

Abstract
Many children with cerebral palsy walk in a crouch gait that progressively worsens over time, decreasing walking efficiency and leading to joint degeneration. This study examined the effect of crouched postures on the capacity of muscles to extend the hip and knee joints and the joint flexions induced by gravity during the single limb stance phase of gait. We first characterized representative mild, moderate, and severe crouch gait kinematics based on a large group of subjects with cerebral palsy (N = 316). We then used a three-dimensional model of the musculoskeletal system and its associated equations of motion to determine the effect of these crouched gait postures on (1) the capacity of individual muscles to extend the hip and knee joints, which we defined as the angular accelerations of the joints, towards extension, that resulted from applying a 1 N muscle force to the model, and (2) the angular acceleration of the joints induced by gravity. Our analysis showed that the capacities of almost all the major hip and knee extensors were markedly reduced in a crouched gait posture, with the exception of the hamstrings muscle group, whose extension capacity was maintained in a crouched posture. Crouch gait also increased the flexion accelerations induced by gravity at the hip and knee throughout single limb stance. These findings help explain the increased energy requirements and progressive nature of crouch gait in patients with cerebral palsy.
Keywords: Dynamics, Muscle, Crouch gait, Cerebral palsy, Tibial torsion
INTRODUCTION
Crouch gait, one of the most common gait pathologies in patients with cerebral palsy (Wren et al. 2005), is characterized by increased knee flexion throughout stance phase and, frequently, increased hip flexion and internal rotation. Walking with a crouch gait increases the energy costs of walking (Campbell and Ball 1978; Waters and Lunsford 1985; Rose et al. 1990) and can lead to joint pain and degeneration (Rosenthal and Levine 1977; Lloyd-Roberts et al. 1985; Bleck 1987). Further, without intervention, crouch gait typically worsens over time (Sutherland and Cooper 1978; Bell et al. 2002). A host of possible factors have been linked to the development of crouch gait, including muscle tightness, weakness, and spasticity (Hoffinger et al. 1993; McNee et al. 2004; Arnold et al. 2005), skeletal deformities (Gage and Schwartz 2001), and motor control deficits (Gage and Schwartz 2004). Treatments to improve crouch gait show varying success.
Determining the cause of progressive crouch gait and the appropriate corrective treatment is difficult because the motions generated by muscle forces during crouch gait are not clearly understood. The musculoskeletal system is a complex, multi-joint linkage and, through dynamic coupling, muscles are able to accelerate joints that they do not cross (Zajac and Gordon 1989; Kepple et al. 1997; Riley and Kerrigan 1999; Arnold et al. 2005; Kimmel and Schwartz 2006). Bi-articular muscles may have non-intuitive functions as a result of this dynamic coupling. For example, forces generated by the hamstrings muscle group may produce a knee flexion acceleration through the muscles’ knee flexion moment and may generate knee extension acceleration through the muscles’ hip extension moment (Arnold et al. 2005). Since the joint accelerations that result from a muscle force depend on the relative orientation of the segments of the body, crouched gait postures may reduce the capacity of a muscle to extend the hip or knee (i.e., the joint extension acceleration generated by a 1 N muscle force may decrease).
A link between crouched gait postures and the capacity of muscles to extend the hip and knee has several clinical implications. If a crouched posture significantly reduces the capacity of muscles to extend the hip or knee joints, individuals may be required to exert more muscle force to maintain a crouched posture. Crouch gait may also alter the accelerations of the hip and knee joints that are induced by gravity, further increasing muscle force requirements. Crouch-related changes in muscle extension capacities may help explain differences in muscle activation when walking with a crouch gait (Thomas et al. 1996). For example, muscles that maintain their extension capacity during crouch gait may be favored over muscles with diminished extension capacities. Determining how increasingly severe crouched postures affect the accelerations produced by muscles may help us better understand the progressive nature of crouch gait (Sutherland and Cooper 1978).
The purpose of this study was to determine how crouched postures affect the capacity of muscles to extend the hip and knee joints during the single limb stance phase of gait. We defined a muscle’s extension capacity at the hip or knee joint as the angular acceleration, towards extension, that results from applying a 1 N muscle force to the body along the muscle’s line of action. The muscle’s extension capacity, as we define it, depends solely on the orientation and inertial properties of the body segments and is thus independent of a muscle’s activation level or force-generating capacity. Individuals with crouch gait may have reduced moment-generating capacity of the hip and knee extensors as a result of skeletal deformities, impaired motor control, muscle atrophy, or if muscles operate in suboptimal regions of their force-length curves. However, in this study we examined only the posture-related changes in a muscle’s extension capacity. Since experimentally isolating the effects of a crouched gait posture on muscle extension capacities is difficult, we used musculoskeletal modeling and a dynamic analysis. We first characterized representative crouch gait kinematics, from mild to severe, based on a large database of patients with cerebral palsy. We then determined the effect of these representative crouched postures on the capacity of muscles to extend the hip and knee joints during single limb stance.
METHODS
Representative mild, moderate, and severe crouch gait kinematics were formulated using a database of subjects with cerebral palsy, age 6 or older, who visited the Center for Gait and Motion Analysis at Gillette Children’s Specialty Healthcare, St. Paul, MN. Human subjects approval was obtained from the institutional review boards at Gillette Children’s Specialty Healthcare and Stanford University. A standard clinical protocol was used to place and track the 3D motion of markers on the lower extremity (Davis et al. 1991) and calculate joint angles (Kadaba et al. 1990). All joint angles were normalized to a percent of the gait cycle. Left and right subject sides were analyzed independently. To be included in the study, subjects had to walk with crouch gait, which was defined as a knee flexion angle of at least 20° at initial contact and greater than 15° throughout stance phase, which is approximately 2 SD above normal (Arnold et al. 2006). We did not control for age, surgical history, or level of impairment in order to obtain a general characterization of crouch gait. Subjects with an equinus gait pattern were eliminated from the crouch group by excluding subjects whose average foot-floor angle during single limb stance deviated more than 10° from normal toward equinus.
