

Percutaneous image guided techniques have recently been applied to the management of small renal tumors. Persistent hematuria despite embolization of a 7 cm. renal cell carcinoma was successfully treated with percutaneous radio frequency ablation in a patient with a solitary kidney.
CASE REPORT
A 71-year-old man with coronary artery disease and chronic renal insufficiency (creatinine 2.0 to 2.5) presented with 6 weeks of gross hematuria requiring repeated blood transfusion and continuous bladder irrigation. He had undergone left nephrectomy 6 years previously for renal cell carcinoma, and was currently receiving chemoimmunotherapy for lung metastases and a contralateral 7 cm. renal tumor (fig. 1). No lower tract source of bleeding was identified, and so embolization of the contralateral renal tumor was considered.1 Complete embolization was not attempted given the solitary kidney and underlying renal insufficiency. Selective embolization was performed using polyvinyl alcohol particles, and the 2 primary segmental feeders were successfully occluded but gross hematuria continued. The patient refused surgical management and so was considered for percutaneous radio frequency ablation.
Fig. 1.
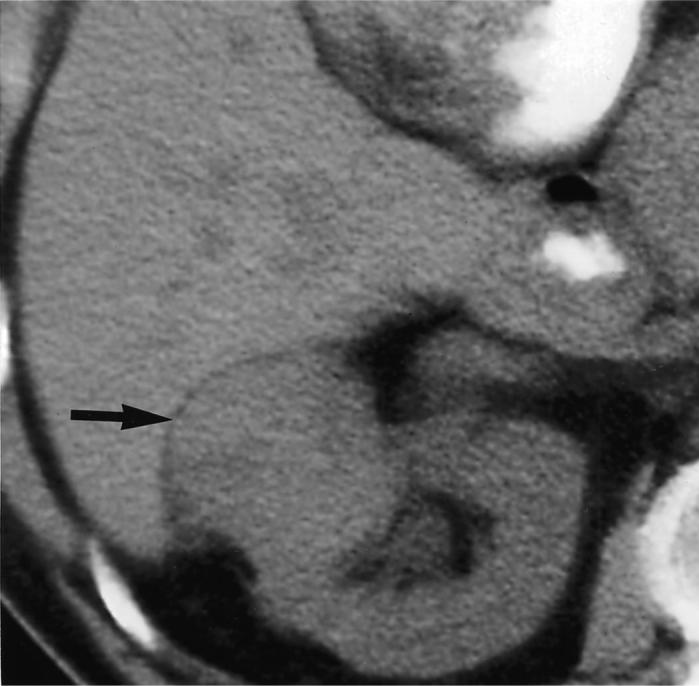
Unenhanced computerized tomography demonstrates exophytic right kidney tumor (arrow).
After obtaining informed consent, he was brought to the interventional radiology suite, where under conscious sedation and ultrasound monitoring a 17.5 gauge radio frequency probe was percutaneously placed into the renal tumor. A single 3 cm. active tip needle-probe and 200 watt, 480 kHz. ablation system were used to deliver 3, 12-minute sessions of radio frequency energy to overlapping spheres in the tumor.
Gross hematuria resolved during the next 24 hours and continuous bladder irrigation was discontinued 2 days thereafter. Followup magnetic resonance imaging (MRI) with gadolinium 4 weeks later revealed low signal areas consistent with necrosis in the tumor. However, the tumor was only partially ablated, as enhancement was noted toward the renal pelvis at the periphery of the thermal lesion (fig. 2). At 5-month followup MRI showed interval growth of the enhancing part of the tumor but no change in overall size. Gross hematuria resolved for 8 months at which time it recurred and resolved without repeat intervention. Creatinine remained stable during the 8-month followup.
Fig. 2.
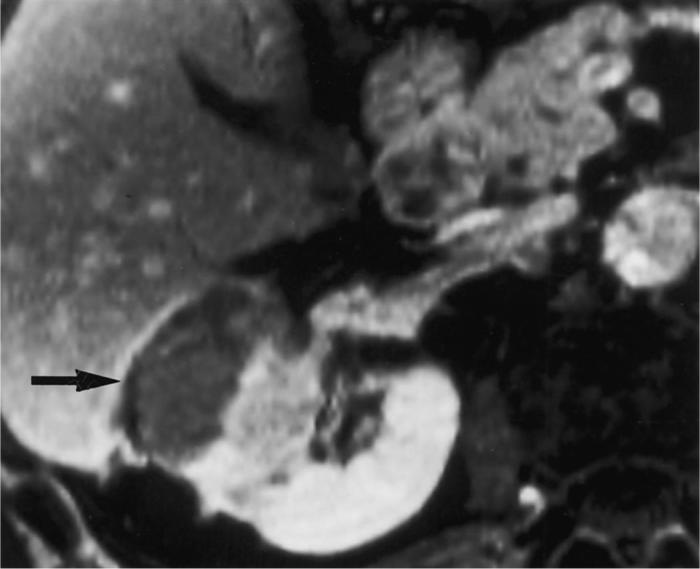
T1-weighted fat suppressed enhanced MRI shows coagulative necrosis at lateral margin of tumor (arrow), with medullary enhancement likely representing residual viable tumor.
DISCUSSION
Persistent hematuria from renal cell carcinoma was successfully managed in a patient with chronic renal insufficiency and a solitary kidney. Radio frequency ablation was selected after selective embolization with polyvinyl alcohol particles failed. Selective embolization was technically difficult in this patient, given the multiple layers of vascularity within the exophytic, cortical and medullary components of the tumor (fig. 1). Less selective embolization may have arrested the bleeding but would have placed renal function and more renal parenchyma at risk. Therefore, radio frequency ablation was performed as a secondary treatment.
Percutaneous, image guided radio frequency ablation can safely treat selected renal tumors while sparing normal kidney parenchyma,2 although it is still unknown whether it can provide long-term cancer control. In our case radio frequency ablation succeeded in treating gross hematuria such that the patient was able to receive systemic therapy for metastatic disease without the need for nephrectomy and/or dialysis. Ultrasound guided percutaneous radio frequency ablation may be a useful alternative management modality for upper tract hematuria in select patients, and mandates further study as an adjunct to selective embolization.3
REFERENCES
- 1.Kalman D, Varenhorst E. The role of arterial embolization in renal cell carcinoma. Scand J Urol Nephrol. 1999;33:162. doi: 10.1080/003655999750015934. [DOI] [PubMed] [Google Scholar]
- 2.Gervais DA, McGovern FJ, Wood BJ, et al. Radiofrequency ablation of renal cell carcinoma: early clinical experience. Radiology. 2000;217:665. doi: 10.1148/radiology.217.3.r00dc39665. [DOI] [PubMed] [Google Scholar]
- 3.Hall WH, McGahan JP, Link DP, et al. Combined embolization and percutaneous radiofrequency ablation of a solid renal tumor. AJR Am J Roentgenol. 2000;174:1592. doi: 10.2214/ajr.174.6.1741592. [DOI] [PubMed] [Google Scholar]