

Abstract
Delay discounting (DD) describes how the value of a reinforcer decreases as delay to its delivery increases. Relationships between DD and various aspects of drug abuse have been demonstrated reliably. A potential barrier to wider adoption of DD techniques is that results are often expressed in terms that may be too abstract or unfamiliar to a broader audience, particularly when describing or comparing hyperbolic DD functions or values of k. In an effort to potentially make DD results more accessible, the current report explores use of an ED50 value in characterizing DD functions, similar to that used in pharmacology research for characterizing dose-effect functions. The ED50 proposed with regard to DD is the delay that is effective in discounting the subjective value of the delayed reinforcer by 50%. Additionally, a convenient method for calculating ED50 values for DD is discussed.
Keywords: Delay Discounting, Impulsivity, Drug Abuse
1. Delay Discounting and Drug Abuse
Delay discounting (DD) describes how the value of a reinforcer decreases as a function of increased delay to delivery (Bickel & Marsch, 2001; Reynolds, 2006). DD provides an account for why organisms will often times choose a smaller, more immediate reinforcer over a larger, delayed one, and has been used to provide an operational definition of at least certain aspects of impulsivity (Logue, 1995; Rachlin & Green, 1972).
Substance abuse can be conceptualized as a problem of impulsivity in which the immediate reinforcing effects of drug consumption are preferred over the longer-term benefits of abstaining from drug abuse (e.g., educational achievement, improved health, financial stability). An emerging literature demonstrates that drug abusers reliably exhibit greater DD when compared to non-drug abusers matched on other socio-demographic characteristics (Bickel & Marsch, 2001; Reynolds, 2006). Compared to non-drug abusers, greater DD has been observed in abusers of opiates (Kirby et al., 1999; Madden et al., 1997), cocaine (Coffey et al., 2003; Heil et al., 2006; Kirby & Petry, 2004), alcohol (Petry, 2001a; Reynolds, et al., 2006; Richards et al., 1999), and cigarettes (Baker et al., 2003; Bickel et al., 1999; Mitchell, 1999). Drug abusers who engage in additional risky behavior (e.g., needle sharing) exhibit greater discounting compared to drug abusers who do not engage in such risky behavior (Odum et al., 2000). Likewise, drug abusers who gamble excessively discount more than drug abusers without gambling problems (Petry, 2001b; Petry & Casarella, 1999). Increases in DD have also been observed during acute withdrawal from opiates (Giordano et al., 2002) and tobacco (Field, 2006; Mitchell 2004). Finally, greater baseline DD predicts poor treatment outcome among those trying to quit cigarette smoking (Dallery & Raiff, 2007; Krishnan et al., 2007; Yoon et al., 2007). Clearly, the breadth of evidence linking DD with drug abuse is compelling and worthy of further investigation.
2. Assessment of Delay Discounting
Assessing DD typically involves procedures similar to those used in psychophysical experiments in which one stimulus is held constant while another is systematically varied (Gescheider, 1997; Richards et al., 1997). Using such methods, the experimenter can discern at what point a subject deems two stimuli to be equivalent along some dimension. Likewise, in DD tasks an adjusting-amount procedure presents subjects with a choice between a smaller, more immediate and a larger, more delayed reinforcer. The magnitude of the more immediate reinforcer is systematically varied until no clear preference is observed between the immediate and delayed reinforcers, otherwise referred to as an indifference point. By determining indifference points at different temporal delays, a DD function can be established that relates the subjective value of the reinforcer to the amount of delay to its availability. The shape of DD functions have been demonstrated to be hyperbolic rather exponential in both human and non-human subjects (e.g., Rodriquez & Logue, 1988; Rachlin et al., 1991; Myerson & Green, 1995; Kirby et al., 2004), meaning that the rate of discounting is inversely proportional to delay. In other words, the value of a reinforcer decreases rapidly at relatively shorter delays and more gradually at relatively longer delays.
| (1) |
Equation 1 Mazur, 1987 describes how the value (V) of a reinforcer of initial magnitude (A) decreases as a function of delay (D) to receiving that reinforcer. When D is zero, A retains its full value. As D increases, the value of A approaches zero. By assessing indifference points as described above, one is able to calculate V at different delays. The free parameter k represents the rate of discounting and can serve as a parametric, operational representation of the degree of impulsive responding. Higher k values correspond with greater discounting, and therefore greater impulsivity (i.e., steeper DD curve).