The subjects were divided into three groups based on crouch severity. Mild crouch subjects had between 20° and 30° of knee flexion at initial contact (N = 89), moderate crouch subjects between 30° and 40° (N = 127), and severe crouch subjects more than 40° (N = 100). Average joint angles for each group were calculated over the entire gait cycle. A comparison set of normal kinematics was determined by averaging gait data for a group of 83 able-bodied children walking at self-selected speed, also collected at Gillette Children’s Specialty Healthcare. Two-sample t-tests were used to compare the joint angles, averaged over the entire gait cycle, between the three crouch groups and normal.
The three-dimensional musculoskeletal model used in our analysis (Figure 1) had 10 segments and 13 degrees of freedom (Delp et al. 1990). The model had a combined head, trunk, and arms segment, a pelvis segment, and a right and left femur, patella, tibia, and foot. The combined upper body segment articulated with the pelvis via a ball and socket joint. The hip joint was modeled as a ball and socket, the articulations of the femur, patella and tibia were modeled as a modified planar joint with one degree of freedom, and the ankle was modeled as a hinge joint. Each of the model’s 92 muscle paths was represented by an origin, insertion, and appropriate wrapping and via points (Delp et al. 1990; Arnold et al. 2000; Anderson and Pandy 2001). The model’s equations of motion were derived using the SIMM Dynamics Pipeline (Delp and Loan 2000) and SD/Fast (Parametric Technologies, Needham, MA).
Figure 1.
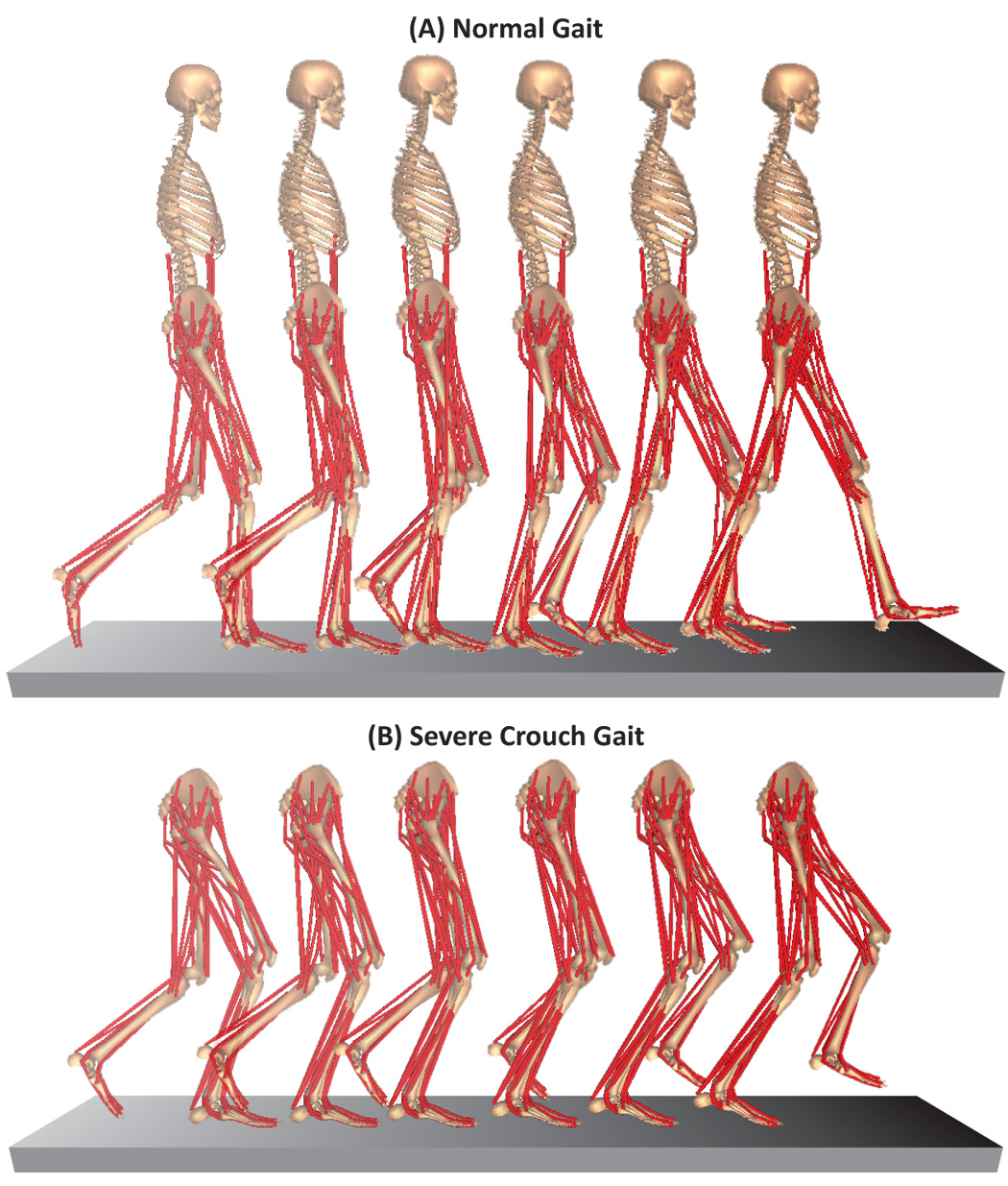
The 3D musculoskeletal model in poses corresponding to single limb stance (14–50% of the gait cycle) for normal gait (A) and severe crouch gait (B). The musculoskeletal model has 10 segments, 13 degrees of freedom, and 92 muscle paths. Although an upper body segment was included in our analysis of crouch gait, it is omitted from the figure. We assumed normal trunk kinematics in the crouch groups since upper body motion data was not available for most subjects with crouch gait.
To quantify the effect of crouch gait on the extension capacity of muscles and the action of gravity at the hip and knee, we used an induced acceleration analysis (Zajac and Gordon 1989). We positioned the musculoskeletal model with the averaged gait kinematics for each of the four groups—normal, mild crouch, moderate crouch, and severe crouch (Figure 1) during the single limb stance phase (14–50%). For each muscle path in the model, at every 2% of single limb stance, a 1 N muscle force and the corresponding ground reaction force were applied to the model, in isolation. The resulting angular accelerations of the hip and knee joints were then calculated using the model’s equations of motion. These accelerations represent the capacity of each muscle to extend the hip and knee joints per unit force, for each position of single limb stance. For muscles represented by more than one path, extension capacities were calculated by taking a weighted average based on the maximum isometric force of each component. To determine the hip and knee angular accelerations induced by gravity throughout single limb stance, we applied a gravitational force to the center of mass of each model segment as well as the corresponding ground reaction force at the foot.
