

Abstract
Purpose
Current lithotripters use a dry treatment head that must be coupled to the patient with gel or oil. We sought to determine how the quality of coupling affects stone breakage under conditions that simulated patient treatment.
Methods
Experiments were performed with a Dornier DoLi-50 electromagnetic lithotripter. The test tank had a clear Mylar membrane for coupling with the water cushion of the treatment head. Thus, air pockets trapped at the coupling interface could be photographed for quantitation. Coupling efficiency was assessed using a fiber-optic hydrophone, and different coupling regimes were tested for effect on the breakage of gypsum stones.
Results
The quality of coupling was variable, with air pockets covering 1.5–19% of the coupling area, resulting in a mean reduction in shock wave amplitude of ~20%. Breaking and reestablishing contact, as when a patient is repositioned during treatment, reduced acoustic pressure nearly 32%—a reduction of 57% in the transmission of acoustic energy. Stone breakage was also reduced when air was trapped in coupling, and coverage by air pockets of only 2% reduced stone breakage by 20–40%.
Conclusions
These in vitro results suggest that coupling in lithotripsy can pose a significant barrier to transmission of shock wave energy to the patient. Stone breakage was very sensitive to the presence of air pockets at the coupling interface. Re-coupling was particularly disruptive, suggesting that repositioning the patient could substantially degrade the quality of coupling. It seems reasonable that variability in the quality of coupling could contribute to variability in clinical outcomes
Keywords: lithotripter, shock wave, coupling, stone breakage
Introduction
An important advance in the evolution of lithotripsy was the introduction of the dry treatment head. This eliminated the need to immerse the patient in a water bath, as was done with the Dornier HM3, and paved the way for development of transportable lithotripters. The switch to dry-head technology was quick to occur and was embraced by the major manufacturers, such that all lithotripters currently in production, regardless of the mode of shock wave generation (i.e. electromagnetic, electrohydraulic, piezoelectric), employ a dry treatment head.
Recent reports suggest that newer generation lithotripters may not be as effective as the HM3.1–9 Indeed, no current lithotripter matches the nearly 90% success rate achieved with the HM3.10 There are many differences between current dry-head lithotripters and the water tub-style HM3— including the dimensions and properties of the acoustic fields—so it is difficult to know what physical factors might contribute to this observed disparity in performance. However, poor coupling is a possible factor. In a modern lithotripter the shock source (e.g. spark gap, electromagnetic membrane) is surrounded by water, and the cushion of the treatment head must be coupled to the patient with a medium of high acoustic transmission. Air reflects pressure waves very effectively; indeed, the intensity transmission coefficient for an acoustic wave moving from water to air is only 0.1%. That is, nearly 99.9% of a pressure wave will be reflected at an air pocket at the coupling interface.11 Thus, if there are bubbles in the coupling medium or if pockets of air become captured at the coupling interface, transmission of the shock wave into the patient will be affected.
In the present in vitro study we have investigated the occurrence of air pockets trapped at the coupling interface of a dry-head lithotripter, and the effect these air pockets have on shock wave transmission and stone comminution. The findings show that even under controlled conditions the quality of coupling is highly variable, and disruption of the interface by uncoupling and re-coupling can reduce the energy of the lithotripter pulse by as much as 50%. This suggests that the conventional coupling interface in dry-head lithotripsy is prone to failure, and imperfections in coupling can significantly reduce the transmission of shock waves and hinder the effectiveness of stone breakage.
MATERIALS AND METHODS
Studies were performed using a Dornier DoLi-50 electromagnetic lithotripter (Dornier Medizintechnic GmbH). The DoLi-50 has six power levels, and experiments were conducted at power level 3, at a rate of 60 shock waves (SW’s) per minute. Water pressure within the flexible coupling cushion of the lithotripter is adjustable, and all experiments were performed at coupling setting 3.
