

Abstract
The cognitive model of social anxiety predicts that negative self-focused cognitions increase anxiety when anticipating social threat. To test this prediction, 36 individuals were asked to anticipate and perform a public speaking task. During anticipation, negative self-focused cognitions or relaxation were experimentally induced while self-reported anxiety, autonomic arousal (heart rate, heart rate variability, skin conductance level), and acoustic eye-blink startle response were assessed. As predicted, negative self-focused cognitions mediated the effects of trait social anxiety on self-reported anxiety and heart rate variability during negative anticipation. Furthermore, trait social anxiety predicted increased startle amplitudes. These findings support a central assumption of the cognitive model of social anxiety.
Keywords: Social Anxiety, Cognitive Mediation, Psychophysiology, Emotion Regulation, Fear of Public Speaking
1. Introduction
The cognitive model of social anxiety (Clark & Wells, 1995; Rapee & Heimberg, 1997) predicts that, when confronted with social threat, socially anxious individuals shift their attention focus inward onto negative self-focused cognitions, leading to heightened social anxiety and subsequent avoidance behaviors. There is evidence for the notion that socially anxious individuals have more negative and self-deprecating cognitions in socially threatening situations than healthy individuals (Clark & Wells, 1995; Hackmann, Clark, & McManus, 2000; Hackmann, Surawy, & Clark, 1998; Stopa & Clark, 1993). Socially anxious individuals typically monitor their internal state in the face of social threat, leading to increased self-reported anxiety (Hofmann & Barlow, 2002; Spurr & Stopa, 2002; Woody, 1996). Successful treatment is associated with decreased self-focused attention (Hofmann, 2000; Wells & Papageorgiou, 1998; Woody, Chambless, & Glass, 1997), which is correlated with changes in social anxiety, especially among individuals who receive cognitive behavioral interventions (Hofmann, Moscovitch, Kim, & Taylor, 2004). When healthy individuals anticipate a public speaking task with a thought protocol imitating the cognitive style of socially anxious individuals, the participants’ self-reported anxiety is comparable to that of high socially anxious individuals (Hinrichsen & Clark, 2003; Vassilopoulos, 2005). It has further been shown that the estimated cost of social mishaps partially mediates therapy success (Hofmann, 2004). This is consistent with cross-sectional studies suggesting that cognitive variables, such as self-focused attention (Kashdan & Roberts, 2004), perception of emotional control (Hofmann, 2005), and evaluation of one’s own performance (Perini, Abbott, & Rapee, 2006), are causally related to social anxiety. Nevertheless, no study has demonstrated experimentally that anxiety in anticipation of a socially threatening situation is cognitively mediated - one of the core assumptions of the cognitive model. As a result, some authors have recently questioned the cognitive mediation model of social anxiety (e.g. Longmore & Worrell, 2007).
To examine whether cognitions mediate social anxiety, which is an important prediction of the cognitive model, we assessed anxious responding during anticipation of public speaking, the most commonly feared social situation by socially anxious individuals and the general population (Mannuzza, Schneier, Chapman, & Liebowitz, 1995; Pollard & Henderson, 1988). We expected that trait social anxiety would predict increases of acute social anxiety in response to this situation. To examine the role of cognitions as a mediator, we induced negative self-focused cognitions with a script developed by Hinrichsen and Clark (2003) and compared this to relaxation instructions that encourage participants to focus their attention away from negative cognitions (Hudetz, Hudetz, & Reddy, 2004)1. Therefore, we expected greater anxiety and negative cognitions during negative anticipation than during baseline and relaxed anticipation. Moreover, we expected that task induced changes would be mediated by corresponding differences in the amount of negative cognitions.
In addition to self-report measures, we examined physiological correlates of trait social anxiety (Dewar & Stravynski, 2001; Hofmann, Heinrichs, & Moscovitch, 2004). Heart rate variability in the high frequency spectrum (HRV-HF, Camm et al., 1996) is a commonly used index of respiratory sinus arrhythmia and primarily reflects parasympathetic influence on heart rate (see Grossman & Taylor, 2007, for a discussion of interpretative issues and further influencing factors). Between-subjects differences have been associated with emotional reactivity (Thayer & Brosschot, 2005; Beauchaine, 2001) and acute shifts of HRV-HF have been linked to self-regulatory efforts of emotional responding (Porges, 1995; Thayer & Lane, 2000; Beauchaine, 2001). Therefore, we expected an inverse relationship of between-subjects’ levels of HRV-HF, and the level of anxiety as well as the amount of negative cognitions while anticipating public speaking. Furthermore, we expected that higher levels of trait social-anxiety would predict stronger task induced within-individual decrease of HRV-HF. Moreover, we expected that this contingency would be mediated by negative cognition. In addition, we used the startle paradigm to probe the activation of avoidance tendencies by affective information processing, (Vrana, Spence, & Lang, 1988; Bradley, Codispoti, & Lang, 2006), assessed skin conductance level as an index of distress related sympathetic arousal (e.g. Boucsein, 1992), and heart rate as a general indicator of physiological activation. In line with previous reports (e.g. Mauss, Wilhelm, & Gross, 2004), we expected general stress-related activation in SCL and HR in anticipation of public speaking, but no association with trait social anxiety. For startle amplitude, we expected similar effects as for self-reported anxiety.
2. Method
2.1 Participants
We recruited 36 undergraduate students at Boston University with a wide range of trait social anxiety (M = 54.48, SD = 23.79, Min = 8.80, Max = 99.32) as measured with the social phobia subscale of the Social Phobia and Anxiety Inventory (SPAI: Turner, Beidel, Dancu, & Stanley, 1989), a well established self-report measure of trait social anxiety with excellent psychometric properties (Turner, Stanley, Beidel, & Bond, 1989). The internal consistency of the SPAI social phobia subscale in the current sample was .96. Overall, our sample was comparable to unselected representative student samples (e.g. Turner, Beidel, Dancu, & Stanley, 1989). Four (11 %) participants scored above 80, a cutoff commonly used as an indicator of probable presence of social anxiety disorder. We found no significant gender difference (male vs. female: M = 46.68 vs. 58.90; SD = 5.87 vs. 5.11; t(34) = 1.51, p < .14, d = .5).
To examine if the effects were specifically related to trait social anxiety, we also measured general trait anxiety with the Spielberger State Trait Anxiety Inventory (M = 51.53, SD = 3.60, Min = 44, Max = 59, STAI-trait: Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983). Most participants were female (n = 23, 63.89 %) and Caucasian (n = 26, 72.22 %). Non-Caucasian participants identified themselves as Asian (n = 3, 8.33 %), Indian (n = 2, 5.56 %), Hispanic (n = 2, 5.56 %), or other (n = 3, 8.33 %). The average age was 18.83 (SD = .94), and all participants were unmarried (n = 36, 100 %). There were no significant differences in SPAI and STAI-trait scores, age, or ethnic origin between the two groups randomized to different Task-Order (negative before relaxed anticipation, or vice versa, all p’s > .74), or between men and women (all p’s > .07).