We used an optimization approach (Anderson and Pandy 2003) to calculate the ground reaction force corresponding to an individual unit muscle force or gravity. A set of five contact points were distributed on the sole of the stance foot. After applying a 1 N muscle force or gravity, we determined the force needed at each contact point to maintain zero acceleration of the foot. A sequential quadratic programming algorithm (CFSQP, AEM Design, Tucker, GA) was used to solve for the distribution of forces that minimized the sum of squared forces at the five contact points while maintaining rigid contact between the foot and the ground.
RESULTS
The crouch gait subjects had significantly larger knee flexion angles than normal during stance, by definition (Figure 2C). Subjects in each crouch group also had larger hip flexion (Figure 2B) and internal rotation (Figure 2E) than normal, when averaged over the gait cycle (p<0.05). Our elimination of subjects with an equinus gait pattern resulted in progressively greater dorsiflexion (p<0.05) in each crouch group (Figure 2D). Subjects with crouch gait also tended to walk with more anterior pelvic tilt and external foot progression than normal, although group differences were not significant (Figures 2A and 2F). The full kinematics profiles for each group and videos of animated models are available as an online supplement (Appendix A).
Figure 2.
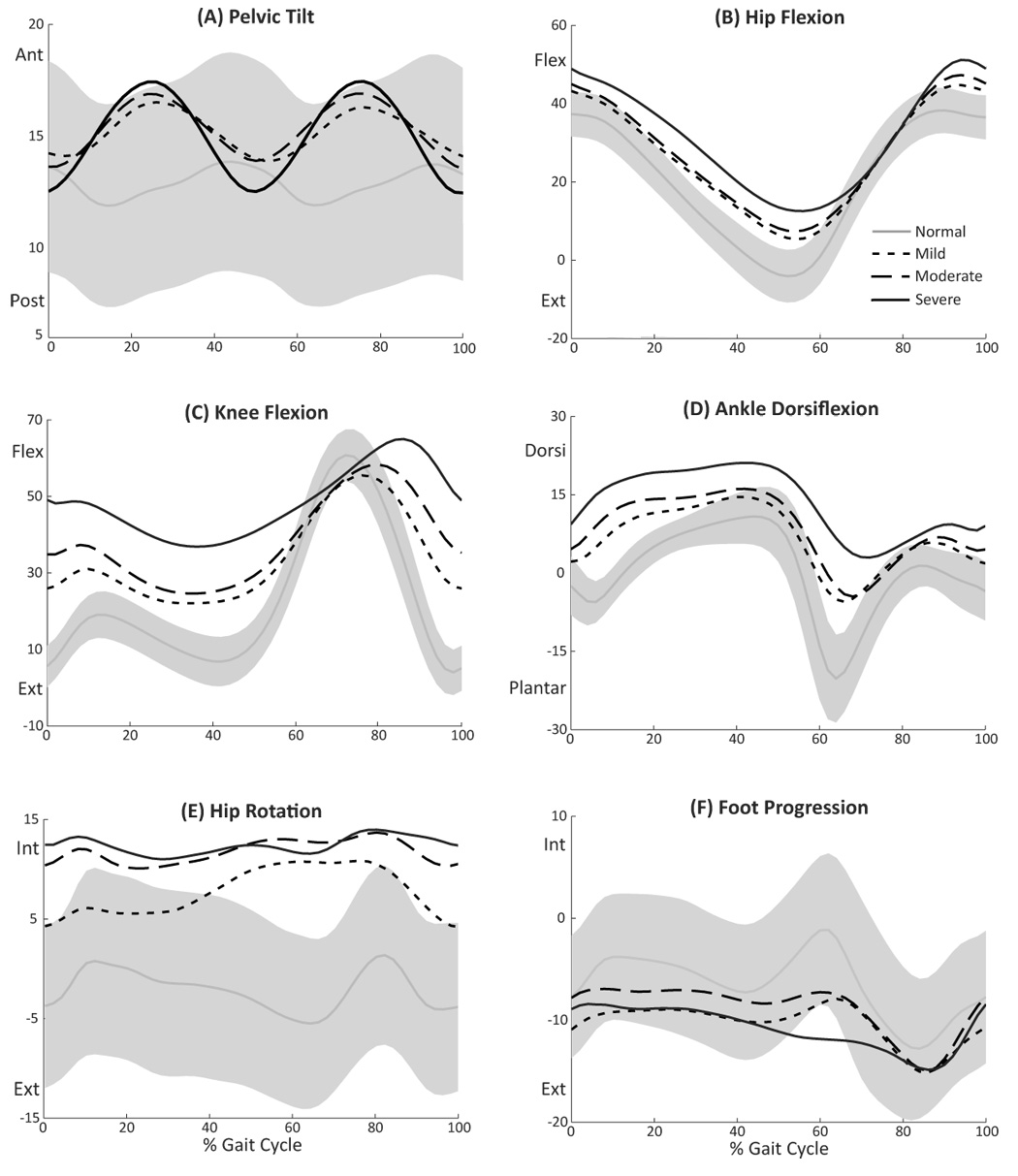
Average joint kinematics for normal and crouch gait. The gray line and bands show the mean values ±1 SD for a group of 83 able-bodied children walking at self-selected speed. The black solid and dashed lines show mean kinematics for subjects with cerebral palsy who walked in a crouch gait, classified as mild (N = 89), moderate (N = 127), or severe (N = 100) based on knee flexion angle at initial contact. All angles are in degrees. The three crouch groups had significantly greater than normal hip flexion (B), knee flexion (C), ankle dorsiflexion (D), and internal hip rotation (E) when averaged over the gait cycle (p<0.05). Anterior pelvic tilt (A) and external foot progression (F) tended to be larger in the crouch groups, but were not significantly different from normal.
