

Abstract
The current study tested the independence of dispositional optimism and pessimism from negative and positive affectivity in the prediction of older adults’ well-being, concurrently and five years later, using structural equation modeling. As hypothesized, in a community sample, both optimism/pessimism and affectivity were correlated cross-sectionally and prospectively with outcomes representing general health and well-being (self-rated health, somatic depression and life satisfaction). However, with both sets of predictors in the model, affectivity eliminated the relationships of optimism/pessimism with the outcomes. Our proposed explanation for these findings, derived from the theoretical self-regulation model, also explains the seemingly contradictory previous findings of an independent contribution of dispositional optimism in patient samples coping with specific stressors.
Keywords: optimism, pessimism, negative affectivity, positive affectivity
INTRODUCTION
The relationship between personality and individuals’ health and well-being has been extensively documented (Smith & Spiro, 2002). The present research focused on dispositional optimism, or “generalized outcome expectancies”, as defined by Scheier and Carver (Scheier & Carver, 1985). This construct was derived from their theory of the self-regulation of behavior (Carver & Scheier, 1998; Scheier & Carver, 1988). Scheier and Carver (1985) have also developed an instrument to assess dispositional optimism, the Life Orientation Test (LOT) and its revised version (LOT-R, Scheier, Carver & Bridges, 1994). Extensive research has provided evidence of the physical and psychological health benefits of optimism (see meta-analysis by Andersson, 1996; reviews by Scheier & Carver, 1987; Scheier, Carver, & Bridges, 2001). However, some researchers have questioned the construct validity of dispositional optimism and argued that it overlaps with neuroticism.
The independent effect of dispositional optimism has first been questioned by Smith, Pope, Rhodewalt, and Poulton (1989), who argued that pessimism is simply another facet of neuroticism. Neuroticism, or negative affectivity, is defined as consisting of chronic negative emotions and has typically been operationalized using scales of neuroticism or of trait anxiety/negative affect. Smith et al. (1989) showed that the correlations of the LOT with health and coping measures were mostly eliminated when neuroticism was controlled for and concluded that the LOT is virtually indistinguishable from neuroticism.
Scheier et al. (1994) replied to this challenge with evidence showing that the associations between optimism and both depression and coping remained significant after controlling for neuroticism, trait anxiety, self-mastery, and self-esteem. Many later studies have also tested the independent associations of optimism and negative affectivity with various outcomes, yielding inconsistent evidence.
Many studies of psychological adjustment supported the independence of dispositional optimism in both young and older samples (e.g., Aspinwall & Taylor, 1992; Chang, Maydeu-Olivares, & D’Zurilla, 1997; Mroczek, Spiro, Aldwin, Ozer, & Bosse, 1993) while others provided partial support for both approaches (Bromberger & Matthews, 1996; Cheng & Hamid, 1997). Regarding physical health, many studies provided evidence supporting the approach that optimism is indistinguishable from negative affectivity (e.g., Chang, 1998a; Ebert, Tucker, & Roth, 2002; Scheier et al., 1994; Smith et al., 1989) or provided partial support for both approaches (Chang, 1998b; Cheng & Hamid, 1997; Robbins, Spence, & Clark, 1991). In sum, neither approach has consistently received clear-cut support. Many of the studies provided partial support for both approaches, showing the independence of optimism regarding some but not all outcomes or samples tested.
Both the Smith et al. (1989) study and Scheier et al.’s (1994) response were based on data from undergraduates. Much of the later research pertaining to this issue has also been carried out with student or community samples of generally healthy young adults. Some studies did include a wider range of ages, but very few studies focused on older adults. This is surprising in a research area that deals with future expectancies, since the future could have a different meaning for older people. Therefore, the objective of the current study is to examine the independence of optimism from affectivity using data from a longitudinal study of a relatively large community sample of older adults, which includes their self-ratings of optimism and affectivity as well as measures of physical and psychological well-being with a follow-up after five years.
Conceptual Issues
How can we explain findings, which sometimes show an independent effect for optimism and sometimes show that negative affectivity provides a more parsimonious explanation for this effect? In order to suggest an explanation and formulate a testable hypothesis, we turn to the theoretical model. Carver and Scheier’s model delineates the process in which we progress towards our goals. Optimism comes into play if and when we experience obstacles on the way: We interrupt our efforts to assess outcome expectancies and decide whether to continue pursuing that goal or forfeit it. Then, “people who are optimistic by nature are more likely to emerge from expectancy assessment with a greater sense of confidence than people who are pessimistic” (Carver & Scheier, 1998, p. 177).
