

Abstract
While excellent adolescent alcohol and drug screening tools are available, there are relatively few, if any, psychometrically validated measures to use in the assessment of adolescent treatment outcome. This study conducted a test-retest exercise of the Form 90 Drug and Alcohol (Form 90 DnA) to determine the stability of adolescent responses when administering the day-by-day calendar/grid approach. Homeless youth (N = 37) with alcohol, drug, or alcohol and drug abuse/dependence combined were recruited to participate in the test-retest study. High pre-post stability in means was obtained on measures of frequency of substance use in general, and on specific measures of alcohol, cocaine, marijuana use. The findings from this paper provide support for the reliability and validity of the Form 90 for use with adolescent runaways with a substance abuse or dependence diagnosis.
Keywords: Runaway and homeless youth, adolescent substance abuse, alcohol and drug assessment
Substantial resources are invested in adolescent substance abuse treat ment, but the relative outcomes of different kinds of such treatment remain, at best, circumstantial. In comparison to over 1,000 alcohol treatment outcome studies with adults (Miller et al., 1995), for example, William and Chang (2000) were able to locate and review only 53 empirical studies investigating the relative effectiveness of treatments for adolescents. The reason for our poor understanding of the relative treatment outcomes, however, is not fully explained by the absence of empirical investigations. A second contributing factor is that the reliability and validity of outcome measures applied in adolescent research is generally unclear, and at times ignored (Winters, 1990; Owen & Nyberg, 1983). Thus, it is currently difficult to interpret individual study findings as well as to meaningfully integrate findings across studies using meta-analytic techniques.
Clearly, the development of reliable screening and treatment planning assessments for adolescents has overshadowed the equally important need for reliable outcome measures. Excellent measures, for instance, are available to assess adolescent-specific substance abuse problems (e.g., RAPI; PEI), DSM substance abuse diagnosis, (e.g., ADI), and adolescent life functioning across diverse domains (e.g., T-ASI; DUSI). In the context of the high cost and efforts of conducting follow-up studies it makes sense to have highly reliable measures of adolescent substance use behaviors.
Why the lack of reliable treatment outcome tools to measure adolescent substance use or, more precisely, why the lack of interest in assessing the reliability of outcome measures applied in adolescent studies? On the one hand, researchers have indiscriminately applied measures and procedures standardized with adult samples to adolescents (Lecesse & Waldron, 1994) in spite of the well-documented differences between adults and adolescents in drinking patterns and use of illicit substances, with the belief that reliability and validity were not adversely affected, or at least not seriously so. Practitioners, on the other hand, have tended to use assessments developed for treatment planning, e.g., T-ASI, as outcome measures for reasons of familiarity and practicality.
The purpose of this study was to investigate the reliability and validity of the Form 90 semi-structured interview when administered to runaway adolescent substance abusers. The Form 90 combines the strengths of the day-by-day calendar approach to reconstructing substance use (Sobell & Sobell, 1992) with a weekly grid procedure to expedite the interview process (Miller & Marlatt, 1984). With treatment seeking adults, the Form 90 has demonstrated excellent test-retest reliability with alcohol (Tonigan et al., 1997) and drug (Westerberg et al., 1998) abusers.
Waldron et al. (2001) provided support for the convergent validity of the Form 90 with adolescent substance users. Bivariate correlations showed convergence between adolescent self-reported marijuana use and parent (r = .37) and sibling report (r = .55) of the adolescent’s use. Additionally, frequency of use was correlated with problem consequences (r = .41) and parent report of externalizing problems (r = .26). Though 99% of youth reported marijuana use in the prior 90 days, 83% of youth also had positive urine findings, indicating a convergence between self-report and biologic measures.
Special populations such as the homeless, school dropouts or those with concurrent mental health problems present with more complex and enduring problems (Gilvarry, 2000). Establishing the reliability of assessment instruments for use with adolescent special populations is a priority for those developing treatment interventions.