Crouched gait postures reduced the capacity of muscles in our model to generate extension accelerations at the hip and knee. The gluteus maximus, posterior gluteus medius, vasti, and soleus all had a substantial capacity to extend the hip and knee joints during normal single limb stance (Figure 3). With crouch gait, the capacities of all of these muscles to extend the joints were markedly reduced. At the hip, the extension capacities of posterior gluteus medius, soleus, and vasti were all less than 50% of normal, for a severe crouch (Figure 3A). At the knee, the capacities of soleus, vasti, and gluteus maximus were less than 50% of normal while the posterior gluteus medius lost nearly all knee extension capacity with severe crouch (Figure 3B). The rectus femoris had a knee extension capacity in normal gait, which was completely lost with severe crouch (Figure 3B). The effect of crouch gait on the extension capacities of these muscles was consistent throughout single limb stance. The effect of crouch gait on the capacity of all muscles in the model to extend the hip and knee is available as an online supplement (Appendix A). In normal gait, the hamstrings in our model had a large hip extension capacity and a small knee extension capacity (Figure 4). With crouch gait, at the hip, we observed an increase in the extension capacity of the hamstrings, especially in the second half of single limb stance. At the knee, there was a slight decrease in the extension capacity of hamstrings in early stance with crouch gait, while in late single limb stance there was an increase.
Figure 3.
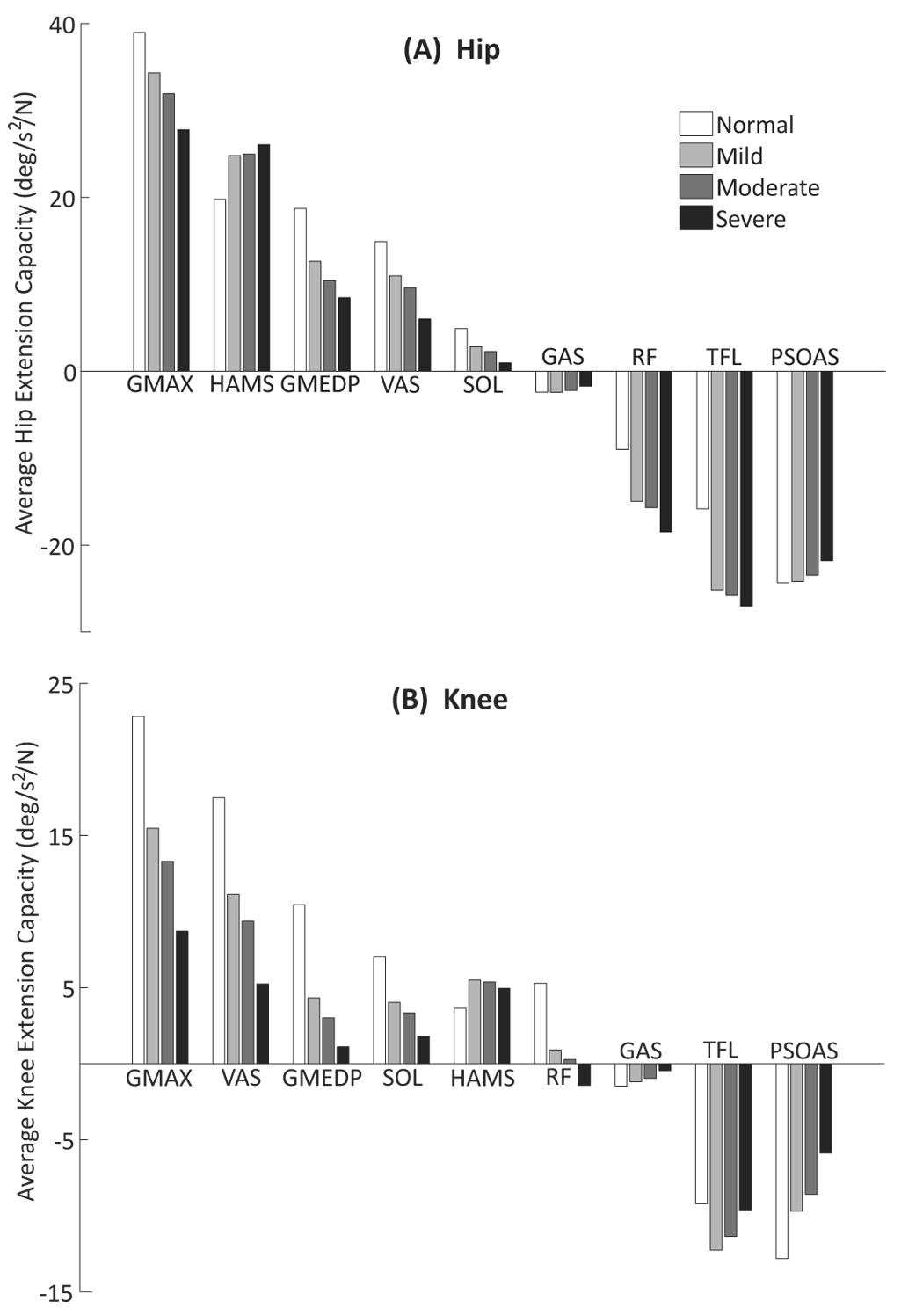
The effect of crouch gait on the capacity of muscles to extend the hip (A) and knee (B). Each bar graph shows the capacity of the major leg muscles to accelerate the hip and knee joints per 1 N muscle force, averaged over the single limb stance period, for normal and crouch gait. Darker shades of gray represent more severe crouch. Extension capacities are positive. The muscles shown include gluteus maximus (GMAX), hamstrings (HAMS), the posterior compartment of gluteus medius (GMEDP), vasti (VAS), soleus (SOL), gastrocnemius (GAS), rectus femoris (RF), tensor fascia latae (TFL), and psoas (PSOAS). Results for the other muscles in the model are available as an online supplement (Appendix A).
Figure 4.