2.2 State Measures
We used the Self-Statements During Public Speaking Scale (SSPS: Hofmann & DiBartolo, 2000) to measure cognitions during the preparation for the participants’ speeches. The SSPS was developed to assess self-focused cognitions.
We specifically used the negative subscale (SSPS-N), because it mediates treatment change in social phobia (Hofmann, Moscovitch, Kim, & Taylor, 2004), and is associated with low expectations for success and low satisfaction in a performance situation, and high self-reported anxiety in a public speaking task (Hofmann & DiBartolo, 2000). Each scale of the SSPS comprises five statements describing feelings and thoughts subjects might have about themselves in public speaking situations. Examples of negative subscale items include: “A failure in this situation would be more proof of my incapacity”, and “What I say will probably sound stupid”. The SSPS has excellent psychometric properties, and is sensitive to change (Hofmann & DiBartolo, 2000). In the current sample, the internal consistency of the SSPS-N was .80 and .81 in the negative and relaxed anticipation conditions, respectively.
Self-reported anxiety was assessed via ratings using the following statement presented on a computer screen: “How anxious do you feel at the moment?” Participants rated their anxiety on a scale from 0 (no anxiety) to 100 (strongest feeling of anxiety that you can imagine). The reliability of the averaged repeated measurements was r = .81, and r = .78 within the negative and relaxed anticipation conditions, respectively.
2.3 Psychophysiological Measures
All psychophysiological measures were recorded with a BIOPAC MP150 system at a sampling rate of 1000 Hz. One electrode (Ag-AgCl, 8 mm) on the left clavicle served as common ground. Two electrodes (Ag-AgCl, 8 mm, on right clavicle and lower left rib cage) were used to record an electrocardiogram (EKG; analog high-pass filter: 0.5 Hz). R-spike detection, screening for artifacts and interpolation of ectopic beats, and computation of the average heart rate (HR [bpm]) was done with Matlab. The RR-interval time series was prorated to equal time intervals (8 Hz) and de-trended to remove tonic shifts of sympathetic activation (10 s high-pass filter period). Finally, mean spectral power density of heart-rate-variability in the high frequency range of 0.15–0.40 Hz (HRV-HF [ms2], see Camm et al., 1996) was derived with discrete Fourier transform (DFT; 64 s Hanning window, 50% overlap). Skin conductance level (SCL [µS]; analog low-pass filter: 10 Hz) was recorded via two electrodes (Ag-AgCl, 8 mm) on the second phalanx of index and ring finger of the non-dominant hand. For the statistical analysis we averaged HR, HRV-HF, and SCL, derived from six a priori determined 2-min epochs within each anticipatory condition. By restricting the measurement to these epochs of quiet sitting, we tried to maximize reliability and minimize artifacts and uncontrolled influences by movement or postural and respiratory variations. While such influences are problematic in general, HRV is particularly susceptible to them (Grossman & Taylor, 2007). To further avoid uncontrolled differential effects between single variables, we used the same measuring intervals for all physiological variables. To maximize comparability across response domains, each recording was followed by a rating of self-reported anxiety, which were also combined into mean scores for each anticipatory condition.
The electromyogramm (EMG [µV]) of the eye blink response to binaural presentations of 50 ms bursts of white noise (instantaneous rise-time) calibrated at 105 dB (A) over Etymotic ER•6 Isolator in ear headphones, was recorded via two sanitized reusable electrodes (Ag-AgCl, 4 mm). Skin preparation, electrode placement, and analysis followed the recommendations of Blumenthal et al. (2005). The raw EMG was filtered (60 Hz notch, 20 Hz 4th order Butterworth high-pass), rectified, and smoothed (100 ms moving average). Next, scoring of the amplitude of the startle-blink reactions was performed with EMGpeakfind (Schulz & Alpers, 2007), a semi-automatic program for Matlab. Startle amplitudes were computed by subtracting the average of 20 ms of data before startle-onset (EMG-baselines) from startle magnitudes. Amplitudes equal or smaller than zero and reactions with artifacts were excluded from the analysis (15.97 %). There were no startle non-responders (Blumenthal et al., 2005).
Mean startle amplitudes were square-root transformed, and mean HRV-HF was log10 transformed to achieve normal data distribution across subjects. Finally, all data were screened according to the recommendations by Tabachnick and Fidell (2007). Outliers in HRV-HF data were deleted from baseline in one participant, and in the negative anticipation condition from another participant.
2.4 Procedure
Experimental Procedure
After signed informed consent was obtained, all participants were asked for their initial ratings of self-reported anxiety, and to fill out the STAI-trait, SPAI and a socio-demographics form. Next, the participants were seated in the experimental room 40 cm in front of a 17”-Monitor, which was used for presenting instructions and visual stimuli. After that, the electrodes for the psychophysiological measurement were attached. After a 2-min baseline of the physiological measures was recorded, the participants were randomly assigned to one of two anticipation conditions:
In the negative anticipation condition we induced negative self-focused cognitions with a script developed by Hinrichsen and Clark (2003, p. 213). Written instructions prompted participants to remember particular social situations that did not go well, to imagine how they appeared in this situation, and what impression this may have created in others. Based on this past image, participants were asked to anticipate how they might perform in the upcoming speech, what could go wrong, what would be the worst thing that could happen, and what would happen if they made a fool out of themselves. This procedure was repeated with additional situations, for the duration of the anticipatory period.
In the relaxed anticipation condition (Hudetz, Hudetz, & Reddy, 2004), participants listened to a pre-recorded tape instructing them to close their eyes, and focus on pleasant thoughts, feelings, and images, and to let go of any negative cognitions that came to mind. The relaxation instructions included statements such as “tension flows from my body” and ”I can relax at will”. This was accompanied by relaxing music and the sound of ocean waves.
Following the 2-min recordings of physiological data, self-reported anxiety was assessed after 2, 8, 10, 29, 35, and 37 min of anticipation respectively. In addition, anticipation was interrupted twice (after 12 and 39 min) by a 15-min startle procedure. Following 55 min of anticipation, two confederates entered the room as an audience. Next, participants were asked to fill out the SSPS, a camera for recording the speech was uncovered and turned on, and the participants were asked to speak for at least 3 min about personal strengths and weaknesses as part of an imaginary job application. In addition, the audience evaluated the speech on a rating chart. Then, the complete procedure (anticipation, startle procedures, and another speech) was repeated with the other anticipatory protocol (negative vs. relaxed). Finally, all participants rated how pleasant they experienced the relaxed and how unpleasant they experienced the negative anticipation condition (0 = not at all; 6 = extremely), and were debriefed.
