- 14.Devita P, Skelly W.A. Effect of landing stiffness on joint kinetics and energetics in the lower extremity. Med Sci Sports Exerc. 1992;24(1):108–115. [PubMed] [Google Scholar]
- 15.Dufek J.S, Bates B.T. Biomechanical factors associated with injury during landing in jump sports. Sports Med. 1991;12(5):326–337. doi: 10.2165/00007256-199112050-00005. [DOI] [PubMed] [Google Scholar]
- 16.Dufek J.S, Zhang S. Landing models for volleyball players: a longitudinal evaluation. J Sports Med Phys Fitness. 1996;36(1):35–42. [PubMed] [Google Scholar]
- 17.Mizrahi J, Susak Z. Analysis of parameters affecting impact force attenuation during landing in human vertical free fall. Eng Med. 1982;11(3):141–147. doi: 10.1243/emed_jour_1982_011_039_02. [DOI] [PubMed] [Google Scholar]
- 18.Dufek J.S, Bates B.T. The evaluation and prediction of impact forces during landings. Med Sci Sports Exerc. 1990;22(3):370–377. [PubMed] [Google Scholar]
- 19.Prapavessis H, McNair P.J. Effects of instruction in jumping technique and experience jumping on ground reaction forces. J Orthop Sports Phys Ther. 1999;29(6):352–356. doi: 10.2519/jospt.1999.29.6.352. [DOI] [PubMed] [Google Scholar]
- 20.Hopper D.M, McNair P, Elliott B.C. Landing in netball: effects of taping and bracing the ankle. Br J Sports Med. 1999;33(6):409–413. doi: 10.1136/bjsm.33.6.409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cordova M.L, Ingersoll C.D. Peroneus longus stretch reflex amplitude increases after ankle brace application. Br J Sports Med. 2003;37(3):258–262. doi: 10.1136/bjsm.37.3.258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Myer G.D, Ford K.R, Palumbo J.P, Hewett T.E. Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. J Strength Cond Res. 2005;19(1):51–60. doi: 10.1519/13643.1. [DOI] [PubMed] [Google Scholar]
- 23.Cordova M.L, Cardona C.V, Ingersoll C.D, Sandrey M.A. Long-term ankle brace use does not affect peroneus longus muscle latency during sudden inversion in normal subjects. J Athl Train. 2000;35(4):407–411. [PMC free article] [PubMed] [Google Scholar]
- 24.Matsusaka N, Yokoyama S, Tsurusaki T, Inokuchi S, Okita M. Effect of ankle disk training combined with tactile stimulation to the leg and foot on functional instability of the ankle. Am J Sports Med. 2001;29(1):25–30. doi: 10.1177/03635465010290010901. [DOI] [PubMed] [Google Scholar]
- 25.Yu B, Gabriel D, Noble L, An K. Estimate of the optimum cutoff frequency for the Butterworth low-pass digital filter. J Appl Biomech. 1999;15(3):318–329. [Google Scholar]
- 26.Leardini A, Cappozzo A, Catani F, et al. Validation of a functional method for the estimation of hip joint centre location. J Biomech. 1999;32(1):99–103. doi: 10.1016/s0021-9290(98)00148-1. [DOI] [PubMed] [Google Scholar]
- 27.Grood E.S, Suntay W.J. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng. 1983;105(2):136–144. doi: 10.1115/1.3138397. [DOI] [PubMed] [Google Scholar]
- 28.Thonnard J.L, Bragard D, Willems P.A, Plaghki L. Stability of the braced ankle: a biomechanical investigation. Am J Sports Med. 1996;24(3):356–361. doi: 10.1177/036354659602400318. [DOI] [PubMed] [Google Scholar]
- 29.Garrick J.G. The frequency of injury, mechanism of injury, and epidemiology of ankle sprains. Am J Sports Med. 1977;5(6):241–242. doi: 10.1177/036354657700500606. [DOI] [PubMed] [Google Scholar]
- 30.Nunley R.M, Wright D.W, Renner J.B, Yu B, Garrett W.E., Jr Gender comparison of patellar tendon tibial shaft angle with weight-bearing. Res Sports Med. 2003;11(3):173–185. [Google Scholar]
- 31.Yu B, Lin C.F, Garrett W.E. Lower extremity biomechanics during the landing of a stop-jump task. Clin Biomech (Bristol, Avon) 2006;21(3):297–305. doi: 10.1016/j.clinbiomech.2005.11.003. [DOI] [PubMed] [Google Scholar]