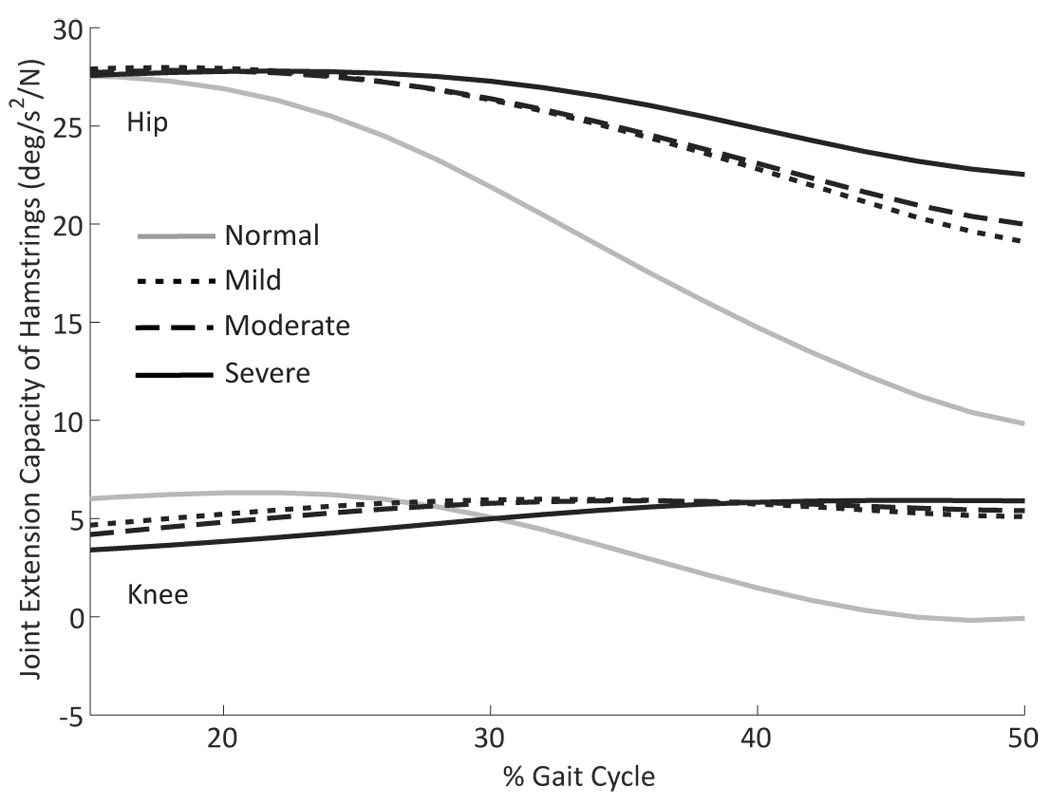
The effect of crouch gait on the capacity of the hamstrings to extend the hip and knee, throughout single limb stance, for normal gait and for mild, moderate, and severe crouch gait.
Crouch gait also influenced some of the hip and knee flexor muscles. At the hip joint, crouch gait had little effect on the psoas, but increased the capacity of both rectus femoris and tensor fascia latae to generate flexion accelerations at the hip (Figure 3A). At the knee joint, the tensor fascia latae showed a slight increase in flexion capacity with crouch gait, while the psoas showed a decrease in flexion capacity (Figure 3B).
In normal gait, gravity accelerated the hip towards flexion in the first half of single limb stance and towards extension in the second half (Figure 5A). Gravity acted to flex the knee throughout normal single limb stance, with a decreasing magnitude as stance progressed (Figure 5B). In crouch gait, gravity instead had a flexion action at both joints, throughout single limb stance, increasing the demands on muscles.
Figure 5.
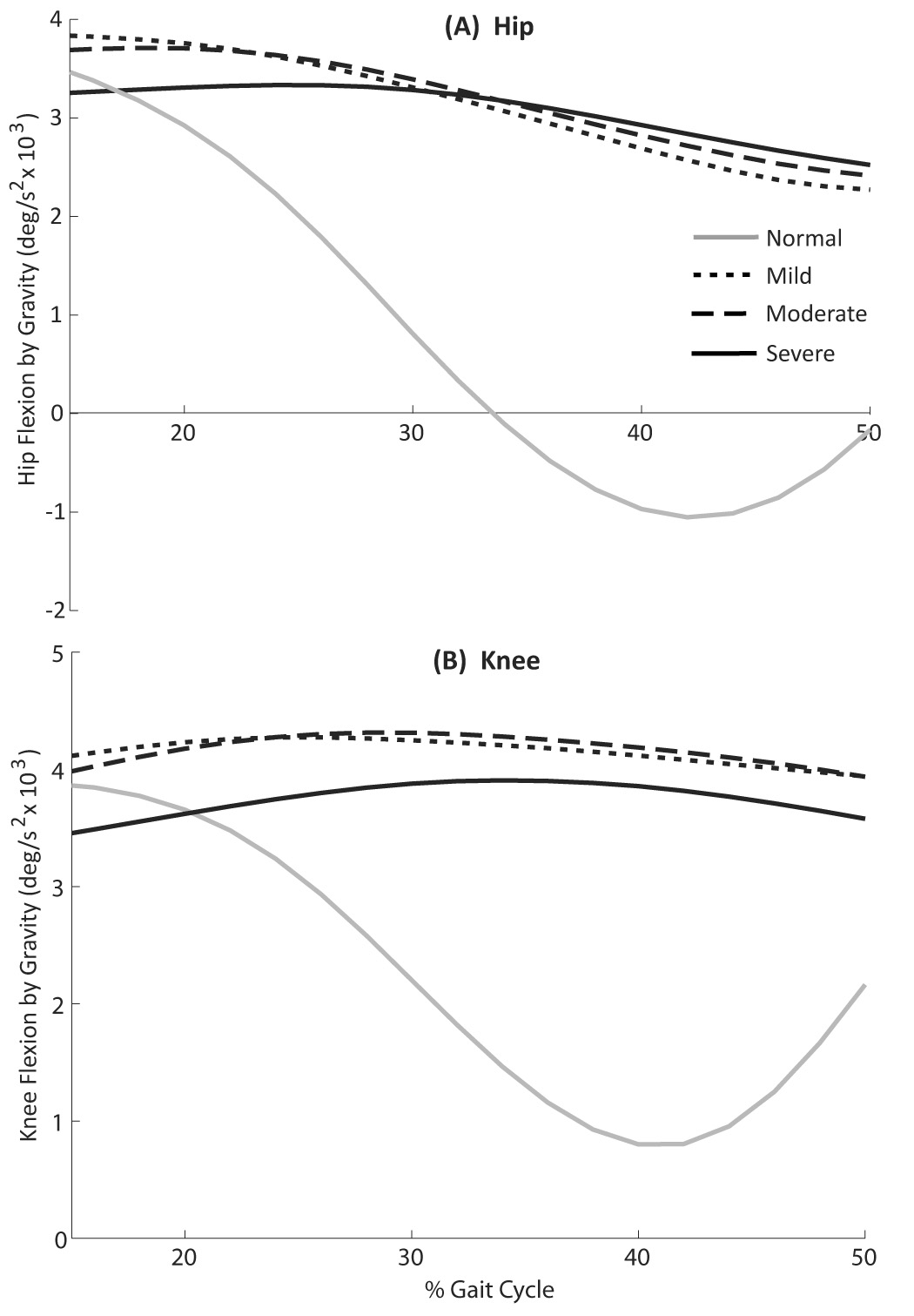
The effect of crouch gait on the flexion accelerations induced by gravity at the hip (A) and knee (B) vs. the gait cycle for normal gait and for mild, moderate, and severe crouch gait. Flexion acceleration is positive.