Startle Procedure
Participants wore headphones throughout the anticipation periods. At the beginning of each startle procedure four startle reactions were elicited while the screen was still blank. The first two reactions were omitted from the analysis. Next, participants were asked to direct their attention to 21 stimuli randomly drawn from 7 categories with differing threat potential (emotional words, facial expressions, and houses). Each stimulus was preceded by a 250 ms fixation cross, and followed by a 15 s (± 5 s) inter-stimulus-interval (blank screen).Startle reactions were elicited during two out of three stimulus presentations per category. Because the results were essentially the same with all stimulus categories, we will only report the analyses of the square-root transforms of the overall mean of the startle amplitude.
2.5 Statistical Analysis
We used repeated measures ANOVAs (within-subjects factor Task: baseline, negative anticipation, relaxed anticipation, between-subjects factor Task-Order: negative before relaxed anticipation, or vice versa) and planned contrasts, as well as independent t-tests (two-tailed) to examine effects of the experimental manipulation, and possible effects of the within-subjects design such as habituation.2 For tests on autonomic physiological activation, we also entered the dependent variables HR, SCL, and log10 transforms of HRV-HF simultaneously in a MANOVA (within-subjects factor Task: baseline, negative anticipation, relaxed anticipation, between-subjects factor Task-Order: negative before relaxed anticipation, or vice versa), because measures within this response domain are not independent. Greenhouse-Geisser statistics are reported, when sphericity could not be assumed.
Furthermore, we used linear regressions to examine if trait social anxiety (SPAI) specifically predicted anxious responding and also applied Baron and Kenny’s (1986) stepwise procedure to test the proposed mediation hypothesis. The criteria for mediation are as follows: In the first step, the predictor variable has to be correlated with the outcome (path c, the total effect). Second, the predictor variable has to correlate with the mediator (path a). Third, the mediator has to affect the outcome variable (path b), while the influence of the predictor variable is controlled. Fourth, full mediation is present if the relationship between predictor and outcome variable, while controlling for the effect of the mediator, is zero (path c’, the direct effect). Otherwise, there is only partial mediation. In addition, we computed Sobel’s (1982) significance test to assess the indirect effect (path ab) of the predictor on the outcome variable through the mediator. Sobel’s test can be interpreted as an index of the strength of mediation. In two mediation models, we examined if negative cognition (SSPS-N) mediated the relationship between trait social anxiety (SPAI) and effects of anticipation on self-reported anxiety and log10 transforms of HRV-HF. For these analyses, we computed baseline corrected difference scores reflecting the increase of self-reported anxiety and the decrease of HRV-HF during negative anticipation. In a third model, we investigated cognitive mediation of the square-root transformed startle amplitudes. Because startle amplitudes were not assessed at baseline, we used uncorrected scores.
3. Results
3.1 Manipulation Check
After the experiment, relaxed anticipation was rated as moderately pleasant (M = 4.17, SD = 1.20), while negative anticipation was rated as moderately unpleasant, M = 3.31, SD = 1.49, t(34) = 3.51, p < .001, d = .78. In addition, negative cognitions (SSPS-N) were significantly enhanced during negative anticipation in comparison to relaxed anticipation, as indicated by a significant main effect Task, F(1, 33) = 10.54, p < .01, partial-η2 = .24 (Table 1). There was no main effect Task-Order, differentiating the two groups either randomized to negative before relaxed anticipation, or vice versa (F(1, 33) = 10.54, p < .01, partial-η2 = .24), and there was no Task by Task-Order interaction, F(1, 33) < 1.
Table 1.
Means and standard deviations for self-report measures (self-reported anxiety [ratings from 0 to 100], negative cognitions [SSPS-N scores from 0 to 10]), autonomic measures (skin conductance level [SCL, µSi], heart rate [HR, bpm], log10-transforms of heart rate variability in the HF-range [HRV-HF, ms2]), and startle eye-blink (square-root transforms of the amplitude [µV]), at baseline, and during negative and relaxed anticipation of public speaking.
| Measures by Response Domain | Baseline | Negative Anticipation | Relaxed Anticipation |
|---|---|---|---|
| M (SD) | M (SD) | M (SD) | |
| Self-Report Measures | |||
| Self-Reported | 24.29 (20.06) | 32.98 (22.90) | 19.71 (15.70) |
| Anxiety | |||
| SSPS-N | -- | 9.43 (5.15) | 7.31 (5.05) |
| Autonomic Measures | |||
| SCL | 17.10 (7.80) | 20.24 (7.90) | 19.20 (6.98) |
| HR | 77.07 (15.43) | 80.91 (13.82) | 80.02 (14.17) |
| HRV-HF | 3.04 (.68) | 2.83 (.60) | 2.94 (.60) |
| Startle Eye-Blink | |||
| Startle | -- | .50 (.29) | .54 (.27) |
| Amplitude |
3.2 Effects of Experimental Manipulation
Self-Reported Anxiety
The anticipatory tasks affected self-reported anxiety as suggested by the significant Task effect, F(2, 66) = 7.78, p < .001, partial-η2 = .19. Planned contrasts showed that self-reported anxiety was significantly elevated during negative anticipation (F(1, 33) = 5.31, p < .03, partial-η2 = .14), but not during relaxed anticipation (F(1, 33) = 1.61, p < .21, partial-η2 = .05), when compared to baseline (Table 1). The direct comparison between negative and relaxed anticipation was significant, F(1, 33) = 23.29, p < .001, partial-η2 = .41. There was no main effect differentiating the two groups randomized to different Task-Order, F(1, 33) < 1. The Task by Task-Order interaction was marginally significant, F(2, 66) = 2.43, p < .10, partial-η2 = .07. Contrast computations revealed that self-reported anxiety decreased significantly from the first (M = 29.77, SD = 23.01) to the second anticipation (M = 22.91, SD = 17.54), as indicated by a significant Task by Task-Order interaction, F(1, 33) = 5.72, p < .02, partial-η2 = .15.
Autonomic Measures
A multivariate test using the Pillay-Spur criterion with measures of autonomic physiological activation as dependent variables (SCL, HR, and log10 transforms of HRV-HF) showed a significant main effect Task, F(6, 27) = 3.09, p < .02, partial-η2 = .41. There was no significant difference between the two groups randomized to different Task-Order, F(3, 30) = 1.18, p < .34, partial-η2 = .11. However, there was a significant Task by Task-Order interaction, F(6, 27) = 3.23, p < .02, partial-η2 = .42. This multivariate test was followed up with univariate analyses and planned contrasts to examine task-effects in each dependent measure.