3. Clarifying Delay Discounting Results
A potential hurdle in conveying DD methods and findings to drug abuse researchers is that the interpretation of DD results may be unfamiliar. For example, differences in DD between populations are often shown as two separate hyperbolic discounting curves plotting V as a function of D. Even if differences in rates of discounting between the two curves are reported to be statistically significant, the results can be difficult to comprehend in everyday terms. How much steeper or more shallow should one curve be in order for a reader to discuss a meaningful difference in discounting? The problem of unfamiliarity can be compounded under circumstances when DD results are simply conveyed as differences in observed k values, which use the units of inverse time and often range over several orders of magnitude across participants in a study (e.g., Kirby et al., 1999; Yoon et al., 2007).
A technique for making comparisons between DD curves more intuitive or practical may be useful. Fortunately, a model already exists in pharmacology research that may be helpful. In pharmacology, the relationship between drug response and the concentration of drug present at the receptor is characterized by dose-effect curves. At relatively low drug doses, little drug effect is observed, but as drug dose increases, the drug effect also increases until a maximum drug effect is reached. A commonly used method for quantifying drug action in receptor pharmacology is the ED50, the dose of drug at which 50% of the maximum drug effect is observed (Ross & Kenakin, 2001). Shifts in the dose-response functions due to various influences such as the presence of an agonist, antagonist, or tolerance are often conveniently described and contrasted as changes in ED50 values.
A similar measure may be useful in DD research. Such a practice would not be completely alien as some DD reports have already used similar methods to compare DD functions, although such descriptions have always been secondary to statistical descriptions. For example, one method is to pick an arbitrary delay and report differences in the value at that delay. Conversely, an arbitrary value can be chosen and the results described in terms of differences in time. Instead of using an arbitrary value, however, we propose consideration of a midpoint value like the ED50 that is less likely to be affected by floor or ceiling effects in the data and overtime would become familiar to readers of and contributors to the DD literature. Specifically, we are suggesting the delay that effectively discounts the value of the delayed reinforcer by 50%. We propose that this new measure be referred to as an ED50 as well, except that instead of the effective dose, we are referring to the effective delay. Such an ED50 value can be readily calculated by manipulating Equation 1 in the following manner:
First, substitute A/2 for V. This alters the formula to specifically look for the delay at which the reinforcer (A) value is reduced to half its original amount. The variable D is therefore the ED50 measure.
| (2) |
Next, the A values cancel out and cross-multiplying yields Equation 3.
| (3) |
Subtracting by 1 on both sides and dividing by k yields the final formula.
| (4) |
Quite conveniently, the delay at which A decreases to 50% of its original value is simply 1/k. At this time, we would like to emphasize that we are not advocating replacing graphs of DD curves with ED50 values. Instead, ED50 values would be used to enhance descriptions of DD discounting functions in a similar manner as they do in pharmacology research for dose-effect functions.