Optimists’ confidence can “yield a mix of feelings that is relatively positive…” whereas the pessimists’ “doubt should yield a greater tendency toward negative feelings…” (Scheier et al., 2001, p. 191). Such relationships of optimism with affect do not contradict Smith et al.’s (1989) assertion that lack of optimism, or pessimism, is merely another facet of neuroticism. However, Carver and Scheier also argue that this sense of confidence leads people to renew their efforts to attain their goal whereas a sense of doubt can lead them to give up their goal. Renewed efforts to attain a goal increase the chances of attaining it, which explains why optimism has been linked with more favorable outcomes.
This self-regulation process suggests that optimism’s unique role should be apparent among people coping with a specific stressor and regarding outcomes that are specifically related to stress and coping. For example, faced with the stress of a serious health threat or a difficult medical procedure, people are likely to be more tuned to specific recovery goals but could also doubt their ability to achieve these goals, and therefore optimism would be more likely to play a role. This corresponds with findings from studies of older adults, which often involved patients coping with specific stressors, and were therefore more likely to find unique effects for optimism (e.g., Scheier et al., 1999). Data from a sub-sample of the current study sample also supported this part of our explanation: In a small sub-sample of arthritis patients, optimism and pessimism had unique associations with use of pain coping strategies, even after controlling for negative (and positive) affectivity (Benyamini, 2004).
However, the theoretical model also provides the rationale for the other part of our explanation, which argues that in a community sample of older adults, regarding measures of general psychological and physical well-being, there is no reason to expect that optimism will have a unique effect beyond that of affectivity. Thus, we hypothesize that among elderly community residents: (1) Optimism will be related to measures of general psychological and physical well-being (self-ratings of health, depression, and life satisfaction) cross-sectionally and longitudinally; but, (2) this effect will not be significant after controlling for affectivity.
Methodological Issues
Many of the studies that tested the independence of optimism from affectivity were cross-sectional. Studies that employed a longitudinal design typically included a follow-up of up to a year (for an exception, see Bromberger & Matthews, 1996, who had a 3-year follow-up and reported that both optimism and trait anxiety predicted future depressive symptoms for women who experienced a stressful ongoing problem). Furthermore, most tests of the independence of optimism in predicting psychological and physical health outcomes were based on partial correlations, often derived from multiple regression analyses. Only a handful of studies employed Structural Equation Modeling (SEM), which allows for consideration of substantive relations between hypothetical constructs apart from measurement issues (Aspinwall & Taylor, 1992; Ebert et al., 2002; Robinson-Whelen, Kim, MacCallum, & Kiecolt-Glaser, 1997).
Therefore, we used data from community-residing elderly people, which included baseline measures of the LOT and of positive and negative affectivity as well as measures of three important aspects of elderly people’s well-being: Their self-rating of health, symptoms of somatic depression, and life satisfaction. Follow-up data was collected five years later. The data were analyzed with SEM. Thus, this study enabled us to investigate the independence of optimism from affectivity among elderly community residents, within a longitudinal study design, using a relatively large sample and appropriate statistical methodology.
In testing the study hypothesis, we distinguished between optimism and pessimism (and between positive and negative affectivity). Specifically for an older population, the decision to treat these constructs separately is justified by the lower correlations between optimism and pessimism in elderly samples (e.g., Mroczek et al., 1993; Plomin et al., 1992) and evidence that older adults report higher rates of both optimism and pessimism compared with younger ones (Isaacowitz, 2005). An additional reason for this decision was the abundant support for a two-factor model of affect (Kunzmann, Little, & Smith, 2000) and our wish to keep the models equivalent for the two types of dispositions.
METHODS
Participants
Participants were residents of a retirement community who participated in the Rutgers Aging and Health Study (RAH). Their mean age was 72.19 (±7.14) at baseline and 61.1% were women. The baseline (T1) RAH sample included 851 participants. The present study used data from 525 participants who were also interviewed five years later (T2). Subject dropout due to withdrawal, severe illness, relocation, or death, amounted to about 8% a year, which is reasonable for an elderly sample of self-respondents. Details about recruitment procedures were published elsewhere (Benyamini, Leventhal, & Leventhal, 1999).
Procedure
The study included face-to-face interviews, mostly (95%) conducted in respondents’ homes, the remainder in the community clubhouse. Interviewers read each question aloud and recorded the participant’s response into a computer.