The Task effect was significant for SCL (F(1.53, 51.94) = 4.92, p < .01, partial-η2 = .13), and planned contrasts showed that SCL was elevated during both negative (F(1, 34) = 6.16, p < .02, partial-η2 = .15), and relaxed anticipation (F(1, 34) = 5.55, p < .02, partial-η2 = .14), in comparison to baseline (Table 1). There was no significant difference between negative and relaxed anticipation, F(1, 34) = 1.68, p < .20, partial-η2 = .05. The two groups randomized to different Task-Order were not significantly different (F(1, 34) < 1), and there was no Task by Task-Order interaction, F(1.53, 51.94) = 1.75, p < .19, partial-η2 = .05.
Similarly, the Task effect was significant for HR (F(2, 68) = 9.75, p < .001, partial-η2 = .22), and planned contrasts showed that HR was significantly higher during both negative (F(1, 34) = 15.38, p < .001, partial-η2 = .31), and relaxed anticipation (F(1, 34) = 9.05, p < .01, partial-η2 = .21) in comparison to baseline. There was no significant difference between negative and relaxed anticipation, F(1, 34) = 1.13, p < .30, partial-η2 = .03. The two groups randomized to different Task-Order were not significantly different, F(1, 34) = 2.34, p < .14, partial-η2 = .07. However, there was a significant Task by Task-Order interaction, F(2, 68) = 4.27, p < .02, partial-η2 = .11. Contrast computations revealed that self-reported anxiety decreased significantly from the first (M = 81.68, SD = 13.96) to the second anticipation (M = 79.25, SD = 13.95), as indicated by a significant Task by Task-Order interaction, F(1, 34) = 11.17, p < .01, partial-η2 = .25.
Finally, we found a significant Task effect for log10 transformed HRV-HF, F(1.51, 48.41) = 7.10, p < .01, partial-η2 = .18. Planned contrasts showed that HRV-HF was significantly decreased during negative anticipation (F(1, 32) = 9.58, p < .01, partial-η2 = .23), and marginally significantly decreased during relaxed anticipation (F(1, 32) = 3.27, p < .08, partial-η2 = .09), when compared to baseline. Consequently, HRV-HF was significantly lower during negative than during relaxed anticipation, F(1, 32) = 7.44, p < .01, partial-η2 = .19. A marginally significant main effect Task-Order indicated that HRV-HF was generally higher in the group beginning with negative anticipation, F(1, 32) = 3.60, p < .07, partial-η2 = .10. There was no Task by Task-Order interaction, F(1.51, 48.41) < 1.
Startle Eye-Blink
There was no significant difference between square-root transforms of startle amplitude during negative and relaxed anticipation, F(1, 33) =1.35, p < .25, partial-η2 = .04 (Table 1). There was no difference between the two groups randomized to different Task-Order (F(1, 33) = 1.73, p < .20, partial-η2 = .05), but a significant Task by Task-Order interaction (F(1, 33) = 23.26, p < .001, partial-η2 = .41), suggesting a significant decrease of startle amplitude from the first (M = .60, SD = .30) to the second anticipation (M = .44, SD = .23).
3.4 Mediation Analyses
Trait social anxiety specifically predicted the amount of negative cognitions (SSPS-N), self-reported anxiety, and square-root transformed startle-amplitude3 during both negative and relaxed anticipation, but not at baseline (Table 2). In contrast, trait social anxiety, and general trait anxiety (R2 = .15, β =−.39, t(1, 34) = −2.41, p < .02) predicted log10 transformed HRV-HF at baseline. Finally, HR and SCL were neither related to trait social anxiety nor to general trait anxiety.
Table 2.
Parameters for separate linear regression analyses of criteria (self-reported anxiety, negative cognitions [SSPS-N], skin conductance level [SCL], heart rate [HR], log10-transforms of heart rate variability in the HF-range [HRV-HF], square-root transforms of startle eye-blink amplitude) on predictor trait social anxiety (SPAI) at baseline, and during negative and relaxed anticipation of public speaking
| Measures by Response Domain | Baseline | Negative Anticipation | Relaxed Anticipation |
|---|---|---|---|
| R2, β | R2, β | R2, β | |
| t (df) | t (df) | t (df) | |
| Self-Report Measures | |||
| Self-Reported | .11, .33, | .42, .65, | .18, .43, |
| Anxiety | 1.99 (1,33) | 4.91 (1,33)*** | 2.67 (1,33)** |
| SSPS-N | -- | .57, .76, | .28, .53, |
| 6.65 (1,33)*** | 3.63 (1,34)*** | ||
| Autonomic Measures | |||
| SCL | .05, .21, | .02, .13, | .03, .16, |
| 1.28 (1,34) | .76 (1,34) | .96 (1,34) | |
| HR | .01, −.08, | .01, −.02, | .01, −.03, |
| −.46 (1,34) | −.14 (1,34) | −.17 (1,34) | |
| HRV-HF | .13, .36, | .01, .08, | .07, .27, |
| 2.24 (1,33)* | .47 (1,33) | 1.60 (1,32) | |
| Startle Eye-Blink | |||
| Startle | -- | .20, .45, | .24, .49, |
| Amplitude | 2.95 (1,34)** | 3.19 (1,33)** |
p < .05
p < .01
p < .001.
In two mediation models, we examined if negative cognition (SSPS-N) mediated the relationship between trait social anxiety (SPAI) and effects of anticipation on self-reported anxiety and log10 transformed HRV-HF (Figure 1). Step 1 of Baron and Kenny’s (1986) procedure showed that trait social anxiety predicted the increase of self-reported anxiety (R2 = .13, β = .36, t(1, 33) = 2.21, p < .03), and the decrease of HRV-HF (R2 = .24, β = −.50, t(1, 33) = −3.25, p < .01) from baseline to negative anticipation (path c in Figure 1 A and B). In addition, we confirmed specificity of this effect with an analogous analysis with predictor SPAI-trait (all t’s < 1.98). Step 2 (path a in Figure 1 A and B) was established for both mediation models: trait-social anxiety (SPAI) predicted the amount of negative cognitions (SSPS-N) during negative anticipation, R2 = .57, β = .76, t(1, 33) = 6.65, p < .001. Step 3 (path b in Figure 1 A and B) confirmed that negative anticipatory cognitions (SSPS-N) mediated the relationship between trait-social anxiety (SPAI) and the increase of self-reported anxiety from baseline to negative anticipation (R2 = .24, β = .50, t(2, 31) = 1.09, p < .05) as well as the decrease of HRV-HF from baseline to negative anticipation, R2 = .35, β = −.49, t(2, 31) = −2.20, p < .04. Full mediation was shown by Step 4 (path c’ in Figure 1 A and B), which confirmed that the direct effect of trait social anxiety on the outcome variables, while controlling for the effect of the mediator, was no longer significant (self-reported anxiety: R2 = .24, β = −.01, t(2, 31) = −.02, p < .99; HRV-HF: R2 = .35, β = −.13, t(2, 31) = −.58, p < .57). This was corroborated by significant indirect effects (self-reported anxiety: 0.36; Sobel z-value = 1.99, p < .05; HRV-HF: −0.37; Sobel z-value = −2.12, p < .03).