A test system was assembled to simulate coupling of the treatment head to the body wall, and consisted of an acrylic water tank (height × width × average depth:40×50×52 cm3) with an acoustic window covered by a sheet of 0.13 mm Mylar (Fig. 1). The components were optically clear, making it possible to observe and photograph air pockets trapped at the coupling interface. LithoClear gel (Sonotech Inc., Bellingham, WA) was used as the coupling medium.
Fig. 1.

Experimental setup for the in vitro study. The water cushion of the lithotripter was coupled to the Mylar membrane of the test tank. Dotted lines mark convergence to the focal point, where the stone basket or tip of the optical fiber hydrophone was positioned.
The occurrence of air pockets at the coupling surface was recorded and quantitated. For quantitation of air pockets, digital images of the coupling interface were recorded from a set vantage point at the rear of the tank, always under the same conditions of incident lighting. The images were post-processed using Adobe Photoshop, and the surface area of air pockets was determined using ImageJ (http://rsb.info.nih.gov/ij/). The accuracy of trapped bubble area determination was estimated to be within 1 cm2. The entire coupling interface was about 120 cm2.
The test tank was filled with tap water degassed overnight with a pinhole degasser12, and the degasser was run continuously during all measurements.13 Water in the tank remained at room temperature (20–22°C) while water in the coupling cushion of the lithotripter was at about 37°C.
A fiber optic hydrophone (FOPH-500, University of Stuttgart, Germany)14 was used to measure the acoustic field. Waveforms were collected at the focus of the lithotripter, which was localized by the following procedure. First a stylus was positioned at the focal point using X-ray alignment of the lithotripter, and the focus was marked with crossed diode laser beams. Position of the hydrophone was readjusted to the point of maximum amplitude of the acoustic field, found by scanning in two directions perpendicular to the acoustic axis of the lithotripter. This refined position was marked by the lasers and was used for measurements. If the hydrophone tip was broken during measurements, a newly prepared tip could be easily positioned at the same place marked in the water by the crossed lasers. Waveforms were recorded using a Tektronix TDS 5034 (Tektronix Inc., Beaverton, Oregon) oscilloscope in sets of 60 shock waves per coupling condition. Averaged waveforms were calculated by aligning recorded pulses to the coincidence of the half amplitude of the shock fronts by a program written in LabVIEW (National Instruments, Austin, TX).
Simultaneous with acoustic measurements, coupling efficiency was assessed by measuring the comminution of gypsum stones.15 Stones were placed in the 2 mm-mesh nylon basket supplied with DoLi-50 test kit, and positioned at the focus of the lithotripter (Fig. 1). Stone particles retained in the mesh basket after 500 shock waves were dried and weighed.
Results
During coupling, air pockets became trapped between the water cushion of the treatment head and the Mylar membrane of the test tank. These pockets could be removed manually by pulling a thin strip of latex (cut from a surgical glove) across the interface. We used coupling with manual removal of air pockets as a baseline condition (air-free) for comparison with other coupling regimes.
Compared to air-free (44±2 MPa), the transmission of acoustic pressure was reduced under routine, single coupling (35±2 MPa), and when the water cushion was coupled, pulled back from the test tank and then re-coupled (30±2 MPa) (Fig. 2). That is, measures of peak positive pressure showed that coupling, as might be done in preparation for lithotripsy, reduced shock wave amplitude by about 20%. Breaking and re-establishing coupling, as might occur when a patient is repositioned during a treatment session, lowered shock wave amplitude by about 32%. Since shock wave energy is proportional to pressure squared integrated over time, the transmission of acoustic energy in this case was reduced by almost 57%.
Fig. 2.