METHOD
Participants
Runaway youth (N = 37) were recruited through two runaway/homeless shelters in a southwestern city as part of two larger studies examining family therapy outcome with substance abusing runaway adolescents (grants R29DA11590 and R01AA12173). All youth in this sample agreed to the possibility of family treatment with a parent or surrogate parent. To be eligible for participation, adolescents had to satisfy DSM IV diagnostic criteria for substance abuse or dependence, be between the ages of 12 to 17, and reside within a 60-mile radius of the research site.
Procedure
Participants already engaged into the larger clinical trial were engaged into the test-retest study, and all youth met DSM criteria for a substance abuse or dependence diagnosis. Recruitment began with a review of the nature and conditions of the test-retest study, a formal review of the elements of informed consent, and a signing of the consent statement. The youth’s primary caretaker was then contacted and consent was obtained.
The retest assessment was completed within 7 to 14 days from the original pretreatment assessment by a different interviewer. Interviewers were instructed not to discuss, share, or in any way inform one another about the content or process of a Form 90 interview. The assessment period of the Form-90 was a 90-day retrospective period defined from the day of the test administration, and both test and retest interviews covered the same 90-day interval. Youth were paid $10 for completing the second interview.
Interviewers
Six trained interviewers participated in the test-retest study. All interviewers had substantial experience in conducting Form 90 interviews developed through their research duties on NIAAA and NIDA funded studies of adolescent substance use (R29DA11590 and R01AA12173). Two of the 6 interviewers were graduate level trained research assistants, and four were full-time staff with undergraduate degrees in psychology. All interviewers initially had received formal training in the administration of the Form 90 by center staff, and continuing supervision of Form 90 assessment procedures was structured into each grant, typically on a bi-weekly basis.
Materials
The examiner administered a Demographic Questionnaire assessing a set of core variables used to characterize and compare samples included in the study. These demographic items include age, gender, self-identified ethnicity, parent and sibling information, education, income sources, number of previous runaway episodes, days on the street, and homeless and victimization experiences.
The Computerized Diagnostic Interview Schedule for Children (CDISC, Shaffer, 1992), is a computerized structured interview containing 263 items pertinent to a comprehensive psychiatric diagnostic interview based upon DSM-IV criteria, and includes modules to diagnose alcohol, tobacco and other substance abuse and dependence. The diagnosis for other substance abuse specifies drug class, including stimulants, sedatives, opiates, hallucinogens, etc. In addition to diagnostic screening for Psychoactive Substance Use and Psychosis, sections on Conduct Disorder, ADHD, Oppositional Defiant Disorder, Mood, Eating and Anxiety disorders were also administered. These diagnoses provide important information relating to comorbidity among homeless, substance abusing adolescents. CDISC was developed specifically to diagnose children and adolescents, is prominent in the field (Winters & Stinchfield, 1995) and has been used with homeless youth (Morgan & Cauce, 1999; Mundy et al., 1990; Warheit & Biafora, 1991).
The Beck Depression Inventory (BDI, Beck, Ward, Mendelson, Mock & Erlbaugh, 1961) is the most frequently used self-report instrument for assessment of mood, cognitive and somatic aspects of depression, and has been used with homeless youth (Miner, 1991; Maxwell, 1992), and has shown good psychometric properties. Estimates of internal consistency and test-retest reliability are high, and the measure appears sensitive to depression severity across community and clinical populations (Norman, Miller, & Klee, 1983; Rush et al., 1986).
To address problem consequences, the POSIT (Rahdert, 1991) was developed to identify all possible functional areas which are most affected by, or associated with, an adolescent’s drug abuse. Although the POSIT has demonstrated good psychometric properties (McLaney, Delboca and Babor, 1994) its length has been a concern to practitioners and researchers. The POST-SF (Danseco & Marques, 2000) has 78 items and 8 scales: substance use/abuse, mental and physical health, family relations, peer relations, educational status, vocational status, social skills and leisure, and aggressive behavior/delinquency. The POSIT-SF was developed using secondary data analysis of full-length POSIT scores (Chamberlain et al. 1998). The original POSIT validation sample was then used to further examine the reliability and validity of the POSIT-SF (Klitzner, Gruenwald, Taff, Behringer & Harol, 1993).