Figure 1.
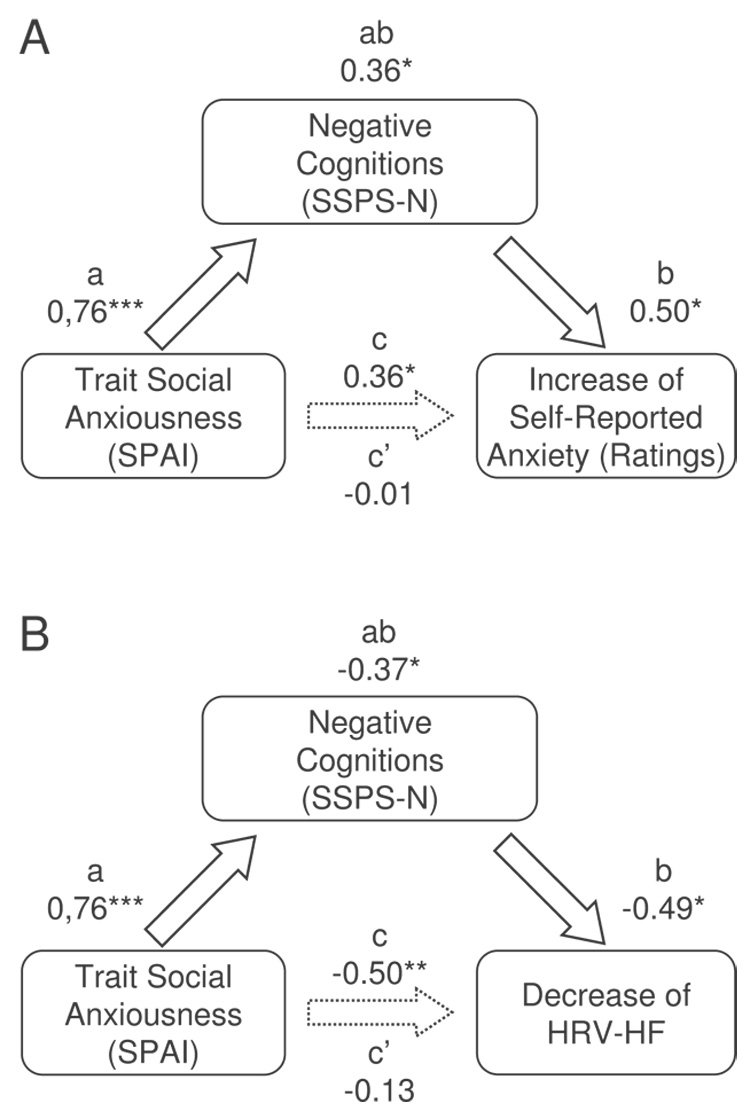
Results of the hypothesized mediation models: A) negative cognitions (SSPS-N) as a mediator between trait social anxiety (SPAI) and increases of self-reported anxiety from baseline to negative anticipation; B) negative cognitions (SSPS-N) as a mediator between trait social anxiety (SPAI) and decreases of log10-transforms of heart rate variability in the HF-range (HRVHF) from baseline to negative anticipation; standardized regression coefficients, * p < .05, ** p < .01, *** p < .001.
In a third model, we investigated cognitive mediation of square-root transformed startle amplitudes. As reported above, trait-social anxiety (SPAI) predicted startle amplitude during both, negative and relaxed anticipation. Hence requirements of Step 1 in Baron and Kenny’s (1986) procedure were met. In Step 2, it was shown that trait-social anxiety predicted the amount of negative cognitions (SSPS-N) not only during negative but also relaxed anticipation, R2 = .53, β = .53, t(1, 34) = 3.63, p < .001. However, in Step 3 of Baron and Kenny’s (1986) procedure, negative cognitions were not predictive of startle amplitude during negative (R2 = .20, β = −.01, t(2, 32) = .02, p < .98) or relaxed anticipation, R2 = .30, β = .30, t(2, 32) = 1.71, p = .10. Finally, Step 4 showed that marginally significant effects of trait social anxiety persisted while controlling for the effect of negative cognition during negative (R2 = .20, β = .46, t(2, 32) = 1.89, p < .07) and relaxed anticipation, R2 = .30, β = .33, t(2, 32) = 1.94, p < .06.
We further explored correlations of startle amplitude with other measures. We found significant correlations with negative cognitions (SSPS-N) during both negative (r2 = .34, p < .05) and relaxed anticipation (r2 = .47, p < .01), and with self-reported anxiety during negative anticipation only, r2 = .40, p < .02.
4. Discussion
In the present study, we investigated a core assumption of the cognitive model of social anxiety (Clark & Wells, 1995; Rapee & Heimberg, 1997), namely, that negative self-focused cognitions mediate the relationship between trait social anxiety and anxious responding during anticipation of a socially threatening situation (i.e. public speaking). Our results support our main hypothesis. Consistent with previous reports (Hinrichsen & Clark, 2003; Vassilopoulos, 2005), self-reported anxiety increased significantly from baseline to anticipation of public speaking, when participants engaged in negative self-focused cognitions. Furthermore, self-reported anxiety but not general trait anxiety predicted higher intensity of negative cognition (SSPS-N) and self-reported anxiety. The mediation analyses with the procedures described in Baron and Kenny (1986), and Sobel (1982) revealed, that this heightened anxiety response was fully mediated by the amount of negative self-focused cognitions during anticipation (SSPS-N). This supports an important predication of the cognitive model. As expected, the participants had significantly reduced negative cognitions during relaxed anticipation. Greater trait social anxiety predicted both higher intensity of negative cognitions (SSPS-N) and higher self-reported anxiety during relaxed anticipation. This finding suggests an interaction between trait social anxiety and situational context, regardless of the nature of the anticipatory task. However, self-reported anxiety did not increase significantly from baseline during relaxed anticipation. This finding shows that manipulating anticipatory cognitions successfully affected the emergence of anticipatory anxiety.