Measures
Optimism/pessimism
We used a 6-item version (3 optimism and 3 pessimism items) adapted from the LOT1 (Scheier & Carver, 1985). Responses were made on a 5-point scale from 1=“strongly disagree” to 5=“strongly agree”. Internal reliability coefficients for all study measures are reported in Table 1.
Table 1.
Descriptive Statistics, Internal Reliabilities, and Intercorrelations Among Study Measures Within Each Data Wave (N=525)
| Meam | SD | Alpha | 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 Optimism a | T1 | 3.61 | 0.70 | .76 | ||||||
| T2 | 3.63 | 0.63 | .74 | - | ||||||
| 2 Pessimism a | T1 | 2.19 | 0.58 | .66 | −.45 | |||||
| T2 | 2.24* | 0.56 | .64 | −.41 | - | |||||
| 3 Happiness | T1 | 1.71 | 0.68 | .88 | .51 | −.44 | ||||
| T2 | 1.87*** | 0.68 | .90 | .48 | −.34 | - | ||||
| 4 Anxiety | T1 | 3.81 | 0.67 | .89 | −.42 | .35 | −.34 | |||
| T2 | 3.47*** | 0.74 | .88 | −.30 | .26 | −.48 | - | |||
| 5 Self-rated health | T1 | 3.70 | 0.86 | .86 | .27 | −.24 | .38 | −.30 | ||
| T2 | 3.37*** | 0.86 | .88 | .31 | −.22 | .47 | −.30 | - | ||
| 6 Somatic depression | T1 | 1.32 | 0.38 | .66 | −.30 | 25 | −.33 | .45 | −.38 | |
| T2 | 1.45*** | 0.41 | .65 | −.30 | .28 | −.47 | .50 | −.45 | - | |
| 7 Life satisfaction | T1 | 3.54 | 0.66 | .78 | .40 | −.38 | .54 | −.31 | .32 | −.32 |
| T2 | 3.42*** | 0.65 | .78 | .43 | −.31 | .62 | −.45 | .48 | −.46 |
Note: Correlations over .17 are significant at p<.001, for all other correlations p<.05; for means, asterisks denote level of significance of difference between T1 and T2,
p<.05
p<.01
p<.001.
Negative and Positive Affectivity were operationalized using scales of trait anxiety and happiness. These traits do not include all aspects of neuroticism, or negative affectivity, as defined in previous research. However, in practice, many of the studies cited above also operationalized neuroticism using measures of trait anxiety (including Smith et al., 1989). These traits were assessed using 5-item scales each of anxiety and happiness based on the Profile of Mood States (POMS, McNair, Lorr, & Droppleman, 1971) and selected according to the highest loadings in confirmatory factor analyses of data from an elderly sample (Usala & Hertzog, 1989). The item format was: “How nervous/worried/tense/on edge/uneasy are you usually?” and “How happy/pleased/content/enthusiastic/cheerful are you usually?” (response scale from 1=“not at all” to 5=“very much”). Since “usually” was often unclear, the interviewers emphasized that the participant is requested to refer to a long range of time and not to the recent days, thus distinguishing between this measure and current mood.
Self-rated health was assessed using two items: “In general, would you say your health is...?”, and “Compared to other people your own age, would you say your general health is…excellent (5), very good, good, fair, or poor (1)”. The validity of self-rated health as a predictor of future health outcomes has been extensively documented (Idler & Benyamini, 1997).
Somatic depression symptoms were assessed using 5 items from the Center for Epidemiological Studies Depression Scale (CES-D, Radloff, 1977) that refer to somatic depression (e.g., sleep and appetite problems, difficulties in “getting going”). Participants were asked how often they have felt this way during the past two weeks, from 1=“rarely or none of the time” to 4=“most or all of the time”.
Satisfaction with life was assessed using the following four items: (1) I am very satisfied with my life; (2) These are the best years of my life; (3) My life could be happier than it is now; and, (4) The quality of my life is poor (the latter two were reverse coded). The items were rated on a 5-point scale from 1=“strongly disagree” to 5=“strongly agree”.