As an illustrative example, a frequency distribution of obtained k values from a previous study we conducted (Yoon et al., 2007) was examined in order to obtain representative k values (Fig. 1, top). The three most commonly observed k values were chosen, including the peak value and a k value that was higher and lower than the peak k value that were approximately on equal levels of the normal distribution. The three k values chosen were 3.4×10−4(a), 9.1×10−4(b), and 2.5×10−3(c). It should be immediately apparent that the difference in magnitude between these k values alone would be difficult to interpret for a general audience, except perhaps for the fact that 2.5×10−3 represents greater discounting than 3.4×10−4. By plotting the three k values according to Equation 1 (Fig. 1, bottom), the relationship across k values becomes clearer and easier to compare but arguably still difficult to interpret in practical terms without focusing on points at a particular value or delay. That is where we are proposing that by inverting k values and converting into years to obtain ED50 values (Equation 4) can be helpful. In this case, the ED50 values are 8.1, 3.0, and 1.1 years for curves a, b, and c, respectively. Described in other terms, there was a nearly 3-fold difference between curves c and b and an approximately 8-fold difference between curves c and a in the delay necessary to effectively reduce the value of the reinforcer by 50%.
Fig. 1.
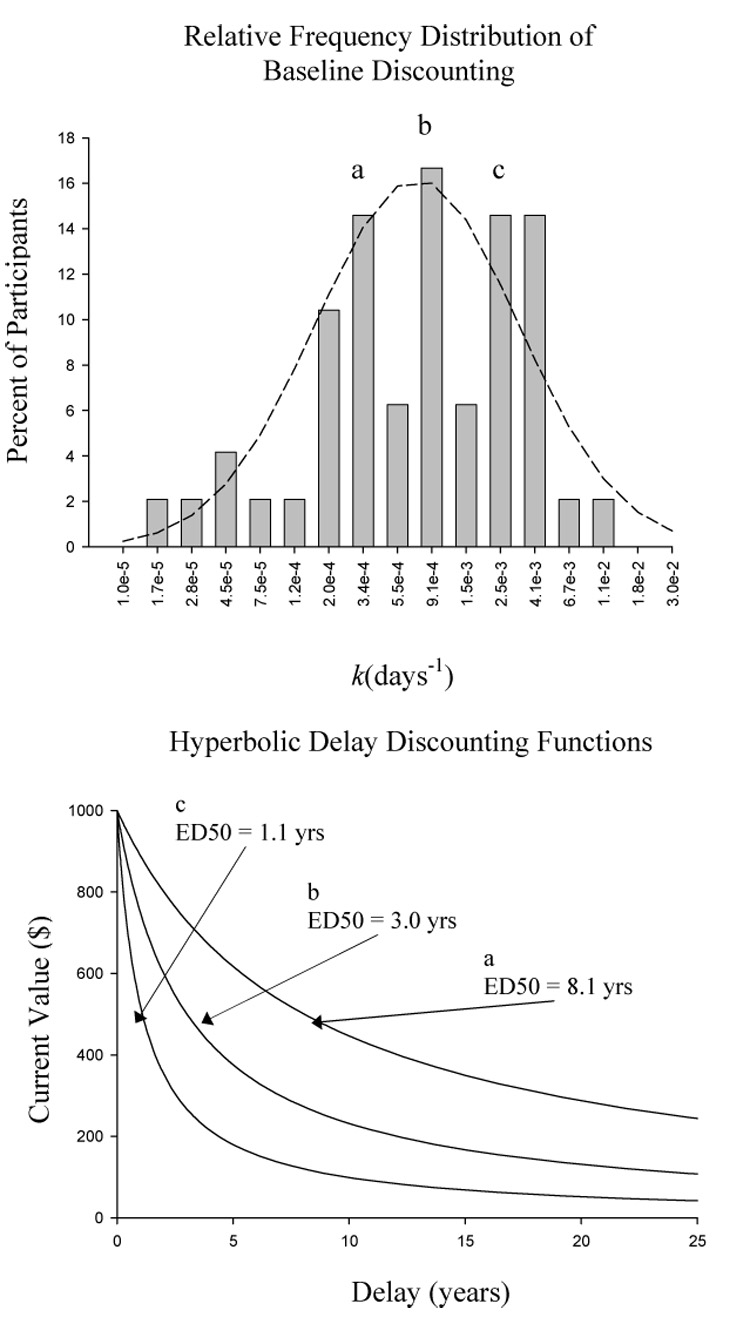
Various representations of DD. Top panel shows the relative frequency distribution of baseline k values on a log scale. The curve represents the best-fit normal distribution function. Note that higher k values represent greater rates of DD. Representative k values marked a, b, and c are graphed according to Equation 1 in the bottom panel. Note that steeper, shallower curves indicate greater DD.