We specifically encouraged participants to assess their feelings when rating self-reported anxiety, as opposed to assessing their cognitions (SSPS-N). Although these are standard methods to measure emotional response and cognitions, these measures may be subject to rater biases such as a halo effect. However, the physiological measures are unlikely to be affected by these biases. Interestingly, the results of HRV-HF mirror the findings of self-reported anxiety when examining task-induced changes from baseline. Increased self-reported anxiety during negative anticipation was matched by a significant decrease of HRV-HF. Moreover, higher levels of trait social anxiety predicted stronger decrease of HRV-HF. This relationship was fully mediated by negative self-focused cognitions (SSPS-N). Although there was also a significant decrease of HRV-HF in the relaxed anticipation condition, it was significantly smaller. A positive correlation between general trait anxiety and baseline HRV-HF suggests a general deficiency in emotional reactivity to situational demands (Beauchaine, 2001; Thayer & Brosschot, 2005). At the same time, there was a positive correlation between baseline HRV-HF and trait social anxiety, suggesting flexibility of emotional reactivity in socially anxious individuals. During anticipation of public speaking, this relationship reversed. In line with our hypothesis, trait social anxiety predicted a deficient parasympathetic regulatory response to anticipation of public speaking, which was especially pronounced during negative anticipation. Taken together, these findings suggest that the effect hinges on a triple interaction of trait, situational context, and cognition, which is perfectly in line with the DSM-IV definition of social anxiety disorder (APA, 2000). Consistent with previous results (Mauss, Wilhelm, & Gross, 2004), further evidence for physiological correlates of social anxiety was limited. HR and SCL increased from baseline to both negative and relaxed anticipation. HR and SCL were not correlated with trait social anxiety or general trait anxiety. First, this suggests that all participants were activated and had increased sympathetic arousal in anticipation of public speaking. Second, it further underlines the specific association of parasympathetic reactivity and social anxiety. Interestingly, longitudinal studies have linked low heart period variability in response to cognitive stressors to behavioral inhibition in infants and children (Kagan, Reznick, & Snidman, 1987), a predictor of later development of social anxiety disorder (Hayward, Killen, Kraemer, & Taylor, 1998). In adults, HRV-HF decreases in response to situational demands were associated with deficiencies in emotional regulation (Thayer & Lane, 2000). However, in contrast to these studies, we primarily found a deficient parasympathetic response, rather than sympathetic dis-inhibition by parasympathetic feed-forward loops. Notably, other studies have also failed to show sympathetic hyperarousability in socially anxious individuals (Brown, Chorpita, & Barlow, 1998; Mauss, Wilhelm, & Gross, 2004 ). Taken together, this offers an interesting objective for future studies on correlates of emotion regulation as potential precursors in the etiology of the negative cognitive style associated with social phobia. In this pursuit it will be important to disambiguate the relative contribution of sympathetic vs. parasympathetic reactivity in response to social threat.
Similar to previous results (Panayiotou & Vrana, 1998) trait social anxiety predicted increased startle amplitude in our sample. In the negative anticipation condition, startle amplitude correlated with self-reported anxiety. Furthermore, there were no correlations with HR, or SCL. These findings parallel effects found for self-reported anxiety, and HRV-HF. However, startle amplitude was not different in the relaxed vs. negative anticipation condition, and startle response was not mediated by cognition. Lack of startle measurements at baseline complicates the interpretation of these results. However, Cornwell, Johnson, Berardi, & Grillon (2006) found similar positive correlations between startle amplitude and fear of negative evaluation not only during anticipation of public speaking in a virtual reality task (r = .46) but also during baseline (r = .40). Therefore, our results could indicate a general vulnerability of affective information processing rather than an effect or by-product of acute social anxiety. As briefly mentioned, this finding seems to be independent of the content of mild emotional foreground stimuli.
The study shows a number of limitations. First, we only considered negative self-focused cognitions as a potential mediator of social anxiety. Other potential mediators such as estimated social cost (Hofmann, 2004), may be even more specific to social anxiety. Second, Task-Order by Task interactions indicated a general decrease in all measures except SCL, and HRV-HF from the first to the second anticipation of public speaking. Although one might expect that depending on the first task different carry over effects to the second anticipation might occur, or that post processing of the first speech might affect the second anticipation period, these effects were principally consistent. In addition, the two groups randomized to different Task-Order were largely equivalent. Therefore, the most parsimonious interpretation is habituation or a reduction of overall arousal due to reduced uncertainty about the procedure in the second task. Although such effects should be further explored in future studies, we found no indication that this compromised our main results. Third, HRV-HF is only a reliable indicator of parasympathetic activation when assessed under controlled conditions. We addressed this issue by using only data uncompromised by known sources of artifact. Furthermore, measuring shifts of HRV-HF is more reliable than baseline assessment of vagal tone (e.g. Grossman & Taylor, 2007). However, we cannot rule out that faster breathing may have inflated HRV-HF decreases (Camm et al., 1996). Therefore, future studies should examine possible effects of respiration. Fourth, although some studies have suggested that gender might be an important factor in social anxiety disorder, we found only minor differences between men and women, unrelated to social anxiety. However, gender effects may be stronger in individuals with a clinical diagnosis of social anxiety disorder. Finally, we used an experimental manipulation to encourage or discourage participants from engaging in negative thinking. Under the assumption that all other conditions were held constant between the two anticipatory conditions, our findings suggest that cognitions cause changes in self-reported anxiety and psychophysiology. Although other variables may be involved in this effect, this finding implies a functional role of this mediator. However, such claims of causality remain to be tested in future studies with appropriate models and experiment designs (e.g. Steyer, 1992).
Despite these limitations, our results support the notion that negative self-focused cognitions mediate the effects of trait social anxiety on subjective and psychophysiological correlates of social anxiety when anticipating social threat. This supports a primary assumption of the cognitive model (Clark & Wells, 1995; Rapee & Heimberg, 1997). The effects on heart rate variability (HRV-HF) further point to dysfunctional emotion regulation as an important element of social anxiety.
Acknowledgements
This work was funded in part by NIMH grant MHMH075889 (Stefan G. Hofmann), and a scholarship by the Gottlieb Daimler- and Karl Benz-Foundation (Stefan M. Schulz), Germany, and by the Research Group Emotion and Behavior which is sponsored by the German Research Society (DFG) (Georg W. Alpers). It was conducted as part of S. M. Schulz’s doctoral dissertation at the Department of Psychology, University of Würzburg. Dr. Hofmann is a paid consultant by Organon (Schering-Plough) for issues and projects unrelated to this study. We thank Dr. Paul Pauli for his input and Dr. Alexander Gerlach for providing his tools for physiological data analysis, and Chih-Fang Hsieh, Gezim Begolli, Andrew Camp, Nick Carde, Mica Brosbe, Delia Aneacsiu, and Nikola Stenzel for their assistance.
Correspondence concerning this article should be address to PD Dr. Georg W. Alpers, University of Würzburg, Department of Psychology, Marcusstrasse 9-11, 97070 Würzburg, Germany, Email: alpers@psychologie.uni-wuerzburg.de, Phone: +49-931-312840, Fax: +49-931-312733.
