

Abstract
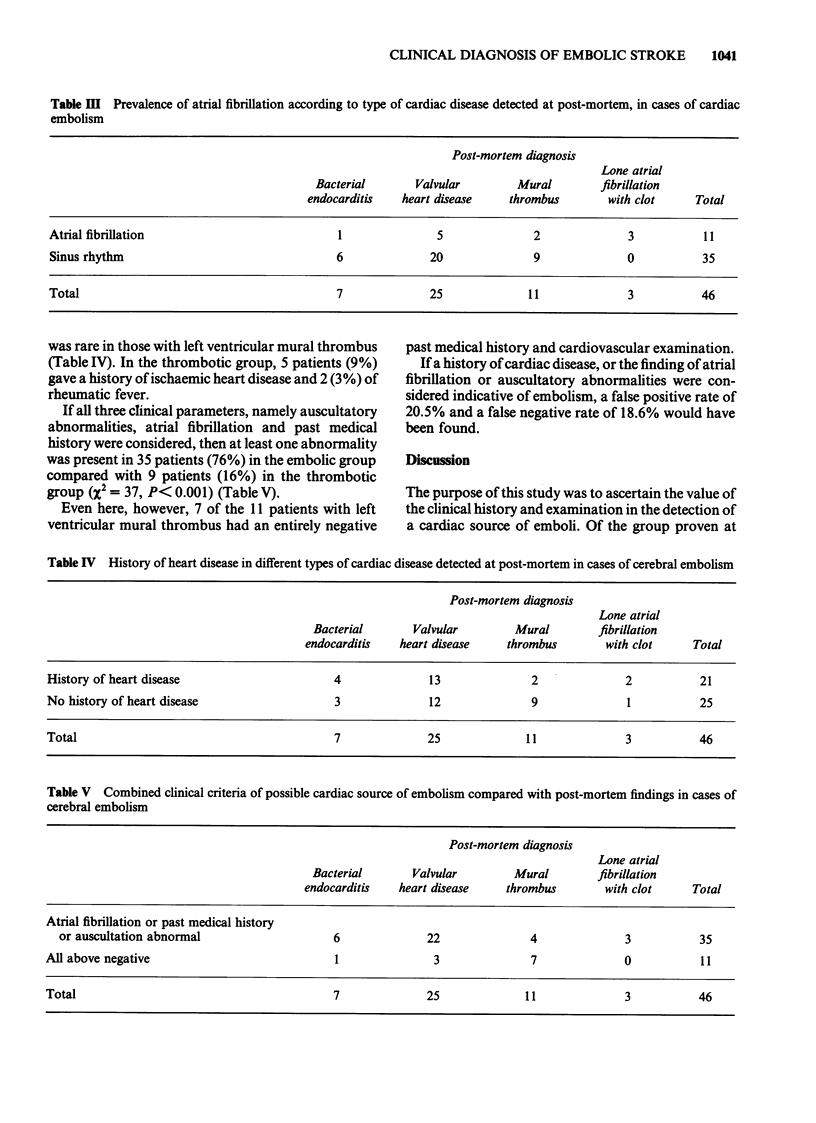
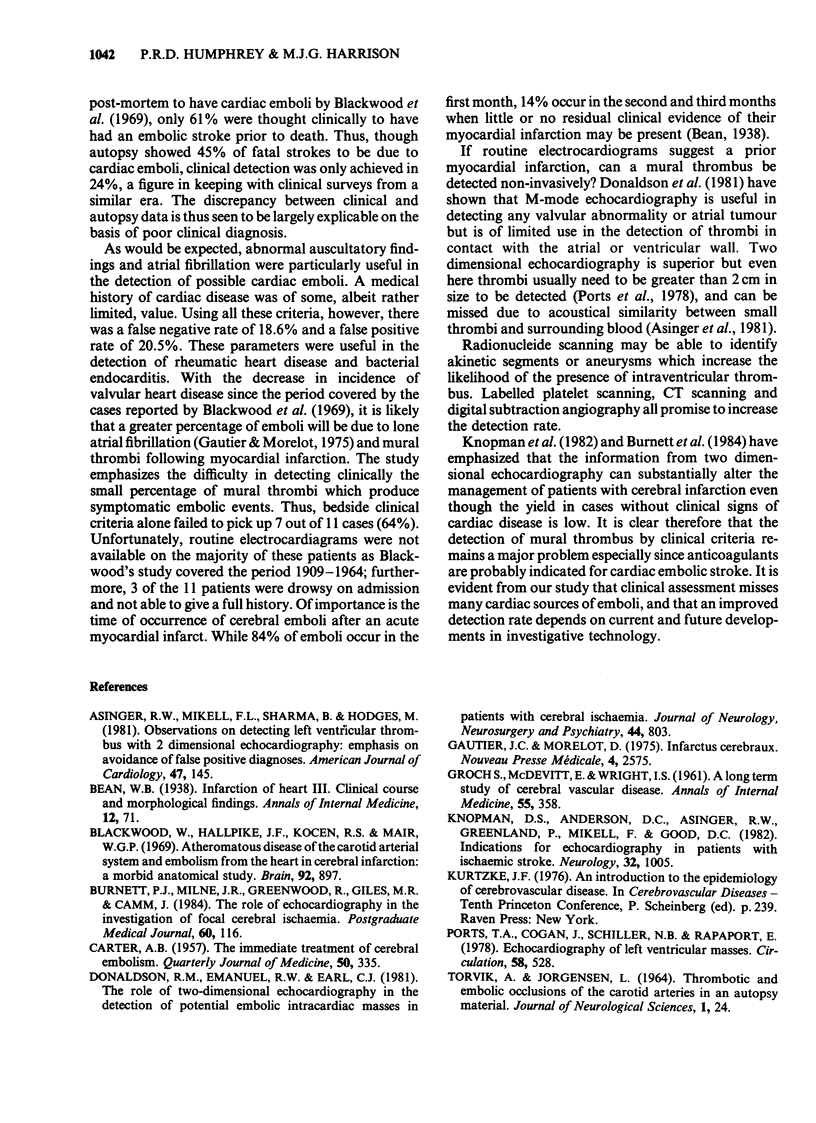
A retrospective case note survey of 103 autopsy proven cases of cerebral infarction was carried out to assess how often a cardiac source for embolism had been correctly suspected on clinical grounds. Only 61% of 46 patients with cardiac embolic sources were so identified. Cases of rheumatic heart disease and bacterial endocarditis were more frequently identified than cases of mural thromboembolism from ischaemic heart disease. This relative failure of unaided clinical diagnostic criteria probably accounts for the discrepancy between the autopsy evidence of cardiac embolism as a cause of stroke (about 40%), and clinical studies (about 20%).
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Asinger R. W., Mikell F. L., Sharma B., Hodges M. Observations on detecting left ventricular thrombus with two dimensional echocardiography: emphasis on avoidance of false positive diagnoses. Am J Cardiol. 1981 Jan;47(1):145–156. doi: 10.1016/0002-9149(81)90303-9. [DOI] [PubMed] [Google Scholar]
- Blackwood W., Hallpike J. F., Kocen R. S., Mair W. G. Atheromatous disease of the carotid arterial system and embolism from the heart in cerebral infarction: a morbid anatomical study. Brain. 1969;92(4):897–910. doi: 10.1093/brain/92.4.897. [DOI] [PubMed] [Google Scholar]