Another measure of problems associated with drinking, the Adolescent Drinking Index (ADI; Harrell & Wirtz, 1989a, 1989b) was utilized. This instrument differentiates adolescents whose drinking poses a problem for their functioning from adolescents whose drinking does not. The scale consists of 24 self-report items, requires 5 minutes to complete, and was normed and validated with adolescent samples.
The Form 90, developed for NIAAA funded Project Match (Miller, 1996), combines the timeline follow-back method (Sobell & Sobell, 1992) and grid averaging (Miller & Marlatt, 1984). Form 90-D drug interview is adapted from the Form 90-A alcohol interview which has shown excellent test-retest reliability for indices of drug use in major categories (Tonigan, Miller, & Brown, 1997) with kappas for different drug classes ranging from .74 to 1.0. Form 90-D Intake Form (Form 90 DI) and Form 90 Drug Follow-up Form (Form 90 DF) is a structured interview and uses a timeline follow-back procedure to yield a daily reconstruction of all drug classes, including alcohol, and has also shown good reliability and validity with adult substance users (Westerberg, Tonigan, & Miller, 1998). This interview measure will yield total number of days, in the last 90, of all drug use, total number of drugs used, age at first use, lifetime weeks of use, level of use (single use, several uses, or heavy use), as well as school and work attendance, living situation and health care utilization.
RESULTS
A total of 37 adolescents participated in the test-retest study, with no youth refusing to participate. Male (n = 18) and female (n = 19) adolescents were equally represented. The average age of the youth was 15.16 (SD = 1.40) years (range 12 to 17). The mean grade level completed was 9.19 (SD = 1.47), and 16 (43.2%) of the participants reported that they were currently not attending school. A majority of the youth self-identified as being Hispanic, Mexican, or New Mexican (54%, n = 20), about 22% were Non-Hispanic Whites (n = 8), and the remaining 9 adolescents were African American, Asian, Native American, and Other. Although all youth in the project were recruited during their stay at a runaway shelter, a majority of the adolescents reported that in the three months prior to their stay at the shelter, they lived primarily with their parents (n = 29; 78.4%) or with their friends (n = 5; 13.5%). Three adolescents indicated that they lived primarily with other relatives, foster parents, or alone.
Table 1 provides substance use diagnosis, psychiatric symptomatology, and social/legal of the sample at the time of study recruitment. All participants but one received a CDIS diagnosis of alcohol, drug, or alcohol and drug abuse or dependence. This one youth met criteria based upon DSM IV symptom requirements for marijuana abuse, but did not receive a positive diagnosis on the computer inventory. Seventeen (45.9%) were diagnosed with alcohol and drug abuse/dependence, 7 (18.9%) with only alcohol abuse/dependence, and 13 (35.1%) with drug abuse/dependence only. Adolescents in this sample reported, on average, highly disruptive and chaotic lifestyles, characterized by frequent arrest, being victims of physical and sexual abuse, carrying weapons, and selling drugs for financial support. On average, parents of the adolescents held a high school diploma, and earned about 20,000 per year to support about 4 family members. On average, youth reported mild depression as reported on the BDI, and approximately half met diagnostic criteria for conduct disorder, while approximately 14% met criteria for posttraumatic stress disorder.
TABLE 1.