4. Benefits of Using an ED50 Value with Explicit Time Units
The primary purpose of introducing the ED50 measure is to increase the ease of interpreting DD results. The primary facilitating mechanism appears to be that the ED50 value uses the units of time, a clearly more common measure than that of k, the inverse of time. Reporting ED50 values, with explicit time units, therefore has several benefits that make DD results more accessible. First, when comparing DD curves (Fig. 1, bottom), ED50 values should provide readers greater confidence in judging differences in the magnitude of DD results for themselves rather than basing their opinions solely on reports of statistical significance or differences in k. Second, use of ED50 values should increase the ease in comparing findings not only within a study, but across studies as well. Currently, k is often reported without any accompanying units at all. Furthermore, different units of time (e.g., days, months, years, etc) can be used in calculating k, which results in different values of k. Using an ED50 value with explicit time units should therefore alleviate some of the vagueness inherent in the way k values are generally reported. This change in turn should simplify comparing DD results across experiments, thereby facilitating examinations of the generality of DD results. Third, an extension of the second point would be that the field could begin to gain a sense of what kind of ED50 values one should expect from drug abusing versus non-abusing populations. Although reliable differences in DD have been observed between drug abusers and non-abusers as described above, there is very little sense in the field as to what a given k value means in the same way researchers examining cocaine abuse would know what is a relatively high or low dose of cocaine.
At this point, it should be stressed that the main benefit of the ED50 measure is in increasing interpretive ease by describing DD in everyday terms. Since the ED50 value is simply the inverse of k, problems associated with the analysis of k (e.g., requiring non-linear regression, non-normally distributed) remain associated with ED50 values. For example, Area Under the Curve (AUC, Myerson et al., 2001) is an alternative measure of DD that has certain advantages over k as well as the currently proposed ED50 value (amenable to linear regression analysis methods, normally distributed, easily calculated). The ED50 measure, however, is still arguably more tangible than that of AUC, which has values ranging from 0 to 1. Additionally, Mazur’s k value is still widely used and reported. Therefore, as long as k values continue to be reported, we feel that the extra step of calculating the ED50 value by inverting k is warranted by the potential benefits described above.
5. Conclusions
Research in DD has revealed a variety of reliable associations between sensitivity to delayed consequences and various aspects of drug abuse and other disorders. The current report introduces a simple method for calculating an ED50 value that may be useful in this emerging research area. Adoption of reporting ED50 values wherever k is used has potentially significant contributions to make in the ease of interpreting DD results and making within and across study comparisons.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Baker F, Johson MW, Bickel WK. Delay discounting in current and never-before cigarette smokers: Similarities and differences across commodity, sign, and magnitude. J Abnorm Psychol. 2003;112:382–392. doi: 10.1037/0021-843x.112.3.382. [DOI] [PubMed] [Google Scholar]