DISCUSSION
This study examined the effect of crouched gait postures on the capacity of muscles to generate extension accelerations at the hip and knee during single limb stance. We found that a crouched posture, which changes the relative orientation of the body segments and thus alters dynamic coupling between joints, led to major reductions in the hip and knee extension accelerations generated by several important stance-phase muscles. Gluteus maximus, posterior gluteus medius, vasti, and soleus all showed reduced extension capacities for mild, moderate, and severe crouch gait—reductions that are independent of muscle activation and the physiological ability of the muscle to generate force.
In a crouched posture, the joint flexion accelerations induced by gravity increase and the capacity of muscles to generate joint extension acclereations decrease, so an individual in a crouch gait must generate more muscle force to maintain a crouched posture. This increase in required muscle force is consistent with experimental studies that show greater muscle activity in flexed postures (Hsu et al. 1993) and reports of increased energy expenditure for crouch gait (Rose et al. 1990; Waters and Mulroy 1999). Larger muscle forces also increase joint loading, a likely contributor to knee abnormalities, like patella alta, observed in patients who walk with crouch gait for extended time periods (Rosenthal and Levine 1977; Lloyd-Roberts et al. 1985). The progressive reduction in muscle extension capacities with increasing crouch severity suggests that subjects may enter a downward cycle once they start to develop crouch, as observed in clinical settings (Sutherland and Cooper 1978; Bell et al. 2002).
Extended hamstrings activation into mid- and late-stance is commonly observed in individuals with crouch gait (Hoffinger et al. 1993). While this hamstrings over-activity is believed to cause the excess knee flexion associated with crouch gait, the results of our analysis suggest that, for some patients, increased hamstrings activation during single limb stance may instead be a compensation for crouch gait. Patients walking in a crouched posture may increase activation of the hamstrings during single support since the capacity of this muscle group to accelerate the hip and knee toward extension is maintained in crouched postures. Over time, this hamstrings over-activity would likely lead to muscle remodeling and tightness, further feeding the downward cycle of crouch gait. We emphasize that the change in joint extension capacities with crouched gait postures is only one possible component of the set of factors that may lead to progressively worsening crouch gait. Muscle weakness and spasticity, joint contractures, bony deformities, and motor control deficits, in addition to changes in muscle extension capacities that result from a crouched posture, are all interacting factors that may contribute to crouch gait. More investigation is needed to determine why patients initially develop a crouch gait pattern, despite its detrimental effect on the capacity of muscles to extend the joints.
We previously demonstrated that excess tibial torsion, a common skeletal deformity in patients with crouch gait, reduces the capacity of the soleus and gluteal muscles to extend the hip and knee at body positions corresponding to the single limb stance phase of normal gait (Hicks et al. 2007). The impact of a tibial deformity when walking in a crouched posture has not been determined. Using our previously-developed technique to simulate torsional bone deformities, we created a set of musculoskeletal models with a range of tibial torsion angles and positioned each of these deformed models with moderate crouch gait single limb stance kinematics. We determined the additional reduction in average muscle extension capacities during single limb stance as a result of tibial torsion and compared these results to the trends observed with normal gait. Tibial torsion had a similar effect for both normal and moderate crouch gait, reducing the hip and knee extension accelerations generated by several important stance phase muscles, particularly the gluteal muscles and soleus (Figure 6). These findings suggest that tibial deformities may be problematic in subjects with crouch gait, as their muscle extension capacities are already substantially reduced.
Figure 6.
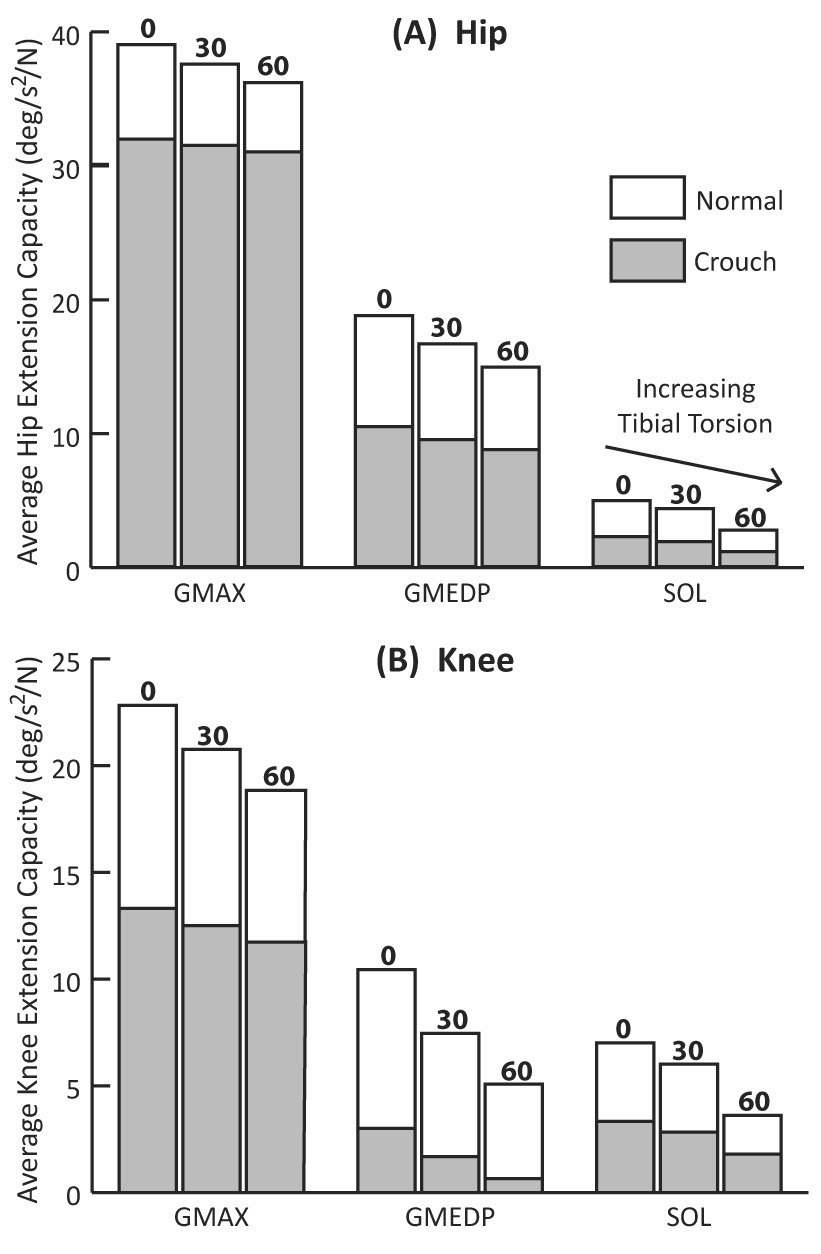
The effect of tibial torsion on the capacity of muscles to extend the hip (A) and knee (B) in normal and moderate crouch gait during single limb stance. The muscles shown, including gluteus maximus (GMAX), the posterior compartment of gluteus medius (GMEDP), and soleus (SOL), are the stance phase extensor muscles that are substantially affected by tibial torsion (Hicks et al. 2007). The solid white bars show the average extension capacity during normal single limb stance for each muscle in a model with 0°, 30°, and 60° of tibial torsion. The grey bars show the average extension capacity during moderate crouch gait single limb stance, for a model with 0°, 30°, and 60° of tibial torsion.
