

Abstract
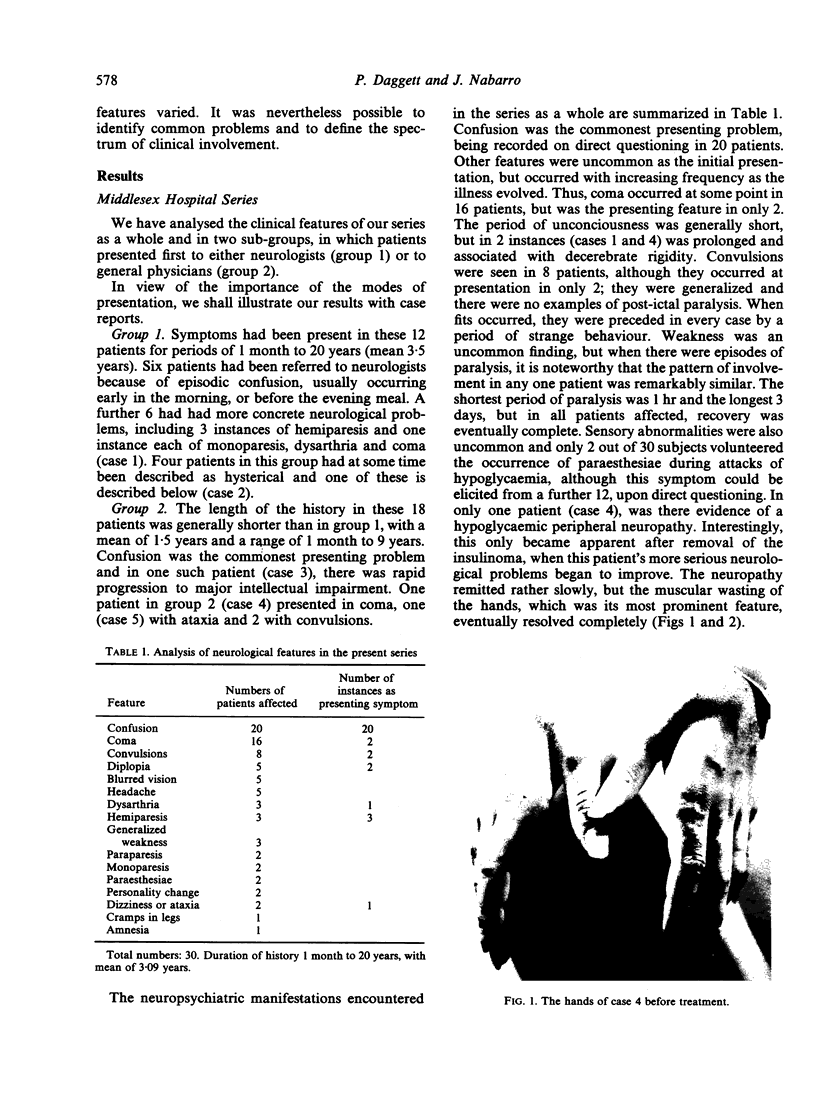
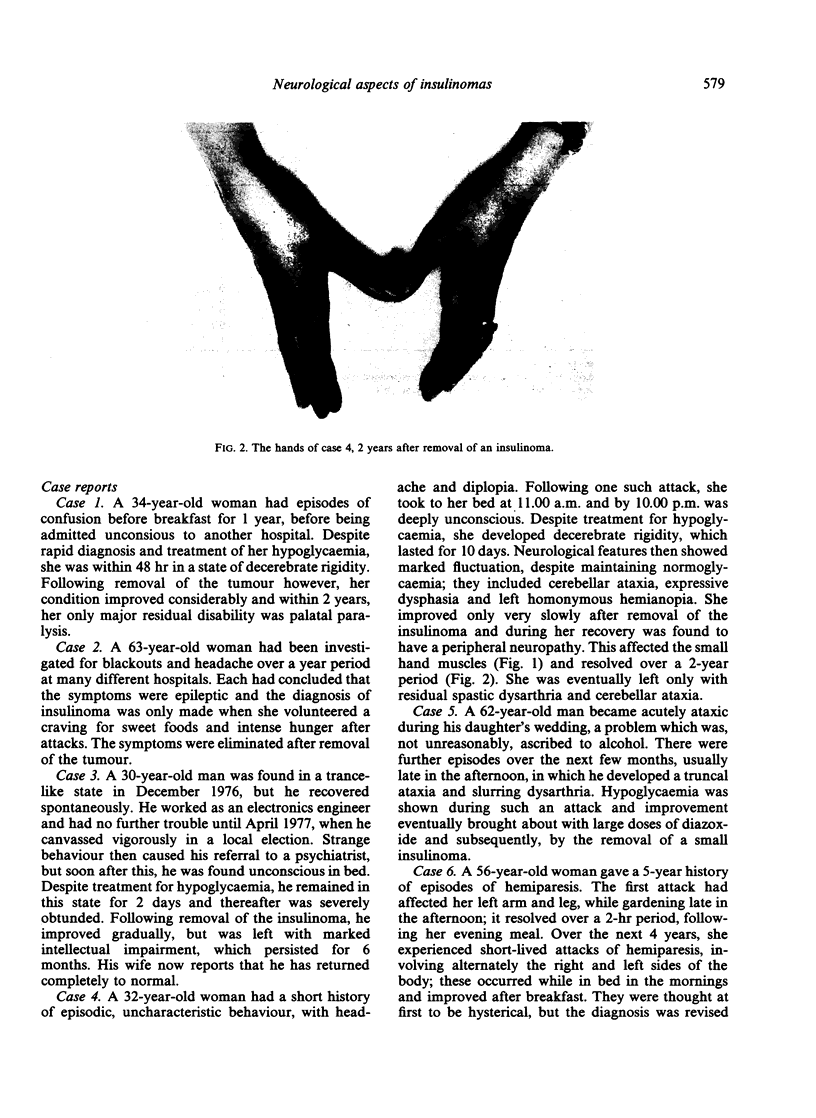
Neurological involvement occurred in every one of a series of 30 patients with an insulinoma. The episodic nature of the hypoglycaemia caused symptoms and signs to fluctuate and often led to delay in diagnosis (mean length of history was 3 years). The commonest feature at first presentation was confusion (20 instances), but as the illness evolved, coma (16 instances) and convulsions (8 instances) became more frequent. Objective weakness was found in 7 patients, with 3 examples of hemiparesis and 2 each of paraparesis and monoparesis; in all, the weakness resolved over a period of 1 hr to 3 days when normoglycaemia was maintained. Other neurological features included subjective visual disturbances, headache, dysarthria and ataxia. 220 patients with an insulinoma from 7 series in the literature were reviewed. The high incidence of neurological features was confirmed, with confusion (152 cases), coma (82 cases) and convulsions (58 cases) predominating. Visual disturbances were common, though not accurately quantified in some series. Objective evidence of weakness on the other hand was reported in only 6 of the 222 patients. Other less common symptoms included headache (18 instances) and peripheral paraesthesiae (14 instances). In the 7 series reviewed, as in our own, it was found that in any one patient, each episode of hypoglycaemia was accompanied by the same symptom complex. The presence of an insulinoma should be considered in any patient with unusual, or inexplicable neurological features, particularly when they are intermittent. The diagnosis can be confirmed by demonstrating an inappropriately high circulating insulin level, for the ambient blood glucose concentration.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Best J. D., Chisholm D. J., Alford F. P. Insulinoma: poor recognition of clinical features is the major problem in diagnosis. Med J Aust. 1978 Jul 1;2(1):1–5. doi: 10.5694/j.1326-5377.1978.tb131299.x. [DOI] [PubMed] [Google Scholar]
- Clarke M., Crofford O. B., Graves H. A., Jr, Scott H. W., Jr Functioning beta cell tumors (insulinomas) of the pancreas. Ann Surg. 1972 Jun;175(6):956–974. doi: 10.1097/00000658-197206010-00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frerichs H., Creutzfeldt W. Hypoglycaemia. 1. Insulin secreting tumours. Clin Endocrinol Metab. 1976 Nov;5(3):747–767. doi: 10.1016/s0300-595x(76)80049-7. [DOI] [PubMed] [Google Scholar]
