

Caseous calcification of the mitral annulus (CCMA) is a rare variant of mitral annulus calcification (MAC), constituting about 0.63% of all MAC cases.1 Although CCMA is usually a benign, asymptomatic condition, it is often misconstrued as a cardiac tumor,2,3 a thrombus,4 or an abscess,5 which leads to unnecessary investigations and interventions. Transthoracic echocardiography is a very useful tool for diagnosing this condition.
A 71-year-old man, with no relevant medical history, presented elsewhere with recurrent episodes of dizziness and near-syncope. An echocardiogram revealed a large mass involving the mitral annulus. The patient was told that he had a cardiac tumor and was referred to our hospital for surgical removal of the lesion.
On arrival, additional imaging studies were ordered. Gated myocardial perfusion single-positron-emission computed tomography showed normal systolic function and normal left ventricular wall motion. At cardiac catheterization, the coronary arteries were normal, but a bulky calcific mass was again noted in proximity to the mitral valve (Figs. 1 and 2). The patient underwent cardiac magnetic resonance imaging (MRI), which showed a mass attached mostly to the lateral part of the posterior mitral annulus. On T1 and T2-weighted imaging, the mass had a low-signal intensity that suggested calcification (Fig. 3). The lesion's appearance was not consistent with that of an atrial myxoma or hemangioma.

Fig. 1 Anteroposterior view, obtained during cardiac catheterization, of a 3 × 4-cm calcific mass attached to the mitral annulus.
Real-time motion images are available at texasheart.org/journal

Fig. 2 Left anterior oblique view, obtained during cardiac catheterization, shows the spatial relationship of the left anterior descending and left circumflex arteries to the calcific mass.
Real-time motion images are available at texasheart.org/journal

Fig. 3 Cardiac magnetic resonance image of a hypo-intense mass (arrow) attached to the mitral annulus.
Real-time motion images are available at texasheart.org/journal
Our consultative review of the outside echocardiogram confirmed a large, well demarcated, sausage-shaped, echodense mass integral to the mitral annulus and measuring 3 × 2.9 cm in cross-section. The mass affected the entire base of the posterior mitral valve leaflet and involved part of the basal ventricular myocardium (Figs. 4 and 5). Mitral valve function was normal, and there was no evidence of either mitral regurgitation or mitral stenosis (Fig. 6). Except for mild left ventricular hypertrophy, no other significant structural or hemodynamic abnormalities were noted. Caseous calcification of the mitral annulus was suspected, and this diagnosis was supported by the cardiac MRI findings. However, the cause of the patient's symptoms was still in question.

Fig. 4 Two-dimensional echocardiogram, in the parasternal long-axis view, of a calcific mass attached to the mitral valve.
Real-time motion images are available at texasheart.org/journal
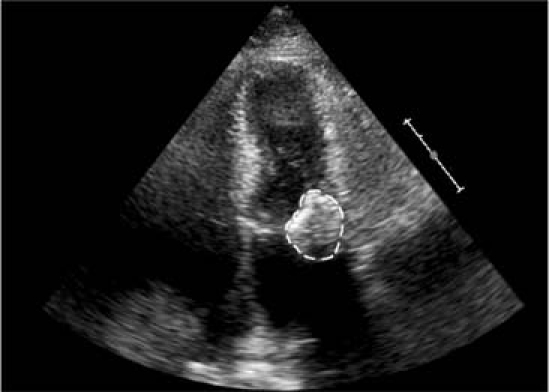
Fig. 5 Two-dimensional echocardiogram, in the apical 4-chamber view, of a calcific mass attached to the mitral annulus.
Real-time motion images, including color Doppler, are available at texasheart.org/journal
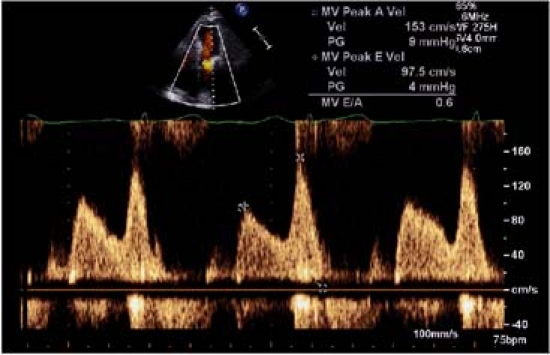
Fig. 6 Spectral Doppler echocardiogram of the mitral inflow tract, in the apical 4-chamber view. No significant stenosis or regurgitation is present.
The patient then had a diagnostic episode of monitored near-syncope, during which an electrocardiogram showed regular narrow-complex tachycardia at 125 beats/min that converted to normal sinus rhythm after an adenosine injection. The patient underwent an electrophysiologic study in which atrioventricular nodal re-entry tachycardia (slow-fast type) was induced, and radiofrequency ablation of the slow pathway was successfully performed. He had no further episodes of atrioventricular nodal re-entry tachycardia and was discharged from the hospital. Our patient did not undergo surgical resection of the mass, which we considered a large but innocent bystander, apparent on the initial echocardiogram without the need for additional studies.
In cases of CCMA, echocardiography usually reveals a large, round, echodense mass with smooth borders and central areas of echolucency.1 The lesion is usually located on the posterior mitral leaflet and contains caseous putty-like material surrounded by a calcified envelope. Microscopic examination shows this material to be amorphous, acellular, basophilic, and calcific, with a mild chronic inflammatory reaction manifested mainly by macrophages. However, pathologic confirmation is not usually required for a diagnosis, because image-based findings are so typical.1
Caseous calcification of the mitral valve should be considered in the differential diagnosis of cardiac tumors. Such calcification usually carries a benign prognosis, but patients so diagnosed require careful follow-up observation if they develop new symptoms or have a high propensity for tissue calcium deposition (as in chronic renal failure).
Supplementary Material
Footnotes
Address for reprints: Raymond F. Stainback, MD, 6624 Fannin, Suite 2480, Houston, TX 77030 E-mail: rstainback@sleh.com
References
- 1.Harpaz D, Auerbach I, Vered Z, Motro M, Tobar A, Rosenblatt S. Caseous calcification of the mitral annulus: a neglected, unrecognized diagnosis. J Am Soc Echocardiogr 2001;14 (8):825–31. [DOI] [PubMed]
- 2.Teja K, Gibson RS, Nolan SP. Atrial extension of mitral annular calcification mimicking intracardiac tumor. Clin Cardiol 1987;10(9):546–8. [DOI] [PubMed]
- 3.Kautzner J, Vondracek V, Jirasek A, Belohlavek M. Tumor-like mitral annular calcification with central liquefaction. Echocardiography 1993;10:459–63.
- 4.Stone E, Cohn D, Deal C, Pollock C. Calcific atrial mass in end-stage renal failure. Nephrol Dial Transplant 1997;12(4): 807–10. [DOI] [PubMed]
- 5.Borowski A, Korb H, Voth E, de Vivie ER. Asymptomatic myocardial abscess. Thorac Cardiovasc Surg 1988;36(6): 338–40. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.