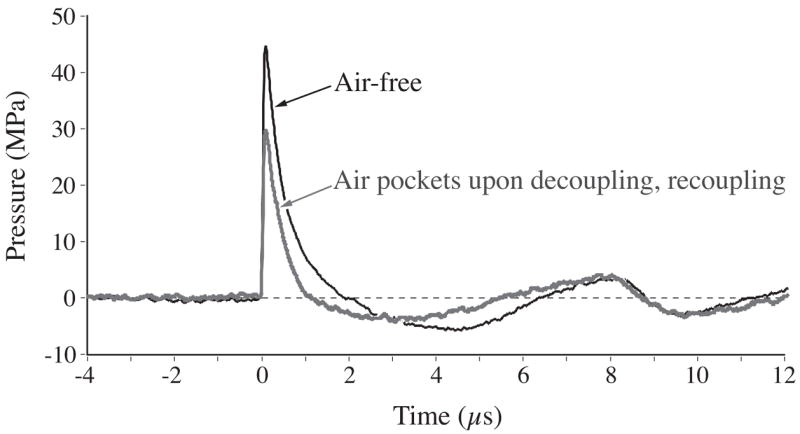
Temporal profiles of lithotripter shock waves recorded with and without air pockets trapped at the coupling interface. This compares the quality of coupling achieved by manual removal of air pockets versus decoupling/re-coupling (photographs of the corresponding coupling conditions are shown in the left and right columns of Fig. 3). Shock waves were recorded by fiber-optic hydrophone positioned at the geometric focus of the lithotripter. Each waveform is an average of 60 shock waves fired at power level 3, and a rate of 60 SW’s/min. The presence of air at the coupling interface reduced shock wave amplitude by about 32%, and total transmitted energy was reduced by about 57%.
The reduction in energy delivery to the focal zone caused by air trapped at the coupling interface also reduced the efficiency of shock waves in stone breakage. Figure 3 shows stone fragments that remained in the 2mm mesh basket following treatment with 500 shock waves under three conditions: when air pockets were removed from the coupling interface, when the water cushion was coupled to the test tank (coupled once), and when the treatment head was decoupled and re-coupled. Breakage was most complete when the interface was free of air pockets, and breakage was poorest when the interface was decoupled and re-coupled. From the images of the coupling interface, it is clear that more air pockets were present with decoupling and re-coupling than with coupling alone. Measures of the surface area of air pockets showed a significant, near-linear correlation (r2=0.8) between stone comminution and air trapped at the coupling interface (Fig. 4). The efficiency of stone breakage was very sensitive to the presence of air at the coupling interface, and only 2% coverage by air pockets reduced breakage by 20–40%.
Fig. 3.

Three coupling regimes used for in vitro testing. When air pockets were manually removed from the coupling interface (left) stone breakage was more efficient than with single coupling (middle) or decoupling/re-coupling (right). Top row shows original photographs of the coupling interface. Middle row shows digitized images with air pockets highlighted for better visibility. Surface area occupied by air pockets in these images was about 0.5%, 6% and 15%, respectively. Bottom row shows stone fragments retained by 2-mm mesh basket following 500 SW’s (power level 3, 60 SW/min) for four stones treated with each coupling regime.
Fig. 4.