Test-Retest Sample Characteristics
| Male n = 18 | Female n = 19 | p | |
|---|---|---|---|
| Substance Use | |||
| Alcohol Abuse (CDIS) | 3 (16.7%) | 4 (21.1%) | p < .73 |
| Alcohol Dependence (CDIS) | 6 (33.3%) | 11 (57.9%) | p < .13 |
| Marijuana Abuse (CDIS) | 6 (33.3%) | 7 (36.8%) | p < .82 |
| Marijuana Dependence (CDIS) | 9 (50.0%) | 7 (36.8%) | p < .42 |
| Psychiatric Symptoms | |||
| Beck Depression Inventory | 12.22 (11.25) | 14.16 (13.64) | p < .64 |
| Conduct Disorder (CDIS) | 10 (55.6%) | 6 (31.6%) | p < .14 |
| PTSD (CDIS) | 3 (16.7%) | 2 (10.5%) | p < .66 |
| Social | |||
| Persons in Home | 4.17 (1.47) | 4.79 (1.51) | P < .21 |
| Last Grade Completed | 8.78 (1.06) | 7.89 (1.15) | p < .02 |
| Annual Family Income | 20,573 (30,741) | 23,948 (24,163) | p < .71 |
| Primary Caretaker Grade Level | 12.56 (2.92) | 12.00 (2.85) | p < .56 |
| Number of Times Arrested | 4.18 (5.10) | 1.73 (3.26) | p < .12 |
| Number of Times Runaway | 6.22 (8.47) | 5.89 (11.18) | p < .92 |
| Percent Ever in Group Home | 44.4% (8) | 36.8% (7) | p < .64 |
| Percent in Jail Overnight | 44.4% (8) | 15.8 (3) FF | p < .08 |
| Victim of Sexual Abuse | 0 % (0) | 5 (26.3%) FF | p < .05 |
| Victim Physical Abuse | 8 (44.4%) | 8 (42.1%) | p < .89 |
| Financial Support Selling Drugs | 10 (55.6%) | 4 (21.1%) | p < .03 |
| Victim Sexual Assault | 0 (0%) | 6 (31.6%) FF | p < .02 |
| Percent Carry Weapon for Safety | 11 (61.1%) | 3 (15.8%) FF | p < .01 |
Four of the six interviewers conducted both test and retest assessments (n = 23), never with the same adolescent. The fifth interviewer conducted only test assessments (n = 5), and the sixth interviewer conducted only retest assessments (n = 4). Five (13.5%) of the 37 adolescents did not return to participate in the retest exercise (2 males and 3 females). No mean differences were found between completers and dropouts in percentage day’s use of any illicit drugs, or when alcohol, cocaine, or marijuana use was considered separately (each measure was provided at test administration). Fisher exact tests indicated that there was no relationship between study attrition and CDIS diagnoses for alcohol or drug abuse and dependence, and that the two groups did not differ on any other CDIS axis I diagnosis. Finally, t-tests indicated that there were no mean differences by attrition status in adolescent age, highest grade completed, current GPA, annual family income, and caretaker education.
On average, 12.32 (SD = 6.01) days elapsed between the test and retest administrations (range, 7 to 41 days). No relationship was found on length of time between the two interviews by adolescent gender (t (30) = 1.74, p < .09), or on multiple measures of substance use, measured at the test administration (largest obtained correlation, r = −.25, p < .17 between days elapsed and percentage days any drug use).
Table 2 presents the test-retest sample means for selected substance use and residential/health care utilization variables collected on the Form 90. As shown, test-retest means were relatively stable. No significant mean differences were obtained on the 17 paired t-test contrasts, and measures of effect size (d) corrected for small sample bias indicated that, in absolute terms, test-retest mean differences were small. Interestingly, the largest observed differences in test-retest means (although small in absolute magnitude) were in the areas of health care utilization and residential experiences, not substance use.
TABLE 2.