- Galbut D. L., Markowitz A. M. Insulinoma: diagnosis, surgical management and long-term follow-up. Review of 41 cases. Am J Surg. 1980 May;139(5):682–690. doi: 10.1016/0002-9610(80)90363-3. [DOI] [PubMed] [Google Scholar]
- Glickman M. H., Hart M. J., White T. T. Insulinoma in Seattle: 39 cases in 30 years. Am J Surg. 1980 Jul;140(1):119–125. doi: 10.1016/0002-9610(80)90427-4. [DOI] [PubMed] [Google Scholar]
- Jaspan J. B., Wollman R. L., Bernstein L., Rubenstein A. H. Hypoglycemic peripheral neuropathy in association with insulinoma: implication of glucopenia rather than hyperinsulinism. Case report and literature review. Medicine (Baltimore) 1982 Jan;61(1):33–44. [PubMed] [Google Scholar]
- Jayasinghe K. S., Nimalasuriya A., Dharmadasa K. A case of insulinoma with peripheral neuropathy. Postgrad Med J. 1983 Mar;59(689):189–190. doi: 10.1136/pgmj.59.689.189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubenstein A. H., Block M. B., Starr J., Melani F., Steiner D. F. Proinsulin and C-peptide in blood. Diabetes. 1972;21(2 Suppl):661–672. doi: 10.2337/diab.21.2.s661. [DOI] [PubMed] [Google Scholar]
- SCHEINBERG P. OBSERVATIONS ON CEREBRAL CARBOHYDRATE METABOLISM IN MAN. Ann Intern Med. 1965 Feb;62:367–371. doi: 10.7326/0003-4819-62-2-367. [DOI] [PubMed] [Google Scholar]
- Service F. J., Dale A. J., Elveback L. R., Jiang N. S. Insulinoma: clinical and diagnostic features of 60 consecutive cases. Mayo Clin Proc. 1976 Jul;51(7):417–429. [PubMed] [Google Scholar]
- Service F. J., Horwitz D. L., Rubenstein A. H., Kuzuya H., Mako M. E., Reynolds C., Molnar G. D. C-peptide suppression test for insulinoma. J Lab Clin Med. 1977 Jul;90(1):180–186. [PubMed] [Google Scholar]
- Stellon A., Townell N. H. C-peptide assay for factitious hyperinsulinism. Lancet. 1979 Jul 21;2(8134):148–149. doi: 10.1016/s0140-6736(79)90029-1. [DOI] [PubMed] [Google Scholar]
- Sved S., McGilveray I. J., Beaudoin N. Assay of sulfonylureas in human plasma by high-performance liquid chromatography. J Pharm Sci. 1976 Sep;65(9):1356–1359. doi: 10.1002/jps.2600650924. [DOI] [PubMed] [Google Scholar]
- Turner R. C., Harris E. Diagnosis of insulinomas by suppression tests. Lancet. 1974 Jul 27;2(7874):188–190. doi: 10.1016/s0140-6736(74)91484-6. [DOI] [PubMed] [Google Scholar]