- Bickel WK, Marsch L. Toward a behavioral economic understanding of drug dependence: Delay discounting processes. Addiction. 2001;96:73–86. doi: 10.1046/j.1360-0443.2001.961736.x. [DOI] [PubMed] [Google Scholar]
- Bickel WK, Odum AL, Madden GJ. Impulsivity and cigarette smoking: Delay discounting in current, never, and ex-smokers. Psychopharmacology (Berl) 1999;146:477–454. doi: 10.1007/pl00005490. [DOI] [PubMed] [Google Scholar]
- Coffey SF, Gudleski GD, Saldin ME, Brady KT. Impulsivity and rapid discounting of delayed hypothetical rewards in cocaine-dependent individuals. Exp Clin Psychopharmacol. 2003;11:18–25. doi: 10.1037//1064-1297.11.1.18. [DOI] [PubMed] [Google Scholar]
- Dallery J, Raiff BR. Delay discounting predicts cigarette smoking in a laboratory model of abstinence reinforcement. Psychopharmacology (Berl) 2007;190:485–496. doi: 10.1007/s00213-006-0627-5. [DOI] [PubMed] [Google Scholar]
- Fields M, Santarcangelo M, Sumnall H, Goudie AJ, Cole J. Delay discounting and the behavioral economics of cigarette purchases in smokers: The effects of nicotine deprivation. Psychopharmacology (Berl) 2006;186:255–263. doi: 10.1007/s00213-006-0385-4. [DOI] [PubMed] [Google Scholar]
- Gescheider GA. Psychophysics: The Fundamentals. 3rd ed. New Jersey: Erlbaum; 1997. [Google Scholar]
- Giordano LA, Bickel WK, Loewenstein G, Jacobs EA, Marsch L, Badger GJ. Mild opioid deprivation increases the degree that opioid-dependent outpatients discount delayed heroin and money. Psychopharmacology (Berl) 2002;163:174–182. doi: 10.1007/s00213-002-1159-2. [DOI] [PubMed] [Google Scholar]
- Heil SH, Johnson MW, Higgins ST, Bickel WK. Delay discounting in currently using and currently abstinent cocaine-dependent outpatients and non-drug using matched controls. Addict Behav. 2006:1290–1294. doi: 10.1016/j.addbeh.2005.09.005. [DOI] [PubMed] [Google Scholar]
- Kirby KN, Petry NM. Heroin and cocaine abusers have higher discount rates for delayed rewards than alcoholics or non-drug-using controls. Addiction. 2004;99:461–471. doi: 10.1111/j.1360-0443.2003.00669.x. [DOI] [PubMed] [Google Scholar]
- Kirby KN, Petry NM, Bickel WK. Heroin addicts have higher discounting for delayed rewards then alcoholics or non-drug-using controls. Addiction. 1999;99:461–471. doi: 10.1111/j.1360-0443.2003.00669.x. [DOI] [PubMed] [Google Scholar]
- Krishnan-Sarin S, Reynolds B, Duhig AM, Smith A, Liss T, McFetridge A, Cavallo DA, Carroll KM, Potenza MN. Behavioral impulsivity predicts treatment outcome in a smoking cessation program for adolescent smokers. Drug Alcohol Depend. 2006:79–82. doi: 10.1016/j.drugalcdep.2006.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Logue AW. Self-control: Waiting until tomorrow for what you want today. New Jersey: Prentice-Hall; 1995. [Google Scholar]
- Madden GJ, Petry N, Badger G, Bickel WK. Impulsive and self-control choices in opioid-dependent patients and non-drug-using control participants: Drug and monetary rewards. Exp Clin Psychopharmacol. 1997;5:256–262. doi: 10.1037//1064-1297.5.3.256. [DOI] [PubMed] [Google Scholar]
- Mazur JE. An adjusting procedure for studying delayed reinforcement. In: Commons ML, Mazure JM, Nevin JA, Rachlin H, editors. Quantitative Analysis of Behavior: Vol. 5. The Effects of Delay and of Intervening Events on Reinforcement Value. New Jersey: Erlbaum; 1987. pp. 55–73. [Google Scholar]
- Mitchell SH. Effects of short-term nicotine deprivation on decision making: Delay, uncertainty, and effort discounting. Nicotine Tob Res. 2004;6:819–828. doi: 10.1080/14622200412331296002. [DOI] [PubMed] [Google Scholar]