Test-Retest Group Means (N = 32) on Selected Form 90 Variables: Past 90 Day Period
| Variable | Test | Retest | p | d |
|---|---|---|---|---|
| Substance Use | ||||
| Percent Days Any Substance Use | 76.83 (30.54) | 75.28 (32.46) | .54 | .05 |
| Percent Days Substance Use (except Tob) | 52.63 (34.24) | 52.22 (32.19) | .94 | .01 |
| Percent Days Substance Use (except To, Al) | 47.72 (36.51) | 45.57 (35.91) | .68 | .06 |
| Percent Days Alcohol Use (only) | 15.62 (22.14) | 15.95 (23.19) | .79 | −.01 |
| Percent Days Cocaine Use (only) | 8.24 (23.16) | 7.41 (22.21) | .36 | .04 |
| Percent Days Marijuana Use (only) | 39.70 (34.35) | 43.25 (35.16) | .60 | −.10 |
| Residential/Health Care | ||||
| Days Prescribed Medications Taken | 6.94 (22.22) | 4.81 (16.76) | .42 | .11 |
| Days Receiving Medical Treatment | .59 (1.16) | .81 (2.18) | .44 | −.13 |
| Days in Hospital | .13 (.34) | .06 (.25) | .16 | .23 |
| Total Days Residential Treatment | .13 (.34) | .50 (2.30) | .32 | −.23 |
| Days Incarcerated (jail) | 1.63 (3.71) | 2.0 (5.49) | .31 | −.08 |
| Total Days in Institutions | 1.78 (3.66) | 2.47 (5.79) | .20 | −.14 |
| Total Days Living with Caretaker | 68.22 (27.28) | 70.44 (28.81) | .62 | −.08 |
| Days Homeless | 8.63 (17.54) | 10.50 (20.04) | .17 | −.10 |
| Days Paid for Work | 9.72 (17.75) | 7.00 (12.88) | .34 | .18 |
| Days of Education | 29.53 (25.05) | 30.28 (27.45) | .85 | −.03 |
| Days Religious Attendance | 2.19 (3.99) | 3.47 (6.65) | .17 | −.23 |
Table 3 reports the intraclass and Pearson Product moment correlations between test and retest measures of substance use and health care and residential experiences. Standards to assess the reliability of instruments based upon r are available. There is less agreement, however, about the interpretation of ICCs. Cicchetti (1994) has recommended the following ranges to interpret the reliability of clinical instruments when ICCs are considered: below .40 = poor; .40 to .59 = fair; .60 to .74 = good; and .75 to 1.0 = excellent. Applying this standard, the three global measures of percentage of substance use days had good-to-excellent reliability. Two of the three measures of specific percentages of substance use days also had excellent reliability: percentage alcohol and cocaine days. In contrast, only poor-to-fair reliability was obtained on estimates of the percentage days of marijuana use.
TABLE 3.
Test-Retest Intraclass and Pearson Correlations of Substance Use and General Functioning
| Variable | Pearson Product | Intraclass |
|---|---|---|
| Substance Use | ||
| Percent Days Any Substance Use | .90 | .90 |
| Percent Days Substance Use (use1) | .65 | .64 |
| Percent Days Substance Use (use2) | .68 | .68 |
| Percent Days Alcohol Use (only) | .95 | .95 |
| Percent Days Cocaine Use (only) | .98 | .97 |
| Percent Days Marijuana Use (only) | .40 | .40 |
| Residential/Health Care | ||
| Days Prescribed Medications Taken | .76 | .73 |
| Days Receiving Medical Treatment | .71 | .59 |
| Days in Hospital | .68 | .64 |
| Total Days Residential Treatment | .54 | .16 |
| Days Incarcerated (jail) | .97 | .90 |
| Total Days in Institutions | .90 | .81 |
| Days Homeless | .93 | .92 |
| Days Paid for Work | .49 | .47 |
| Days of Education | .66 | .64 |
| Days Religious Attendance | .63 | .55 |
Post hoc analyses of the finding of poor-to-fair reliability for the measure of marijuana use began with a visual inspection of the test-retest values (see Figure 1). As shown, five paired scores indicated gross test-retest discrepancies, with the apparent pattern of significantly higher retest reporting, e.g., 4 of 5 pairs had low values at test and very high values at retest. A single interviewer was associated with 4 of these 5 discrepant pairs (3 of 4 grossly higher retest scores and the single higher test score). Assuming the presence of interviewer error or bias, we removed the four outlying cases associated with this interviewer and recalculated the measures of reliability. With the reduced set of test-retest scores (N = 28) good-to-excellent reliability was obtained on the measure of percentage of days marijuana use, r = .74 and ICC = .71.
FIGURE 1.