- Burnett P. J., Milne J. R., Greenwood R., Giles M. R., Camm J. The role of echocardiography in the investigation of focal cerebral ischaemia. Postgrad Med J. 1984 Feb;60(700):116–119. doi: 10.1136/pgmj.60.700.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CARTER A. B. The immediate treatment of cerebral embolism. Q J Med. 1957 Jul;26(103):335–348. [PubMed] [Google Scholar]
- Donaldson R. M., Emanuel R. W., Earl C. J. The role of two-dimensional echocardiography in the detection of potentially embolic intracardiac masses in patients with cerebral ischaemia. J Neurol Neurosurg Psychiatry. 1981 Sep;44(9):803–809. doi: 10.1136/jnnp.44.9.803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GROCH S. N., McDEVITT E., WRIGHT I. S. A long-term study of cerebral vascular disease. Ann Intern Med. 1961 Sep;55:358–367. doi: 10.7326/0003-4819-55-3-358. [DOI] [PubMed] [Google Scholar]
- Gautier J. C., Morelot D. Infarctus cérébraux. Etude de leur prévention. Nouv Presse Med. 1975 Oct 25;4(36):2575–2580. [PubMed] [Google Scholar]
- Knopman D. S., Anderson D. C., Asinger R. W., Greenland P., Mikell F., Good D. C. Indications for echocardiography in patients with ischemic stroke. Neurology. 1982 Sep;32(9):1005–1011. doi: 10.1212/wnl.32.9.1005. [DOI] [PubMed] [Google Scholar]
- Ports T. A., Cogan J., Schiller N. B., Rapaport E. Echocardiography of left ventricular masses. Circulation. 1978 Sep;58(3 Pt 1):528–536. doi: 10.1161/01.cir.58.3.528. [DOI] [PubMed] [Google Scholar]