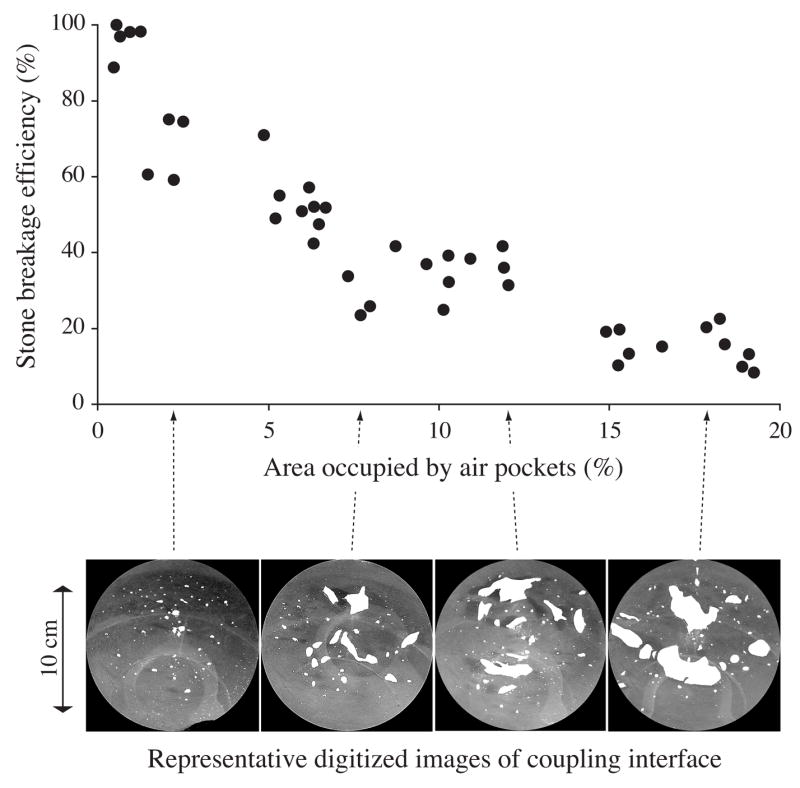
Relationship between efficiency of stone comminution and coverage of the coupling interface by air pockets. Stone breakage (percent of mass lost) declined as air pockets covered more surface area of the coupling interface. At the bottom are digitized images from representative photographs of the coupling interface, with air pockets highlighted for better visibility.
To assess whether the occurrence of air pockets at the coupling interface might be an artifact of the test system, an apparatus was constructed so that a water cushion from the DoLi-50 lithotripter could be brought into contact with skin and the coupling surface visualized. The rubber boot that forms the cushion was filled with water and clamped to the closed end of a cylindrical container, allowing visual access of the coupling interface from the open end of the cylinder. The cylinder was mounted at a 45-degree angle beneath one of the investigators lying on the treatment table. Gel was applied to the cushion, and the volunteer was brought into contact using the motor controls of the table. Figure 5 shows representative images of the coupling interface upon initial contact, and when the cushion was decoupled and re-coupled. Air pockets were trapped in both cases, and by inspection it appeared that the coverage of air pockets trapped against human skin was comparable to that seen with the Mylar membrane of the test system.
Fig. 5.
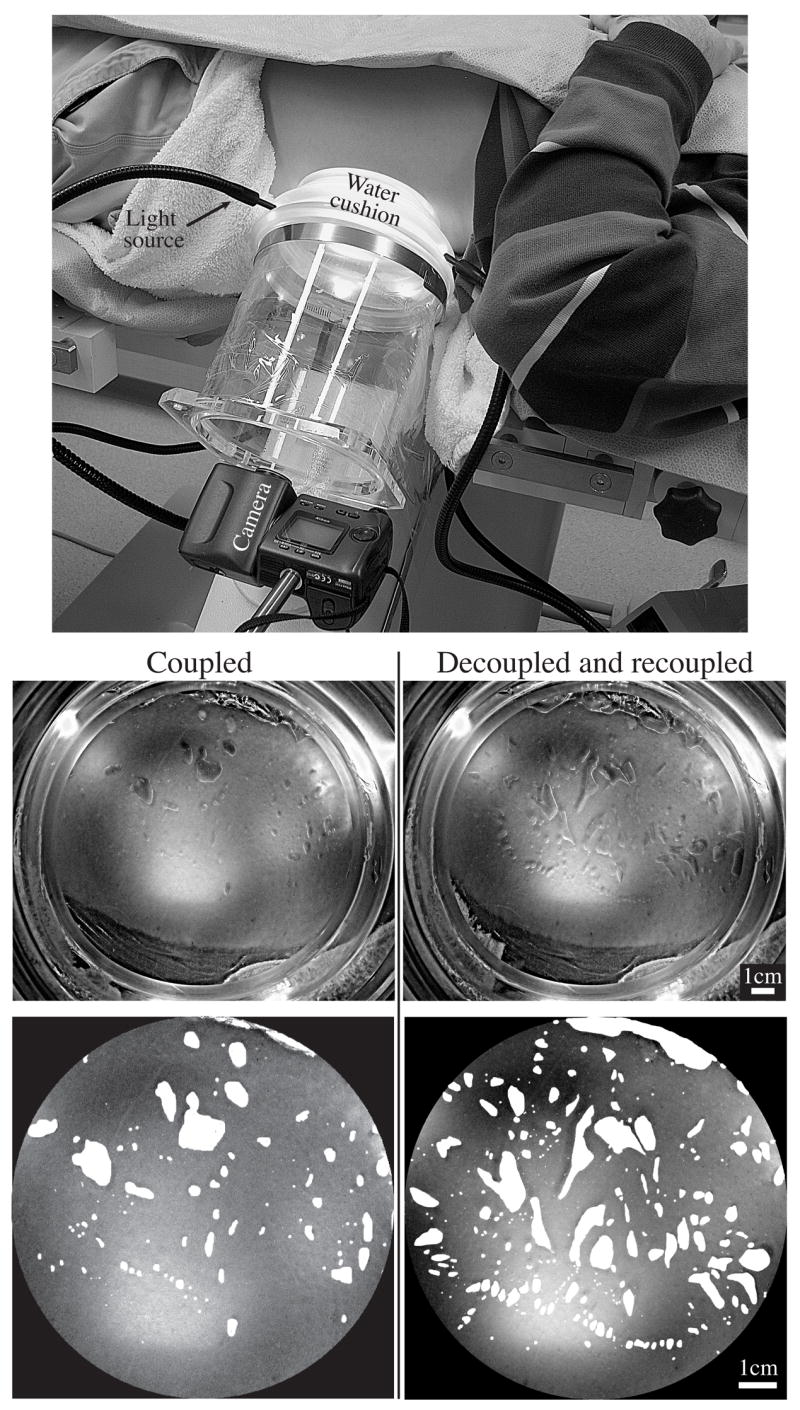
Air pockets became trapped when the lithotripter water cushion was coupled to skin. The cushion was filled with water and mounted on an acrylic cylinder so that the coupling interface could be viewed from behind. Similar to the in vitro setup (Fig. 3), air pockets became trapped against the skin with single coupling, and increased with decoupling/re-coupling (surface area occupied by air pockets in these representative images was about 8% and 16%, respectively).
Discussion