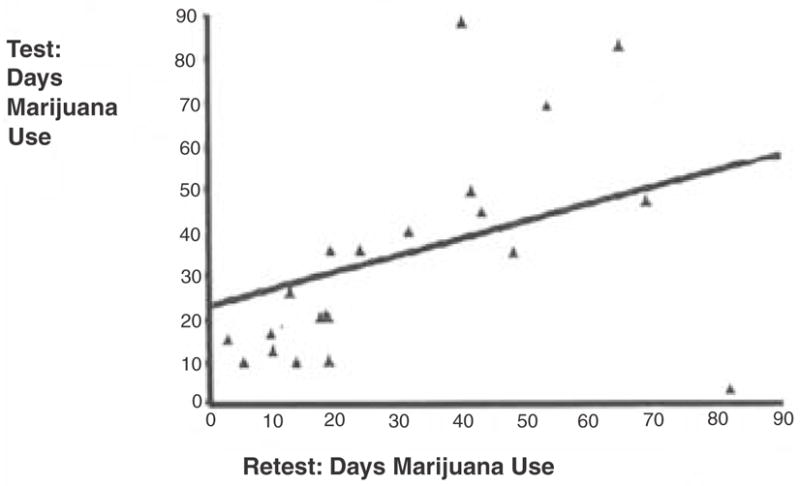
Scatterplot of Test-Retest Days Use of Marijuana N = 32
Reasonably good reliability was obtained on measures of health care utilization, especially in the context of high substance use and chaotic lifestyles. In particular, measurement of days incarcerated, total number of institutional days, and homeless days had excellent reliability according to Cicchetti’s (1994) ICC criteria. In addition, number of days of hospital care, taking of prescribed medications, and school attendance had good reliability. Fair-to-poor reliability, however, was found on four measures: days paid for work, frequency of religious attendance, days residential treatment, and days receiving medical treatment.
Convergent Validity
Pearson moment correlations were computed between four measures of substance use collected on the Form 90 and adolescent responses on the POSIT-SF and the Adolescent Drinking Index (ADI). Correlations between the substance use scale of the POSIT-SF and Form 90 measures of frequency of use of substances in general, alcohol, cocaine, and marijuana were, r = .08, r = .47, r = .42, and r = −.08, respectively. Correlations between the four Form 90 measures of frequency of substance use and three ADI scales are reported in Table 4. As displayed, the 3 ADI scales were most strongly correlated with the Form 90 frequency of alcohol use measure, a finding consistent with the exclusive alcohol focus of the ADI scales. Non-significant differences in the magnitude of correlations, however, were obtained between the 3 ADI scales and frequency of use of alcohol and cocaine. To a large extent, this finding can be explained by the high and significant correlation between alcohol and cocaine use in this sample, r = .76.
TABLE 4.
Correlations Between Four Form 90 Measures and the ADI: Convergent Validity
| Form 901 | ADI2 | ||
|---|---|---|---|
| Medical | Rebellious | Total | |
| Global Substance Use | .22 | .04 | .12 |
| Alcohol Use | .62** | .55** | .58** |
| Cocaine Use | .54** | .38* | .44* |
| Marijuana Use | .13 | .03 | .09 |
p < .05
p < .01
Form 90 variables represent number days substance used in the prior 90 day period.
ADI Medical addresses mood-altering or anxiety-reducing aspects of drinking. ADI Rebellious addresses agressive problem drinking.
DISCUSSION
By intent, this test-retest study recruited a sample that would provide a conservative estimate of the reliability of the Form 90 when administered to adolescents. Forty-six percent of youth met criteria for alcohol and drug abuse/dependence combined. Equally important, homeless youth in this sample had substantially less social structure and stability than typical substance using adolescents. Thus, the task of reconstructing day-by-day substance use and healthcare-related activities was especially challenging for this group relative to most adolescents because of the absence of memory anchors commonly used as an aid in calendar-based approaches to measuring substance use, e.g., school attendance and activities.
In spite of these challenges, most measures collected using the Form 90 were reliable in this test-retest exercise. Thus, although the Form 90 family was originally developed for treatment-seeking adults (Miller, 1995), adolescents in this study were reasonably consistent in reporting the use of global and specific substances using the day-by-day calendar approach. Especially high stability, in fact, was obtained at the group level on all variables in the substance use and health care categories (Table 2), an attractive feature to researchers conducting comparative treatment outcome studies. Specifically, none of the test-retest mean contrasts were significant in Table 2, and effect size estimates adjusted for small sample bias suggest that absolute mean differences between test and retest administrations were small to trivial.