Analytical Approach
SEM was done with EQS Version 6 (Bentler, 2002). The analyses were performed using variance-covariance matrices. About 3% of the observations had missing values in one or two indicators. In the analyses reported, we used pairwise deletion of missing values. Two alternative methods of dealing with missing values were also employed: listwise deletion and estimation using the expectation-maximization method. All three methods yielded very similar results. The variables in the datasets used in the analyses were multivariately non-normally distributed, with normalized estimates of multivariate kurtosis ranging from 10.24 to 42.90. To overcome this violation of the maximum-likelihood estimation assumptions, we employed this estimation method with robust standard errors, together with the Satorra-Bentler rescaled chi-square statistic (Satorra & Bentler, 1994) that compensates for non-normality of variables. Following the recommendations of Hu and Bentler (1999), we report, in addition to the chi-square, two approximate fit indices, the Non-Normed Fit Index (NNFI, also known as TLI) and the Comparative Fit Index (CFI), and two approximate misfit indices, the Root Mean-Square Error of Approximation (RMSEA) and the Standardized Root Mean-Square Residual (SRMR). In spite of the recent critique of such “subjective” fit measures (e.g., Barrett, 2007), we believe that they are useful heuristics (cf. Mulaik, 2007) for evaluating SEModels. Models that (a) have a large N; (b) fail the chi-square test; but (c) exhibit NNFI and CFI close to unity combined with RMSEA and SRMR close to zero, “pass” some minimal statistical requirements and therefore, their parameter values deserve substantial interpretation.
RESULTS
Descriptive statistics and intercorrelations among study measures appear in Table 1. Correlations among optimism, pessimism, happiness, and anxiety ranged between .26 and .51. All zero-order correlations between optimism, pessimism, negative and positive affectivity on the one hand, and self-rated health, somatic depression and life satisfaction on the other hand, were significant at both times.
For the SEM, optimism was indicated by the three positively worded items of the brief LOT-based scale, pessimism by the three negatively worded ones, and self-rated health by two items. For anxiety, happiness, somatic depression, and life satisfaction, we created three indicators each, by averaging some of the items. Since each variable was measured twice, altogether the analyzed data matrix had 40 observed variables. In order to reflect the longitudinal nature of our data, measurement errors of the same indicators at two times were allowed to correlate freely and factor loadings were constrained to be equal at the two times. The measurement model with these specifications performed poorly on the exact fit test, with χ2 (660, N = 525) = 1066.14, p < .001. Nevertheless, as its approximate fit was fair (NNFI = .944, CFI = .952, RMSEA = .034, SRMR = .068), we moved on to testing structural models.
First, we tested separate models, one for optimism and pessimism as predictors of the outcome measures, and the other for happiness and anxiety as predictors. In the first model (Figure 1), both optimism and pessimism were statistically significantly correlated with all three outcomes at T1. At T2, optimism was correlated with self-rated health and life satisfaction, but not with somatic depression, while pessimism was correlated with somatic depression and life satisfaction, but not with self-rated health. In the second model (Figure 2), all paths from anxiety and happiness to the three outcomes were significant at T1, and all but one path (from anxiety to self-rated health) were significant at T2.
Figure 1.
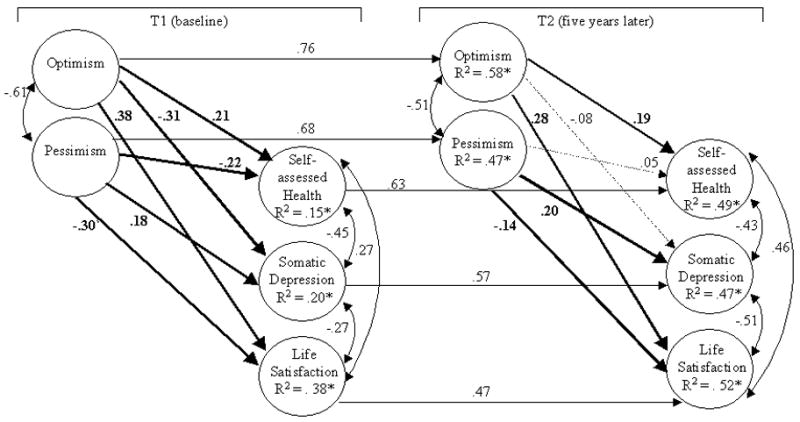
Structural equation model of the associations between optimism and three outcome variables (standardized parameter estimates), χ2 (320, N = 525)=453.79, p<.001, NNFI=.964, CFI=.970, RMSEA=.028, SRMR=.046. In this and the next figures: Solid lines represent statistically significant paths (p<.05). Broken lines represent paths that are not statistically significant. Measured indicators, their errors, and correlations between measurement errors of the same indicators at two times are not shown. All R-squared values are statistically significant at p<.01.
Figure 2.