Although the gait kinematics of subjects within each crouch group were generally consistent, the walking patterns of individuals with crouch gait can be variable. For example, the crouch subjects exhibited mean anterior pelvic tilt angles ranging from approximately 0° to 30°. To test the sensitivity of our results to pelvic tilt, we further divided each crouch severity group into mild, moderate, and severe anterior pelvic tilt groups, creating nine sets of averaged crouch gait kinematics. At each crouch severity level, increasing the amount of pelvic tilt led to a further decrease in muscle extension capacities. Hence, for a given crouch severity, a subject with severe anterior pelvic tilt may have larger reductions in extension capacity than a subject with pelvic kinematics closer to normal. We also assumed normal trunk kinematics in our analysis, which may not accurately represent the commonly observed forward trunk lean in patients with crouch gait. We tested adding an artificial forward lean to the crouch gait kinematics, which did not substantially change the results.
In this study, we only analyzed the capacity of a muscle to generate extension accelerations at the hip or knee. The actual angular acceleration induced by a particular muscle also depends on the muscle’s activation level and physiological ability to generate force. For the bi-articular muscles like hamstrings and rectus femoris, our calculations are sensitive to the ratio of the muscles’ moment arms at the hip and knee, so the results for these muscles must be interpreted with the caution that these ratios may vary from subject to subject.
Our analysis was limited to the single limb stance phase of gait, since obtaining a continuous estimate of the ground reaction force component for each muscle required that the foot had zero acceleration (i.e., was in rigid contact with the ground). However, the single limb support phase is of particular clinical importance, since the generation of excess knee flexion accelerations during single support is thought to be one of the major contributors to crouch gait. Further research is warranted to investigate how a crouched posture may affect muscles in terminal swing and early stance, thus altering the initial conditions for single support.
We have demonstrated that crouch gait reduces the capacity of several important stance phase muscles to extend the hip and knee joints. As a consequence, muscles must work harder to maintain a given limb position, which helps to explain the increase in energy expenditure when walking in a crouched posture. The negative impact of this pathological gait pattern increases with worsening crouch severity, which suggests that crouch gait is a downward cycle, a commonly observed clinical phenomenon. More optimistically, the findings of this study suggest that small improvements in gait posture, as a result of physical therapy or surgery, may help to reverse this process. For example, if correcting a patient’s tibial alignment leads to a small improvement in the capacity of the subject’s muscles to extend the joints, it may lead to a more erect posture, and thus further improvement in muscle extension capacities, perhaps reversing the downward cycle. In addition, the dynamic analysis used in this study could be adapted to analyze the gait kinematics and bone geometry of individual patients. Such quantitative analyses may help to identify candidates who would benefit from targeted strength training or from surgery to correct bony malalignment.
Supplementary Material
{kind=link}
ACKNOWLEDGMENTS
The authors thank the staff of the Center for Gait and Motion Analysis at Gillette Children’s Specialty Healthcare for collection of the subject data and Clay Anderson for providing technical guidance. This work was funded by the National Institutes of Health through the NIH Roadmap for Medical Research, Grant U54GM072970 and through NIH Grants HD33929 and HD046814. Support was also provided by the National Science Foundation and Stanford’s Bio-X program.