These results suggest that the coupling interface in dry head lithotripters is imperfect. Even under controlled conditions, air pockets were trapped at the interface; these air pockets interfered with acoustic transmission, and the interference was substantial. The coupling scenarios we used were intended to simulate conditions that might be encountered in the handling of a patient. That is, we tested the effect of establishing coupling, and then breaking contact and re-coupling. It was surprising how much interference there was with simple coupling, compared to when air pockets were removed manually from the field. Pulse amplitude was measurably reduced in the presence of air at the coupling interface, and the effect on stone breakage was dramatic. Decoupling and re-coupling was particularly disruptive. This suggests the possibility that, in the clinical setting, repositioning the patient without first repeating the preparation for coupling could substantially degrade the transmission of shock wave energy to the patient.
These data also show that consistency in coupling was hard to achieve; that is the quality of coupling from attempt to attempt showed significant variability. For example, the area of visible air pockets created during single coupling ranged from 1.5% to 19.1%, leading to stone breakage efficiency that ranged from ~80% to less than 10%. Such variability in tests under controlled conditions suggests that variability in coupling could contribute to variability in clinical outcomes.
Variability in coupling may also be a potential safety concern. For example, if the routine coupling regime used by a given practice tended to create many air pockets, then it might become standard procedure to use the lithotripter at increased power in order to achieve good stone breakage. In that setting, high variability could mean that those patients who happened to be coupled to the lithotripter with fewer air pockets would get a higher dose of shock wave energy actually delivered to their kidneys, increasing the possibility of renal injury16.