Footnotes
We consider this to be a better control condition than anticipation without a task, because it actively counteracts the default reaction of socially anxious individuals to focus their attention on negative self-related cognitions when anticipating social threat.
In an alternative analysis with gender added as another factor, all reported effects remained unaffected. Marginally significant effects of gender suggested lower baseline HR (F(1,32) = 3.95, p < .06, partial-η2 = .11) and SCL (F(1,32) = 3.36, p < .08, partial-η2 = .10) in men (HR: M = 75.65, SD = 14.73; SCL: M = 14.62, SD = 9.27) as compared to women (HR: M = 77.87; SD = 16.08; SCL: M = 18.51, SD = 6.64). Furthermore, there were marginally significant interactions with Task-Order, suggesting lower self-reported anxiety (F(1,31) = 5.70, p < .02, partial-η2 = .16) and HR (F(1,32) = 3.52, p < .07, partial-η2 = .10) in men in the group that began with relaxed anticipation, and the opposite for women in the group that started with negative anticipation. Finally, a Task by Task-Order by Gender interaction in SCL (F(1.60,51.28) = 2.67, p < .09, partial-η2 = .08) revealed higher baseline HR in women who started with relaxed anticipation, suggesting a smaller change from baseline to anticipation in this subgroup. To provide a concise account of results relevant to our theoretic rational, we therefore chose to omit gender from the analysis.
There are only low and non-significant correlations between trait social anxiety and amplitude of EMG-baselines, confirming that the effect is not a result of signal strength.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- APA. DSM-IV-TR, Diagnostic and statistical manual of mental disorders - text revision. 4th ed. Washington, DC: American Psychiatric Press, Inc.; 2000. [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Beauchaine T. Vagal tone, development, and Gray's motivational theory: toward an integrated model of autonomic nervous system functioning in psychopathology. Development and Psychopathology. 2001;13:183–214. doi: 10.1017/s0954579401002012. [DOI] [PubMed] [Google Scholar]
- Blumenthal TD, Cuthbert BN, Filion DL, Hackley S, Lipp OV, van Boxtel A. Committee report: Guidelines for human startle eyeblink electromyographic studies. Psychophysiology. 2005;42:1–15. doi: 10.1111/j.1469-8986.2005.00271.x. [DOI] [PubMed] [Google Scholar]
- Boucsein W. Electrodermal Activity. New York, NY: Plenum Press; 1992. [Google Scholar]
- Bradley MM, Codispoti M, Lang PJ. A multi-process account of startle modulation during affective perception. Psychophysiology. 2006;43:486–497. doi: 10.1111/j.1469-8986.2006.00412.x. [DOI] [PubMed] [Google Scholar]
- Brown TA, Chorpita BF, Barlow DH. Structural relationships among dimensions of the DSM-IV anxiety and mood disorders and dimensions of negative affect, positive affect, and autonomic arousal. Journal of Abnormal Psychology. 1998;107:179–192. doi: 10.1037//0021-843x.107.2.179. [DOI] [PubMed] [Google Scholar]
- Camm AJ, Malik M, Bigger JT, Breithardt G, Cerutti S, Cohen RJ, et al. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Circulation. 1996;93:1043–1065. [PubMed] [Google Scholar]
- Clark DM, Wells A. A cognitive model of social phobia. In: Heimberg RG, Liebowitz MR, Hope DA, Schneier FR, editors. Social phobia: Diagnosis, assessment, and treatment. New York, NY: Guilford Press; 1995. pp. 69–93. [Google Scholar]
- Cornwell BR, Johnson L, Berardi L, Grillon C. Anticipation of public speaking in virtual reality reveals a relationship between trait social anxiety and startle reactivity. Biological Psychiatry. 2006;59:664–666. doi: 10.1016/j.biopsych.2005.09.015. [DOI] [PubMed] [Google Scholar]
- Dewar KM, Stravynski A. The quest for biological correlates of social phobia: An interim assessment. Acta Psychiatrica Scandinavica. 2001;103:244–251. doi: 10.1034/j.1600-0447.2001.00090.x. [DOI] [PubMed] [Google Scholar]
- Grossman P, Taylor EW. Toward understanding respiratory sinus arrhythmia: relations to cardiac vagal tone, evolution and biobehavioral functions. Biological Psychology. 2007;74:263–285. doi: 10.1016/j.biopsycho.2005.11.014. [DOI] [PubMed] [Google Scholar]
- Hackmann A, Clark DM, McManus F. Recurrent images and early memories in social phobia. Behaviour Research and Therapy. 2000;38:601–610. doi: 10.1016/s0005-7967(99)00161-8. [DOI] [PubMed] [Google Scholar]
- Hackmann A, Surawy C, Clark DM. Seeing yourself through others' eyes: A study of spontaneously occurring images in social phobia. Behavioural and Cognitive Psychotherapy. 1998;26:3–12. [Google Scholar]
- Hayward C, Killen JD, Kraemer HC, Taylor CB. Linking self-reported childhood behavioral inhibition to adolescent social phobia. Journal of the American Academy of Child and Adolescent Psychiatry. 1998;37:1308–1316. doi: 10.1097/00004583-199812000-00015. [DOI] [PubMed] [Google Scholar]
- Hinrichsen H, Clark DM. Anticipatory processing in social anxiety: Two pilot studies. Journal of Behavior Therapy and Experimental Psychiatry. 2003;34:205–218. doi: 10.1016/S0005-7916(03)00050-8. [DOI] [PubMed] [Google Scholar]
- Hofmann SG. Self-focused attention before and after treatment of social phobia. Behaviour Research and Therapy. 2000;38:717–725. doi: 10.1016/s0005-7967(99)00105-9. [DOI] [PubMed] [Google Scholar]
- Hofmann SG. Cognitive Mediation of Treatment Change in Social Phobia. Journal of Consulting and Clinical Psychology. 2004;72:392–399. doi: 10.1037/0022-006X.72.3.392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmann SG. Perception of control over anxiety mediates the relation between catastrophic thinking and social anxiety in social phobia. Behaviour Research and Therapy. 2005;43:885–895. doi: 10.1016/j.brat.2004.07.002. [DOI] [PubMed] [Google Scholar]
- Hofmann SG, Barlow DH. Social phobia (social anxiety disorder) In: Barlow DH, editor. Anxiety and Its Disorders: The Nature and Treatment of Anxiety and Panic. 2nd ed. New York, NY: Guilford Press; 2002. pp. 454–476. [Google Scholar]