Appendix
APPENDIX A: SUPPLEMENTARY MATERIAL
Supplementary data associated with this article can be found in the online version at doi:___________.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- Anderson FC, Pandy MG. Dynamic optimization of human walking. Journal of Biomechanical Engineering. 2001;123:381–390. doi: 10.1115/1.1392310. [DOI] [PubMed] [Google Scholar]
- Anderson FC, Pandy MG. Individual muscle contributions to support in normal walking. Gait and Posture. 2003;17:159–169. doi: 10.1016/s0966-6362(02)00073-5. [DOI] [PubMed] [Google Scholar]
- Arnold AS, Anderson FC, Pandy MG, Delp SL. Muscular contributions to hip and knee extension during the single limb stance phase of normal gait: a framework for investigating the causes of crouch gait. Journal of Biomechanics. 2005;38:2181–2189. doi: 10.1016/j.jbiomech.2004.09.036. [DOI] [PubMed] [Google Scholar]
- Arnold AS, Liu MQ, Schwartz MH, Ounpuu S, Dias LS, Delp SL. Do the hamstrings operate at increased muscle-tendon lengths and velocities after surgical lengthening? Journal of Biomechanics. 2006;39:1498–1506. doi: 10.1016/j.jbiomech.2005.03.026. [DOI] [PubMed] [Google Scholar]
- Arnold AS, Salinas S, Asakawa DJ, Delp SL. Accuracy of muscle moment arms estimated from MRI-based musculoskeletal models of the lower extremity. Computer Aided Surgery. 2000;5:108–119. doi: 10.1002/1097-0150(2000)5:2<108::AID-IGS5>3.0.CO;2-2. [DOI] [PubMed] [Google Scholar]
- Bell KJ, Ounpuu S, DeLuca PA, Romness MJ. Natural progression of gait in children with cerebral palsy. Journal of Pediatric Orthopaedics. 2002;22:677–682. [PubMed] [Google Scholar]
- Bleck EE. Orthopaedic Management in Cerebral Palsy. London: Mac Keith Press; 1987. [Google Scholar]
- Campbell J, Ball J. Energetics of walking in cerebral palsy. Orthopedic Clinics of North America. 1978;9:374–377. [PubMed] [Google Scholar]
- Davis RB, Ounpuu S, Tyburski D, Gage JR. A gait analysis data collection and reduction technique. Human Movement Science. 1991;10:171–178. [Google Scholar]
- Delp SL, Loan JP. A computational framework for simulation and analysis of human and animal movement. IEEE Computing in Science and Engineering; 2000. pp. 46–55. [Google Scholar]
- Delp SL, Loan JP, Hoy MG, Zajac FE, Topp EL, Rosen JM. An interactive graphics-based model of the lower extremity to study orthopaedic surgical procedures. IEEE Transactions on Biomedical Engineering; 1990. pp. 757–767. [DOI] [PubMed] [Google Scholar]
- Gage JR, Schwartz MH. Dynamic deformities and lever arm considerations. In: Paley D, editor. Principles of Deformity. Berlin: Springer; 2001. pp. 761–775. [Google Scholar]
- Gage JR, Schwartz MH. Pathological gait and lever-arm dysfunction. In: Gage JR, editor. The Treatment of Gait Problems in Cerebral Palsy. London: Mac Keith Press; 2004. pp. 180–204. [Google Scholar]
- Hicks J, Arnold A, Anderson F, Schwartz M, Delp S. The effect of excessive tibial torsion on the capacity of muscles to extend the hip and knee during single-limb stance. Gait and Posture. 2007;26:546–552. doi: 10.1016/j.gaitpost.2006.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoffinger SA, Rab GT, Abou-Ghaida H. Hamstrings in cerebral palsy crouch gait. Journal of Pediatric Orthopaedics. 1993;13:722–726. doi: 10.1097/01241398-199311000-00006. [DOI] [PubMed] [Google Scholar]
- Hsu AT, Perry J, Gronley JK, Hislop HJ. Quadriceps force and myoelectric activity during flexed knee stance. Clinical Orthopaedics and Related Research. 1993:254–262. [PubMed] [Google Scholar]
- Kadaba MP, Ramakrishnan HK, Wootten ME. Measurement of lower extremity kinematics during level walking. Journal of Orthopaedic Research. 1990;8:383–392. doi: 10.1002/jor.1100080310. [DOI] [PubMed] [Google Scholar]
- Kepple TM, Siegel KL, Stanhope SJ. Relative contributions of the lower extremity joint moments to forward progression and support during gait. Gait and Posture. 1997;6:1–8. [Google Scholar]
- Kimmel SA, Schwartz MH. A baseline of dynamic muscle function during gait. Gait and Posture. 2006;23:211–221. doi: 10.1016/j.gaitpost.2005.02.004. [DOI] [PubMed] [Google Scholar]
- Lloyd-Roberts GC, Jackson AM, Albert JS. Avulsion of the distal pole of the patella in cerebral palsy. A cause of deteriorating gait. Journal of Bone and Joint Surgery [Br] 1985;67:252–254. doi: 10.1302/0301-620X.67B2.3980536. [DOI] [PubMed] [Google Scholar]
- McNee AE, Shortland AP, Eve LC, Robinson RO, Gough M. Lower limb extensor moments in children with spastic diplegic cerebral palsy. Gait and Posture. 2004;20:171–176. doi: 10.1016/j.gaitpost.2003.08.009. [DOI] [PubMed] [Google Scholar]
- Riley PO, Kerrigan DC. Kinetics of stiff-legged gait: induced acceleration analysis. IEEE Transactions on Rehabilitation Engineering; 1999. pp. 420–426. [DOI] [PubMed] [Google Scholar]
- Rose J, Gamble JG, Burgos A, Medeiros J, Haskell WL. Energy expenditure index of walking for normal children and for children with cerebral palsy. Developmental Medicine and Child Neurology. 1990;32:333–340. doi: 10.1111/j.1469-8749.1990.tb16945.x. [DOI] [PubMed] [Google Scholar]
- Rosenthal RK, Levine DB. Fragmentation of the distal pole of the patella in spastic cerebral palsy. Journal of Bone and Joint Surgery [Am] 1977;59:934–939. [PubMed] [Google Scholar]
- Sutherland DH, Cooper L. The pathomechanics of progressive crouch gait in spastic diplegia. Orthopedic Clinics of North America. 1978;9:143–154. [PubMed] [Google Scholar]
- Thomas SS, Moore C, Kelp-Lenane C, Norris C. Simulated gait patterns: the resulting effects on gait parameters, dynamic electromyography, joint moments, and physiological cost index. Gait and Posture. 1996;4:100–107. [Google Scholar]
- Waters RL, Lunsford BR. Atlas of Orthotics. St. Louis: C.V. Mosby Co.; 1985. Energy expenditure of normal and pathological gait: application to orthotic prescription; pp. 151–159. [Google Scholar]
- Waters RL, Mulroy S. The energy expenditure of normal and pathologic gait. Gait and Posture. 1999;9:207–231. doi: 10.1016/s0966-6362(99)00009-0. [DOI] [PubMed] [Google Scholar]
- Wren TA, Rethlefsen S, Kay RM. Prevalence of specific gait abnormalities in children with cerebral palsy: influence of cerebral palsy subtype, age, and previous surgery. Journal of Pediatric Orthopaedics. 2005;25:79–83. doi: 10.1097/00004694-200501000-00018. [DOI] [PubMed] [Google Scholar]
- Zajac FE, Gordon ME. Determining muscle's force and action in multi-articular movement. Exercise and Sport Sciences Reviews. 1989;17:187–230. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.