A variety of media such as petroleum jelly, anesthetic cream, lubricating jelly, ultrasonography gel and castor oil have been used as coupling agents, and an in vitro study by Cartledge and coworkers17 indicates that the type of coupling agent can have a significant effect on the breakage of model stones. We used a commercial gel (LithoClear) marketed specifically as a lithotripsy coupling agent. This material was not the source of air pockets; that is, large bubbles did not form within the gel during shock wave exposure. Indeed, in some cases air pockets present at the coupling interface at the start of treatment filled in after several hundred shock waves had been fired. It may be that there are other coupling agents that work as well, or other agents that are not as effective for coupling. Similarly, the way in which the coupling agent is applied may have a significant effect on the quality of coupling. The current study used only one method of delivering gel to the treatment head. In preliminary experiments we have observed that applying gel to both the water cushion and the test membrane gives very poor coupling, but that coupling is improved by applying an excessive amount of gel to just the water cushion. This suggests that how a coupling agent is applied makes a difference. Such tests to compare coupling agents or to find the best coupling regime may be valuable to perform, and the in vitro test system used in the present studies could be useful in this sort of assessment.
With this in vitro test system we were able to correlate stone breakage and pulse amplitude with the surface area of air pockets at the coupling interface, because the interface was visible. This is not the case for lithotripsy of patients, and one never knows when bubbles are present. It would be valuable to have a way to make this assessment. Some lithotripters are now equipped with b-mode ultrasound aligned along the acoustic axis. It should be feasible to use this targeting feature to check the quality of coupling. It will have to be determined what constitutes poor coupling, but our in vitro tests (see Figs. 2 and 3) suggest that coverage by air pockets of only 15% of the field reduces the transmission of acoustic energy by almost 60%. Our results show that interference with the shock pulse increases the number of shock waves needed to comminute stones. This may be occurring in patients. If so, these patients will be receiving more shock waves than are necessary—more shock waves than should be needed under ideal treatment conditions—and this is a potential safety concern.
Conclusions
The quality of coupling is a potentially significant variable in shock wave lithotripsy. Poor coupling reduces the effectiveness of stone breakage, requiring that more shock waves be delivered to achieve complete comminution. The quality of coupling is highly variable from attempt to attempt, and this could contribute to variability in clinical outcomes. Inadequate coupling and variability in the quality of coupling likely lead to treatment of patients with more shock waves than are necessary. For these reasons, additional research should be conducted to find ways to assess the quality of coupling during lithotripsy, and to improve the consistency of coupling regimes.
Acknowledgments
This research was supported by a grant from the National Institutes of Health, DK43881. The DoLi-50 lithotripter was donated by American Kidney Stone Management (Columbus, OH).
References
- 1.Gerber R, Studer UE, Danuser H. Is newer better? A comparative study of 3 lithotripter generations. J Urol. 2005;173:2013. doi: 10.1097/01.ju.0000158042.41319.c4. [DOI] [PubMed] [Google Scholar]