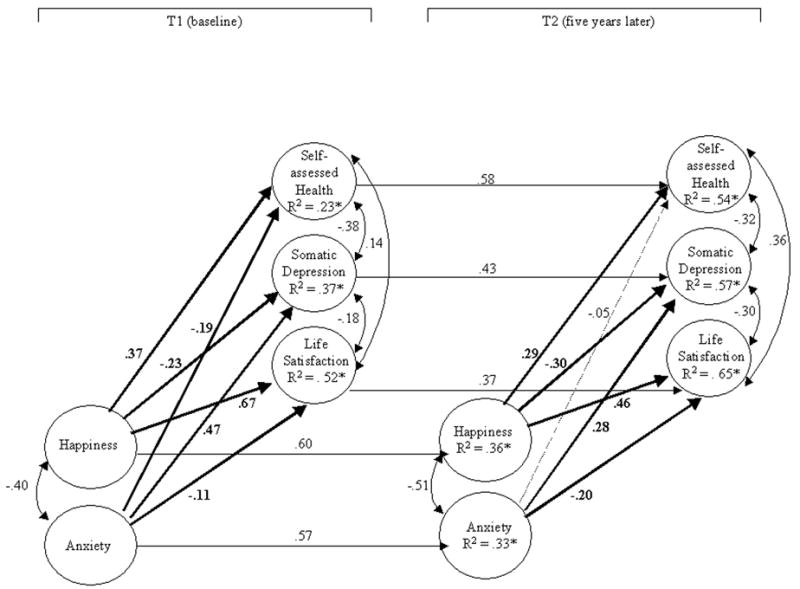
Structural equation model of the associations between affect and three outcome variables (standardized parameter estimates), χ2 (320, N=525)= 444.67, p<.001, NNFI=.976, CFI=.980, RMSEA=.027, SRMR=.055.
Next, we combined both sets of predictors in a single model in order to assess their unique effects. The model, shown in Figure 3, failed the exact fit test, with χ2 (684, N = 525) = 893.30, p < .001. However, its measures of approximate fit were quite high (see figure). In light of this, we considered it appropriate to interpret specific model parameters pertaining to our hypothesis.
Figure 3.
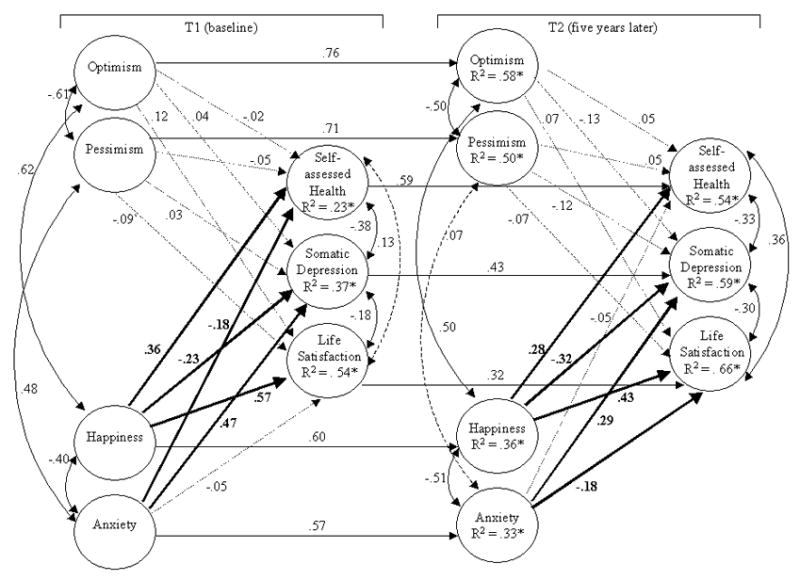
Structural equation model of the associations between optimism and affect and three outcome variables (standardized parameter estimates), χ2 (684, N=525)=893.30, p<.001, NNFI=.971, CFI=.975, RMSEA=.024, SRMR=.049.
The stability of happiness and anxiety over the 5-year period did not differ significantly from that of optimism and pessimism. At both measurement times, most paths from anxiety and depression to the dependent variables were significant (with the exception of the path from anxiety to life satisfaction in T1 and to self-rated health in T2). All paths from optimism and pessimism to the three outcomes were weak and nonsignificant. Thus, both baseline levels and changes in affectivity predicted baseline levels and changes in self-rated health, somatic depression, and life satisfaction, but neither baseline levels nor changes in optimism or pessimism had a predictive effect on these outcomes when affectivity was present in the model.