- Hofmann SG, DiBartolo PM. An instrument to assess self-statements during public speaking: Scale development and preliminary psychometric properties. Behavior Therapy. 2000;31:499–515. doi: 10.1016/s0005-7894(00)80027-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmann SG, Heinrichs N, Moscovitch DA. The nature and expression of social phobia: Toward a new classification. Clinical Psychology Review. 2004;24:767–797. doi: 10.1016/j.cpr.2004.07.004. [DOI] [PubMed] [Google Scholar]
- Hofmann SG, Moscovitch DA, Kim HJ, Taylor AN. Changes in self-perception during treatment of social phobia. Journal of Consulting and Clinical Psychology. 2004;72:588–596. doi: 10.1037/0022-006X.72.4.588. [DOI] [PubMed] [Google Scholar]
- Hudetz JA, Hudetz AG, Reddy DM. Effect of relaxation on working memory and the bispectral index of the EEG. Psychological Reports. 2004;95:53–70. doi: 10.2466/pr0.95.1.53-70. [DOI] [PubMed] [Google Scholar]
- Kagan J, Reznick JS, Snidman N. The physiology and psychology of behavioral inhibition in children. Child Development. 1987;58:1459–1473. [PubMed] [Google Scholar]
- Kashdan TB, Roberts JE. Social anxiety's impact on affect, curiosity, and social self-efficacy during a high self-focus social threat situation. Cognitive Therapy and Research. 2004;28:119–141. [Google Scholar]
- Longmore RJ, Worrell M. Do we need to challenge thoughts in cognitive behavior therapy? Clinical Psychology Review. 2007;27:173–187. doi: 10.1016/j.cpr.2006.08.001. [DOI] [PubMed] [Google Scholar]
- Mannuzza S, Schneier FR, Chapman TF, Liebowitz MR. Generalized social phobia: Reliability and validity. Archives of General Psychiatry. 1995;52:230–237. doi: 10.1001/archpsyc.1995.03950150062011. [DOI] [PubMed] [Google Scholar]
- Mauss IB, Wilhelm FH, Gross JJ. Is there less to social anxiety than meets the eye? Emotion experience, expression, and bodily responding. Cognition & Emotion. 2004;18:631–662. [Google Scholar]
- Panayiotou G, Vrana SR. Effects of self-focused attention on the startle reflex, heart rate, and memory performance among socially anxious and nonanxious individuals. Psychophysiology. 1998;35:328–336. doi: 10.1017/s0048577298960875. [DOI] [PubMed] [Google Scholar]
- Perini SJ, Abbott MJ, Rapee RM. Perception of performance as a mediator in the relationship between social anxiety and negative post-event rumination. Cognitive Therapy and Research. 2006;30:645–659. [Google Scholar]
- Pollard CA, Henderson JG. Four types of social phobia in a community sample. Journal of Nervous and Mental Disease. 1988;176:440–445. doi: 10.1097/00005053-198807000-00006. [DOI] [PubMed] [Google Scholar]
- Porges SW. Orienting in a defensive world: mammalian modifications of our evolutionary heritage. A Polyvagal Theory. Psychophysiology. 1995;32:301–318. doi: 10.1111/j.1469-8986.1995.tb01213.x. [DOI] [PubMed] [Google Scholar]
- Rapee RM, Heimberg RG. A cognitive-behavioral model of anxiety in social phobia. Behaviour Research and Therapy. 1997;35:741–756. doi: 10.1016/s0005-7967(97)00022-3. [DOI] [PubMed] [Google Scholar]
- Schulz SM, Alpers GW. EMGpeakfind - A MATLAB-toolbox for scoring startle eye-blink, and other EMG data. In: Wascher E, Falkenstein M, Rinkenauer G, Grosjean M, editors. Psychologie und Gehirn 2007. 2007. p. 117. Available at: http://hdl.handle.net/2003/24421. [Google Scholar]
- Sobel ME. Asymptotic confidence intervals for indirect effects in structural equations models. In: Leinhart S, editor. Sociological methodology. San Francisco, CA: Jossey-Bass; 1982. pp. 290–312. [Google Scholar]
- Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press; 1983. [Google Scholar]
- Spurr JM, Stopa L. Self-focused attention in social phobia and social anxiety. Clinical Psychology Review. 2002;22:947–975. doi: 10.1016/s0272-7358(02)00107-1. [DOI] [PubMed] [Google Scholar]
- Steyer R. Theorie kausaler Regressionsmodelle. Stuttgart: Gustav Fischer Verlag; 1992. [Google Scholar]
- Stopa L, Clark DM. Cognitive processes in social phobia. Behaviour Research and Therapy. 1993;31:255–267. doi: 10.1016/0005-7967(93)90024-o. [DOI] [PubMed] [Google Scholar]
- Tabachnick BG, Fidell LS. Using multivariate statistics. 5th ed. New York, NY: Allyn ' Bacon; 2007. [Google Scholar]
- Thayer JF, Brosschot JF. Psychosomatics and psychopathology: Looking up and down from the brain. Psychoneuroendocrinology. 2005;30:1050–1058. doi: 10.1016/j.psyneuen.2005.04.014. [DOI] [PubMed] [Google Scholar]
- Thayer JF, Lane RD. A model of neurovisceral integration in emotion regulation and dysregulation. Journal of Affective Disorders. 2000;61:201–216. doi: 10.1016/s0165-0327(00)00338-4. [DOI] [PubMed] [Google Scholar]
- Turner SM, Beidel DC, Dancu CV, Stanley MA. An empirically derived inventory to measure social fears and anxiety: The Social Phobia and Anxiety Inventory. Psychological Assessment. 1989;1:35–40. [Google Scholar]
- Turner SM, Stanley MA, Beidel DC, Bond L. The Social Phobia and Anxiety Inventory: Construct validity. Journal of Psychopathology & Behavioral Assessment. 1989;11:221–234. [Google Scholar]
- Vassilopoulos S. Anticipatory processing plays a role in maintaining social anxiety. Anxiety, Stress and Coping: An International Journal. 2005;18:321–332. [Google Scholar]
- Vrana SR, Spence EL, Lang PJ. The startle probe response: A new measure of emotion? Journal of Abnormal Psychology. 1988;97:487–491. doi: 10.1037//0021-843x.97.4.487. [DOI] [PubMed] [Google Scholar]
- Wells A, Papageorgiou C. Social phobia: Effects of external attention on anxiety, negative beliefs, and perspective taking. Behavior Therapy. 1998;29:357–370. [Google Scholar]
- Woody SR. Effects of focus of attention on anxiety levels and social performance of individuals with social phobia. Journal of Abnormal Psychology. 1996;105:61–69. doi: 10.1037//0021-843x.105.1.61. [DOI] [PubMed] [Google Scholar]
- Woody SR, Chambless DL, Glass CR. Self-focused attention in the treatment of social phobia. Behaviour Research and Therapy. 1997;35:117–129. doi: 10.1016/s0005-7967(96)00084-8. [DOI] [PubMed] [Google Scholar]