With a few important exceptions, correlations reflecting individual test-retest stability indicated good-to-excellent reliability on the Form 90. Global measures of substance use that considered all illicit drug use and illicit drug and alcohol use combined were relatively stable across the test-retest administrations. Less consistency, however, was obtained among measures of specific drug use. On one hand, adolescents in this sample were reasonably consistent in their reported frequency of use of alcohol and cocaine for the prior 90-days. Less agreement, however, was obtained for frequency of marijuana use, with “poor” reliability demonstrated taking into account all test-retest data. With four highly discrepant cases of frequency of marijuana use excluded from the reliability analysis this measure was found to have “good” reliability, but the exact reasons for these discrepant cases being associated with a single interviewer remain unclear. It seems prudent to recommend substantial care in the use of Form 90’s measurement of marijuana use, at least in regards to homeless adolescents whose marijuana use is quite variable.
In addition to test-retest reliability, support for the convergent validity of the Form 90 was provided. Summary substance use scores (percent days of alcohol and drug use) on the Form 90 were significantly correlated with summary problem scores from both the ADI and the POSIT-SF.
Several limitations of this study should be noted. Foremost, the study included a small sample size. A larger sample would provide greater power and would decrease the potential for Type I error. Also, we did not randomize adolescents to interviewers. Related, planned counter-balancing of interviewers between test and retest administrations would have been desirable as it would have permitted more detailed analyses of interviewer effects on adolescent reported substance use. Clearly, in regards to reported use of marijuana these design features would have considerably strengthened post hoc analyses. Practical constraints such as scheduling of interviewers and not being able to anticipate when test and/or retest interviews would be conducted, however, precluded the implementation of these design features.
While additional psychometric work with a larger sample is necessary, findings in this study provide an important first step in documenting the reliability of the Form 90 with adolescents. Findings also have implications for clinical practice in demonstrating that self-reported substance use is a valid and reliability format for obtaining information on adolescent alcohol and drug use. Clinicians who seek baseline and follow up information on adolescent clients’ substance use can have confidence in the form 90 procedure for obtaining such information.
Acknowledgments
This work has been supported by NIAAA and CSAT grant (R01 AA 12173) and NIDA grant (R29 DA 11590).
References
- Beck AT, Ward C, Mendelson M, Mock J, Erlbaugh J. An inventory for measuring depression. Archives of General Psychiatry. 1961;4:53–63. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- Chamberlain R, Banerjee M, Yurek J, Creamer D, Barkett A, Pewewardy N. Juvenile Intake and Assessment Centers: Final Evaluation. Lawrence KS: Office of Social Policy Analysis, University of Kansas School of Social Welfare; 1998. [Google Scholar]
- Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Special section: normative assessment. Psychological Assessment. 1994;6:284–290. [Google Scholar]
- Danseco ER, Marques PR. Problem-Oriented Screening Instrument for Teenagers Short Form (POSIT-SF) Users Manual. Public Services Research Institute; 2000. Unpublished manuscript. [Google Scholar]
- Gilvarry E. Substance abuse in young people. Journal of Child Psychology and Psychiatry and Allied Disciplines. 2000;41:55–80. [PubMed] [Google Scholar]
- Harrell AV, Wirtz PW. Adolescent Drinking Index Test and Manual. Odessa, FL: Psychological Assessment Resources; 1989a. [Google Scholar]