DISCUSSION
Structural equation modeling of data from a relatively large sample of elderly, independently-living respondents revealed that when optimism, pessimism, negative and positive affectivity (anxiety and happiness) were tested together as concurrent and longitudinal predictors of self-rated health, somatic depression and life satisfaction, only the affectivity factors significantly predicted all three outcomes, as well as changes in these outcomes. This finding is in line with our hypothesis. The most straightforward interpretation of these findings is that pessimism is one of many manifestations of the broader trait of negative affectivity, and therefore is indistinguishable from it. This interpretation supports Smith et al.’s (1989) argument and many of the findings in the literature, as reviewed earlier. It is also an interpretation that offers more parsimony in the conceptualization and use of personality measures.
Another interpretation would be to view both dispositional optimism and affectivity as parts of a broader system, which regulates daily cognitions, emotions, and behaviors. Though they may be related, and in some cases indistinguishable, they may have different functions in regard to some outcomes, or under certain conditions. As mentioned earlier, according to the theoretical model underlying the concept of dispositional optimism, this trait has a motivating role: People who have positive outcome expectancies have more confidence that they will attain their goals and therefore they are more likely to persist in their efforts toward their goals. Indeed, when the outcome at question required persistent action towards a specific goal, such as recovery from surgery (Scheier et al., 1999), coping with acute stress (Cohen et al., 1999), or dealing with distressing breast surgery (Montgomery et al., 2003), optimism had a unique effect that was not eliminated when negative affectivity was controlled for. Related findings showed that the effects of optimism on outcomes related to specific stressors were often mediated by coping responses (e.g., David, Montgomery, & Bovberg, 2006).
Thus, optimism may be indistinguishable from affectivity regarding general physical and mental health, as hypothesized and found here for the full RAH sample, which is a normative sample in the sense that participants were interviewed about their daily lives and were not necessarily coping with a specific stressor at the moment. At the same time, optimism could exert a unique effect in relation to outcomes that involve active coping with a health threat, as was found in the Arthritis Sub-study of the RAH study, in which optimism and pessimism were related to pain coping strategies even after controlling for anxiety or happiness (Benyamini, 2004). These seemingly contradictory findings are actually in line with the theoretical framework, which implies that under stress optimism would be more likely to play a role, and with empirical findings, showing that pessimism exacerbates the effects of stress on psychological adjustment. In light of these findings, Bromberger and Matthews (1996) suggested that “pessimism may be a more dynamic trait than the tendency toward anxiety insofar as its effects depend on the specific nature of the environmental challenges and stressors that women are experiencing” (p. 212; their study included only women).
Several limitations should be noted. First, the sample is not representative – it is overwhelmingly Caucasian, educated, and affluent. Second, the focus of the RAH study on older adults made it possible to replicate previous findings from younger samples but not to compare the results with those obtained in a younger group with the same measures and procedures. Third, positive affectivity may overlap in part with one of the outcomes studied, life satisfaction. However, the good fit of the measurement models suggests that these measures are distinct. Additionally, the inclusion of positive and negative measures among both predictors and outcomes provides a better test of the issues at question than has been provided by studies that included only negative measures in one or both sets. Fourth, our trait measure of anxiety does not cover the entire range of emotions included in the construct of neuroticism. Though this is not ideal, it is a limitation stemming from secondary analysis of data from a large longitudinal study of older adults, which has many advantages over most of the samples in which these issues have been tested. It is also worth noting that many other studies of these issues suffer from similar limitations, as they have also operationalized neuroticism using trait anxiety measures, including the Smith et al. (1989) study that initiated the controversy regarding the independence of optimism from neuroticism. Moreover, the pattern of the results suggests that even a rather narrow definition of neuroticism is sufficient to eliminate the effect of optimism.
To conclude, the findings suggest that for community samples of older adults and for measures of general well-being, dispositional optimism is redundant with measures of negative/positive affectivity, similar to findings previously reported from young samples (Smith et al., 1989). These conclusions do not contradict the possibility that for outcomes requiring active coping, under conditions of stress, dispositional optimism could contribute in unique ways that are distinct from negative and positive affectivity, as expected according to the theoretical rationale underlying the construct of dispositional optimism.
Acknowledgments
This research was supported by Grant AG03501 from the National Institute on Aging. We wish to express our deep appreciation to Howard Leventhal and Elaine Leventhal for their major role in the RAH Study and to thank them for their support of our work. We thank Amiram Vinokur and Yoav Ganzach for their helpful comments.