- Myerson J, Green L. Discounting of delayed rewards: Models of individual choice. J Exp Anal Behav. 1995;64:263–276. doi: 10.1901/jeab.1995.64-263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myerson J, Green L, Warusawitharana M. Area under the curve as a measure of discounting. J Exp Anal Behav. 2001;76:234–243. doi: 10.1901/jeab.2001.76-235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odum AL, Madden GJ, Badger GJ, Bickel WK. Needle sharing in opioid-dependent outpatients: Psychological processes underlying risk. Drug Alcohol Depend. 2000;60:259–266. doi: 10.1016/s0376-8716(00)00111-3. [DOI] [PubMed] [Google Scholar]
- Petry NM. Delay discounting of money and alcohol in actively using alcoholics, currently abstinent alcoholics, and controls. Psychopharmacology (Berl) 2001a;154:243–250. doi: 10.1007/s002130000638. [DOI] [PubMed] [Google Scholar]
- Petry NM. Pathological gamblers, with and without substance use disorders, discount delayed rewards at high rates. J Abnorm Psychol. 2001b;110:428–487. doi: 10.1037//0021-843x.110.3.482. [DOI] [PubMed] [Google Scholar]
- Petry NM, Casarella R. Excessive discounting of delayed rewards in substance abusers with gambling problems. Drug Alcohol Depend. 1999;56:25–32. doi: 10.1016/s0376-8716(99)00010-1. [DOI] [PubMed] [Google Scholar]
- Rachlin H, Green L. Commitment, choice, and self-control. J Exp Anal Beh. 1972;17:15–22. doi: 10.1901/jeab.1972.17-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rachlin H, Raineri A, Cross D. Subjective probability of delay. J Exp Anal Beh. 1991;55:233–244. doi: 10.1901/jeab.1991.55-233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reynolds B. A review of delay-discounting research with humans: relations to drug use and gambling. Behav Pharmacol. 2006;17:651–667. doi: 10.1097/FBP.0b013e3280115f99. [DOI] [PubMed] [Google Scholar]
- Reynolds B, Richards JB, de Wit H. Acute-alcohol effects on the Experiential Discounting Task (EDT) and a question-based measure of delay discounting. Pharmacolo Biochem Behav. 2006;83:194–202. doi: 10.1016/j.pbb.2006.01.007. [DOI] [PubMed] [Google Scholar]
- Reynolds B, Schiffbauer R. Measuring state changes in human delay discounting: An experiential discounting task. Behav Processes. 2004;67:343–356. doi: 10.1016/j.beproc.2004.06.003. [DOI] [PubMed] [Google Scholar]
- Richards JB, Mitchell S, de Wit H, Seiden L. Determination of discount functions in rats with an adjusting-amount procedure. J Exp Anal Beh. 1997;67:353–363. doi: 10.1901/jeab.1997.67-353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richards JB, Mitchell S, de Wit H, Seiden L. Delay or probability discounting in a model of impulsive behavior: Effect of alcohol. J Exp Anal Beh. 1999;71:121–143. doi: 10.1901/jeab.1999.71-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodriquez ML, Logue AW. Adjusting delay to reinforcement: Comparing choice in pigeons and humans. J Exp Psychol Anim Behav Process. 1988;14:105–117. [PubMed] [Google Scholar]
- Ross EM, Kenakin TP. Pharmacodynamics – mechanisms of drug action and the relationship between drug concentration and effect. In: Hardman JG, Gilman AJ, editors. The Pharmacological Basis of Therapeutics. 10th ed. London: McGraw; 2001. pp. 31–45. [Google Scholar]
- Yoon JH, Higgins ST, Heil SH, Sugarbaker RJ, Thomas CS, Badger GJ. Delay discounting predicts postpartum relapse to cigarette smoking among pregnant women. Exp Clin Psychopharmacol. 2007;15:176–186. doi: 10.1037/1064-1297.15.2.186. [DOI] [PubMed] [Google Scholar]