- Harrell AV, Wirtz PW. Screening for adolescent problem drinking: Validation of a multidimensional instrument for case identification. Psychological Assessment. 1989b;1:61–63. [Google Scholar]
- Klitzner M, Gruenwald PJ, Taff GA, Behringer L, Harol C. The Adolescent Assessment Referral System-Final Report. National Institute on Drug Abuse; Rockville, MD: 1993. NIDA Contract No. 271-89-8252. [Google Scholar]
- Lecesse M, Waldron HB. Assessing adolescent substance use: A critique of current measurement instruments. Journal of Substance Abuse Treatment. 1994;11:553–563. doi: 10.1016/0740-5472(94)90007-8. [DOI] [PubMed] [Google Scholar]
- McLaney MA, DelBoca FK, Babor TF. A validation study of the Problem Oriented Screening Instrument for Teenagers (POSIT) Journal of Mental Health. 1994;3:363–376. [Google Scholar]
- Miller WR. Increasing motivation for change. In: Hester RK, Miller WR, editors. Handbook of Alcoholism Treatment Approaches. 2. New York: Allyn & Bacon; 1995. pp. 89–104. [Google Scholar]
- Miller WR, Marlatt GA. Manual for the Comprehensive Drinker Profile. Odessa FL: Psychological Assessment Resources; 1984. [Google Scholar]
- Miner MH. The Self-concept of homeless adolescents. Journal of Youth and Adolescence. 1991;20:545–560. doi: 10.1007/BF01540637. [DOI] [PubMed] [Google Scholar]
- Morgan CJ, Cauce AM. Predicting DSM-III-R disorders from the youth self-report: Analysis of data from a field study. Journal of the American Academy of Child and Adolescent Psychiatry. 1999;10:1237–1245. doi: 10.1097/00004583-199910000-00012. [DOI] [PubMed] [Google Scholar]
- Mundy P, Robertson M, Robertson J, Greenblatt M. The prevalence of psychotic symptoms in homeless adolescents. Journal of the American Academy of Child and Adolescent Psychiatry. 1990;29:724–731. doi: 10.1097/00004583-199009000-00008. [DOI] [PubMed] [Google Scholar]
- Norman WH, Miller IW, Klee SH. Assessment of cognitive distortion in a clinically depressed population. Cognitive Therapy and Research. 1983;7:133–140. [Google Scholar]
- Owen PL, Nyberg LR. Assessing alcohol and drug problems among adolescents: Current practices. Journal of Drug Education. 1983;13:249–254. [Google Scholar]
- Rahdert E. The adolescent assessment and referral system manual. Rockville, MD: National Institute on Drug Abuse; 1991. DHHS Publication No. (ADM) 91–1735. [Google Scholar]
- Rush AJ, Giles DE, Schlesser MA, Fulton CL, Weissenburger J, Burns C. The inventory of depressive symptomatology (IDS): Preliminary findings. Psychiatry Research. 1986;18:65–87. doi: 10.1016/0165-1781(86)90060-0. [DOI] [PubMed] [Google Scholar]
- Shaffer D. The Diagnostic Interview Schedule for Children-2.3 Version. New York: Columbia University; 1992. [Google Scholar]
- Sobell LC, Sobell MB. Timeline follow-back. In: Litten R, Allen J, editors. Measuring alcohol consumption. Totowa NJ: Humana Press; 1992. pp. 41–72. [Google Scholar]
- Tonigan JS, Miller WR, Brown JM. The reliability of Form 90: An instrument for assessing alcohol treatment outcome. Journal of Studies on Alcohol. 1997;58:358–364. doi: 10.15288/jsa.1997.58.358. [DOI] [PubMed] [Google Scholar]
- Warheit GJ, Biafora F. Mental health and Substance abuse patterns among a sample of homeless post-adolescents. International Journal of Adolescents and Youth. 1991;3:9–27. [Google Scholar]
- Westerberg VS, Tonigan JS, Miller WR. Reliability of Form 90D: An instrument for quantifying drug use. Substance Abuse. 1998;19:179–189. doi: 10.1080/08897079809511386. [DOI] [PubMed] [Google Scholar]
- Williams RJ, Chang SY. A comprehensive and comparative review of adolescent substance abuse treatment outcomes. Clinical Psychology: Science and Practice. 2000;7:138–166. [Google Scholar]
- Winters KC. The need for improved assessment of adolescent substance involvement. Journal of Drug Issues. 1990;20:487–502. [Google Scholar]
- Winters KC, Stinchfield RD. Current issues and future needs in the assessment of adolescent drug abuse. NIDA Research Monograph. 1995;156:146–171. [PubMed] [Google Scholar]