Footnotes
The LOT-R was not published at T1. Since Scheier et al. (1994) argued that the LOT-R enables a better test of the independence of the optimism/pessimism construct, we computed a 6-item LOT-based measure that resembled the LOT-R as closely as possible: We omitted one of the two positively-worded items that were dropped from the LOT in its revised version and the same pessimistic item that was excluded from the LOT-R.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Andersson G. The benefits of optimism: A meta-analytic review of the life orientation test. Personality and Individual Differences. 1996;21(5):719–725. [Google Scholar]
- Aspinwall LG, Taylor SE. Modeling cognitive adaptation: A longitudinal investigation of the impact of individual differences and coping on college adjustment and performance. Journal of Personality and Social Psychology. 1992;63(6):989–1003. doi: 10.1037//0022-3514.63.6.989. [DOI] [PubMed] [Google Scholar]
- Barrett P. Structural equation modelling: Adjudging model fit. Personality and Individual Differences. 2007;42(5):815–824. [Google Scholar]
- Bentler PM. EQS 6 Structural Equations Program Manual. Encino, CA: Multivariate Software, Inc; 2002. [Google Scholar]
- Benyamini Y. Can high optimism and high pessimism co-exist? Findings from arthritis patients coping with pain. Personality and Individual Differences. 2004;38(6):1463–1473. [Google Scholar]
- Benyamini Y, Leventhal H, Leventhal EA. Self-assessments of health: What do people know that predicts their mortality? Research on Aging. 1999;21(3):477–500. [Google Scholar]
- Bromberger JT, Matthews KA. A longitudinal study of the effects of pessimism, trait anxiety, and life stress on depressive symptoms in middle-aged women. Psychology and Aging. 1996;11:207–213. doi: 10.1037//0882-7974.11.2.207. [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF. On the self-regulation of behavior. Cambridge, UK: Cambridge University Press; 1998. [Google Scholar]
- Chang EC. Dispositional optimism and primary and secondary appraisal of a stressor: Controlling for confounding influences and relations to coping and psychological and physical adjustment. Journal of Personality and Social Psychology. 1998a;74(4):1109–1120. [Google Scholar]
- Chang EC. Distinguishing between optimism and pessimism: A second look at the “optimism-neuroticism” hypothesis. In: Hoffman RR, Sherrik MF, Warm JS, editors. Viewing psychology as a whole: The integrative science of William N. Dember. Washington, DC: American Psychological Association; 1998b. pp. 415–432. [Google Scholar]
- Chang EC, Maydeu-Olivares A, D’Zurilla TJ. Optimism and pessimism as partially independent constructs: Relationship to positive and negative affectivity and psychological well-being. Personality and Individual Differences. 1997;23(3):433–440. [Google Scholar]
- Cheng ST, Hamid PN. Dispositional optimism in Chinese people: What does the Life Orientation Test Measure? International Journal of Psychology. 1997;32(1):15–22. [Google Scholar]
- Cohen F, Kearney KA, Zegans LS, Kemeny ME, Neuhaus JM, Stites DP. Differential immune system changes with acute and persistent stress for optimists vs pessimists. Brain, Behavior, and Immunity. 1999;13:155–174. doi: 10.1006/brbi.1998.0531. [DOI] [PubMed] [Google Scholar]
- David D, Montgomery GH, Bovberg DH. Relations between coping responses and optimism-pessimism in predicting anticipatory psychological distress in surgical breast cancer patients. Personality and Individual Differences. 2006;40:203–213. doi: 10.1016/j.paid.2005.05.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ebert SA, Tucker DC, Roth DL. Psychological resistance factors as predictors of general health status and physical symptom reporting. Psychology, Health & Medicine. 2002;7(3):363–375. [Google Scholar]
- Hu L-t, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equations Modeling. 1999;6(1):1–55. [Google Scholar]
- Idler EL, Benyamini Y. Self-rated health and mortality: A review of 27 community studies. Journal of Health and Social Behavior. 1997;38(1):21–37. [PubMed] [Google Scholar]
- Isaacowitz DM. Correlates of well-being in adulthood and old age: A tale of two optimisms. Journal of Research in Personality. 2005;39:224–244. [Google Scholar]