- 2.Matin SF, Yost A, Streem SB. Extracorporeal shock-wave lithotripsy: a comparative study of electrohydraulic and electromagnetic units. J Urol. 2001;166:2053. doi: 10.1016/s0022-5347(05)65504-8. [DOI] [PubMed] [Google Scholar]
- 3.Graber SF, Danuser H, Hochreiter WW, Studer UE. A prospective randomized trial comparing 2 lithotriptors for stone disintegration and induced renal trauma. J Urol. 2003;169:54. doi: 10.1016/S0022-5347(05)64033-5. [DOI] [PubMed] [Google Scholar]
- 4.Ng CF, McLornan L, Thompson TJ, Tolley DA. Comparison of 2 generations of piezoelectric lithotriptors using matched pair analysis. J Urol. 2004;172:1887. doi: 10.1097/01.ju.0000142730.60583.7a. [DOI] [PubMed] [Google Scholar]
- 5.Teichman JMH, Portis AJ, Cecconi PP, Bub WL, Endicott RC, Denes B, Pearle MS, Clayman RV. In vitro comparison of shock wave lithotripsy machines. J Urol. 2000;164:1259. [PubMed] [Google Scholar]
- 6.Rassweiler J, Henkel TO, Kohrmann KU, Potempa D, Junemann KP, Alken P. Lithotriptor technology: present and future. J Endourol. 1992;6:1. [Google Scholar]
- 7.Bierkens AF, Hendrikx AJ, de Kort VJ, de Reyke T, Bruynen CA, Bouve ER, Beek TV, Vos P, Berkel HV. Efficacy of second generation lithotriptors: a multicenter comparative study of 2,206 extracorporeal shock wave lithotripsy treatments with the Siemens Lithostar, Dornier HM4, Wolf Piezolith 2300, Direx Tripter X-1 and Breakstone lithotriptors. J Urol. 1992;148:1052. doi: 10.1016/s0022-5347(17)36814-3. [DOI] [PubMed] [Google Scholar]
- 8.Lingeman JE. Extracorporeal shock wave lithotripsy: Development, instrumentation, and current status. Urol Clin North Am. 1997;24:185. doi: 10.1016/s0094-0143(05)70363-3. [DOI] [PubMed] [Google Scholar]
- 9.Portis AJ, Yan Y, Pattaras JG, Andreoni C, Moore R, Clayman RV. Matched pair analysis of shock wave lithotripsy effectiveness for comparison of lithotriptors. J Urol. 2003;169:58. doi: 10.1016/S0022-5347(05)64034-7. [DOI] [PubMed] [Google Scholar]
- 10.Lingeman JE, Newman D, Mertz JHO, Mosbaugh PG, Steele RE, Kahnoski J, Coury TA, Woods JR. Extracorporeal shock wave lithotripsy: the Methodist Hospital of Indiana experience. J Urol. 1986;135:1134. doi: 10.1016/s0022-5347(17)46016-2. [DOI] [PubMed] [Google Scholar]
- 11.Cleveland RO, McAteer JA. The Physics of Shock Wave Lithotripsy. Smith’s Textbook on Endourology. Chapter 38 In Press. [Google Scholar]
- 12.Kaiser AR, Cain CA, Hwang EY, Fowlkes JB, Jeffers RJ. A cost effective degassing system for use in ultrasonic measurements: The multiple pinhole degassing (mpd) system. J Acoust Soc Am. 1996;99:3857. [Google Scholar]
- 13.Pishchalnikov YA, Sapozhnikov OA, Bailey MR, Pishchalnikova IV, Williams JC, Jr, McAteer JA. Cavitation selectively reduces the negative-pressure phase of lithotripter shock waves. Acoust Res Lett On-line. 2005;6:280. doi: 10.1121/1.2127115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Stardenraus J, Eisenmenger W. Fiber-optic probe hydrophone for ultrasonic and shock-wave measurements in water. Ultrasonics. 1993;31:267. [Google Scholar]
- 15.McAteer JA, Williams JC, Jr, Cleveland RO, Van Cauwelaert J, Bailey MR, Lifshitz DA, Evan AP. Ultracal-30 gypsum artificial stones for research on the mechanisms of stone breakage in shock wave lithotripsy. Urological Research. doi: 10.1007/s00240-005-0503-5. on-line 31 August 2005. [DOI] [PubMed] [Google Scholar]
- 16.Evan AP, McAteer JA. Q-Effects of shock wave lithotripsy. In: Coe FL, Favus MJ, Pak CYC, Parks JH, Preminger GM, editors. Kidney Stones: Medical and Surgical Management. Lippincott-Raven; Philadelphia: 1996. pp. 549–570. [Google Scholar]
- 17.Cartledge JJ, Cross WR, Lloyd SN, Joyce AD. The efficacy of a range of contact media as coupling agents in extracorporeal shockwave lithotripsy. BJU International. 2001;88:321. doi: 10.1046/j.1464-410x.2001.02289.x. [DOI] [PubMed] [Google Scholar]