- Kunzmann U, Little TD, Smith J. Is age-related stability of subjective well-being a paradox? Cross-sectional and longitudinal evidence from the Berlin Aging Study. Psychology and Aging. 2000;15(3):511–526. doi: 10.1037//0882-7974.15.3.511. [DOI] [PubMed] [Google Scholar]
- McNair C, Lorr M, Droppleman L. Profile of mood states. San Diego, CA: Educational and Industrial Testing Service; 1971. [Google Scholar]
- Montgomery GH, David D, Goldfarb AB, Silverstein JH, Weltz CR, Birk JS, Bovberg DH. Sources of anticipatory distress among breast surgery patients. Journal of Behavioral Medicine. 2003;26(2):153–164. doi: 10.1023/a:1023034706298. [DOI] [PubMed] [Google Scholar]
- Mroczek DK, Spiro A, Aldwin CM, Ozer DJ, Bosse R. Construct validation of optimism and pessimism in older men: Findings from the Normative Aging Study. Health Psychology. 1993;12(5):406–409. doi: 10.1037//0278-6133.12.5.406. [DOI] [PubMed] [Google Scholar]
- Mulaik S. There is a place for approximate fit in structural equation modelling. Personality and Individual Differences. 2007;42(5):883–891. [Google Scholar]
- Plomin R, Scheier MF, Bergeman CS, Pedersen NL, Nesselroade JR, McClearn GE. Optimism, pessimism and mental health: a twin/adoption analysis. Personality and Individual Differences. 1992;13(8):921–930. [Google Scholar]
- Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Robbins AS, Spence JT, Clark H. Psychological determinants of health and performance: The tangled web of desirable and undesirable characteristics. Journal of Personality and Social Psychology. 1991;61:755–765. doi: 10.1037//0022-3514.61.5.755. [DOI] [PubMed] [Google Scholar]
- Robinson-Whelen S, Kim C, MacCallum RC, Kiecolt-Glaser JK. Distinguishing optimism from pessimism in older adults: Is it more important to be optimistic or not to be pessimistic? Journal of Personality and Social Psychology. 1997;73(6):1345–1353. doi: 10.1037//0022-3514.73.6.1345. [DOI] [PubMed] [Google Scholar]
- Satorra A, Bentler PM. Corrections to test statistics and standard errors in covariance structure analysis. In: von Eye A, Clogg CC, editors. Latent Variable Analysis: Applications to Developmental Research. Thousand Oaks, CA: Sage; 1994. pp. 399–419. [Google Scholar]
- Scheier MF, Carver CS. Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychology. 1985;4:219–247. doi: 10.1037//0278-6133.4.3.219. [DOI] [PubMed] [Google Scholar]
- Scheier MF, Carver CS. Dispositional optimism and physical well-being: The influence of generalized outcome expectancies on health. Journal of Personality. 1987;55(2):169–210. doi: 10.1111/j.1467-6494.1987.tb00434.x. [DOI] [PubMed] [Google Scholar]
- Scheier MF, Carver CS. A model of behavioral self-regulation: Translating intention into action. In: Berkowitz L, editor. Advances in Experimental Social Psychology. Vol. 21. San Diego, California: Academic Press; 1988. pp. 303–346. [Google Scholar]
- Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. Journal of Personality and Social Psychology. 1994;67(6):1063–1078. doi: 10.1037//0022-3514.67.6.1063. [DOI] [PubMed] [Google Scholar]
- Scheier MF, Carver CS, Bridges MW. Optimism, pessimism, and psychological well-being. In: Chang EC, editor. Optimism and Pessimism: Implications for theory, research, and practice. Washington, D.C: American Psychological Association; 2001. pp. 189–216. [Google Scholar]
- Scheier MF, Matthews KA, Owens JF, Schulz R, Bridges MW, Magovern GJ, Carver CS. Optimism and rehospitalization after coronary artery bypass graft surgery. Archives of Internal Medicine. 1999;159:829–835. doi: 10.1001/archinte.159.8.829. [DOI] [PubMed] [Google Scholar]
- Smith TW, Pope MK, Rhodewalt F, Poulton JL. Optimism, neuroticism, coping, and symptom reports: An alternative interpretation of the Life Orientation Test. Journal of Personality and Social Psychology. 1989;56(4):640–648. doi: 10.1037//0022-3514.56.4.640. [DOI] [PubMed] [Google Scholar]
- Smith TW, Spiro A. Personality, health, and aging: Prolegomenon for the next generation. Journal of Research in Personality. 2002;36(4):363–394. [Google Scholar]
- Usala P, Hertzog C. Measurement of affective states in adults: Evaluation of an adjective rating scale instrument. Research on Aging. 1989;11:403–426. doi: 10.1177/0164027589114001. [DOI] [PubMed] [Google Scholar]