

Abstract
Objective
To present a novel examination of how error cascades are stopped (ameliorated) before they affect patients.
Design
Qualitative analysis of reported errors in primary care.
Setting
Over a three‐year period, clinicians and staff in two practice‐based research networks voluntarily reported medical errors to a primary care patient safety reporting system, Applied Strategies for Improving Patient Safety (ASIPS). The authors found a number of reports where the error was corrected before it had an adverse impact on the patient.
Results
Of 754 codeable reported events, 60 were classified as ameliorated events. In these events, a participant stopped the progression of the event before it reached or affected the patient. Ameliorators included doctors, nurses, pharmacists, diagnostic laboratories and office staff. Additionally, patients or family members may be ameliorators by recognising the error and taking action. Ameliorating an event after an initial error requires an opportunity to catch the error by systems, chance or attentiveness. Correcting the error before it affects the patient requires action either directed by protocols and systems or by vigilance, power to change course and perseverance on the part of the ameliorator.
Conclusion
Despite numerous individual and systematic methods to prevent errors, a system to prevent all potential errors is not feasible. However, a more pervasive culture of safety that builds on simple acts in addition to more costly and complex electronic systems may improve patient outcomes. Medical staff and patients who are encouraged to be vigilant, ask questions and seek solutions may correct otherwise inevitable wrongs.
Growing attention given to patient safety and quality improvement in ambulatory care settings has led to a better understanding of common medical errors in practice, potential solutions and areas of further investigation.1,2,3,4,5,6,7 Although such studies advance our understanding of what can go wrong and suggest where to intervene for better safety and quality, we know little about what goes right after something goes wrong. The cascade of events2,8 can lead to an adverse outcome or may be interrupted at any point along the course of the error event. Root cause analysis of reported near‐miss events typically attempts to understand how upstream conditions contribute to downstream consequences. In medicine, as in other industries such as aviation, this approach is one piece of a major effort to change the culture around errors.9,10,11 This culture of safety has been described as an “ability to entertain doubt, to develop a questioning attitude, and to respect the legitimacy of others' viewpoints”.12
In contrast to the upstream approach, our analysis looks downstream from the initial error to understand how people interrupted errors to make them near misses. Although a few researchers have begun investigating these “recoveries” in hospital settings,13,14 we are not aware of any published accounts of these events in the ambulatory care setting. This manuscript describes our findings from an exploratory qualitative analysis of these ameliorated cases.
Methods
Applied Strategies for Improving Patient Safety (ASIPS) was a three‐year demonstration project designed to collect and analyse medical error reports from primary care practices in two practice‐based research networks: the Colorado Research Network (CaReNet) and the High Plains Research Network. Because our reporting system encouraged reporting of errors even when there was no known patient harm, we were able to characterise errors that were caught and corrected before they had any impact on the patient. The core of the ASIPS patient safety reporting system was a web‐based data collection and data management system. The dataset includes the text of the narrative description of the event submitted by the reporter of the event. The study encouraged wide participation from all clinical and non‐clinical personnel.
Participants were asked to report “any event you don't wish to have happen again that might represent a threat to patient safety”. This definition included events associated with clinical judgment and knowledge, administrative procedures, and threats from close calls and near misses where no patient harm occurred. Because of this, we were able to identify critical incidents that did not result in patient harm or might not be considered errors or even near misses. More detail on the reporting system, taxonomic coding and our broader analytical methods have been published previously.1,15,16,17,18
The ASIPS taxonomy defined an ameliorator as “a participant whose contribution to an event was positive and stopped the progression of the event before it reached or affected the patient”.19 This included stopping errors or preventing future potential errors, but did not include remedial action after a patient was already affected or that required treatment resulting from the error. Importantly, this subset of near‐miss events specifically required the active contribution of a participant identified in the event. Other near‐miss events that lacked this were not classified as ameliorated events; for example, an automated system that detected dosing errors or drug interactions in which the role of the healthcare professional is largely passive. Elsewhere, ameliorated events have been described as error recovery.13,14 For this analysis, we examined in detail events that were previously identified as ameliorated events using the ASIPS taxonomy.
Our qualitative analysis was designed to identify more than just the steps in an error cascade.2 We specifically wanted examine a subset of near‐miss cases to identify and understand possible patterns in how errors are detected and by whom, who is involved in ameliorating errors, what they did and other contextual factors. This is similar to methods described by Kanse et al in a study on error recovery in a hospital pharmacy.13
The use of both editing and template coding approaches20 allowed us to explore emergent concepts, then review each case again to code for specific concepts of interest, and then review again to consider alternative explanations or to address disagreements in coding or interpretation. A clinician (BP) first reviewed 20 previously identified ameliorator cases to generate an initial list of codes for use by our analysis team (editing style). This initial code list appears in table 1.
Table 1 Initial code list for analysis of event report text.
| Domain | Code | Definition |
|---|---|---|
| I Who: Who was/were the ameliorator/s (can code multiple, if needed) | 1: Patient/Patient‐Related | Patient, family member, patient representative |
| 2: Clinician | Physician, physician's assistant, nurse practitioner | |
| 3: Nurse | RN, MA, LPN | |
| 4: Office staff | Front office staff, billing, administration, or medical records | |
| 5: Lab or lab personnel | Laboratory technician | |
| 6: Pharmacy or pharmacist | Pharmacist, pharmacy technician | |
| 7: Radiology/radiology tech | Radiologists, radiology technician | |
| 8: Other | Any other person not in the above categories | |
| II What: (a) Was the amelioration expected, typical action; OR unexpected above and beyond. If patient was the ameliorator, no code needed. | A: Most people, most times | Most people, most of the time would take this action; it would be expected for most people to do this under the event circumstances. |
| B: Over and above | The action taken is exceptional and goes above and beyond what would normally expect (“Wow! I didn't expect that”) | |
| C: Insufficient information | Use to indicate there seems to be insufficient information to code the event in this domain. | |
| III What: (b) What exactly did the ameliorator do (eg, phone call, double‐check, asked questions, etc) | [open code or in vivo code] | Descriptive codes to get a sense of types of things people do when they ameliorate (eg, phone call, asked extra questions, double‐checked, actually followed protocol) |
| IV When: At what point in the process (ie, the entire loop for an event procedure or activity) did the amelioration occur? | PRE | Amelioration took place before event process started (eg, system change to prevent a future error; corrected medical record to prevent future error) |
| EARLY | Amelioration took place early in the event process (eg, MD noticed wrote wrong dose on Rx and corrected before patient left) | |
| MID | Amelioration took place in middle of process (eg, pharmacy noticed dose was wrong, clarified with clinic, then dispensed correctly) | |
| LATE | Amelioration took place late in event process (eg, patient noticed that dispense pills were different and clarified before taking) | |
| V. System change? | SYSTEM | Use to indicate a change made to system or protocol or practice (ie, implemented an office‐wide change), either as a part of the amelioration or as a result of the event |
Three clinician/non‐clinician pairs familiar with the ASIPS project then each coded 20 events (so all 60 events were coded) using the initial code list. We encouraged open or in vivo coding to determine what the ameliorator actually did and to identify other emerging themes (editing and template coding). All coders then met to discuss discrepancies in coding and other emergent ideas. Two team members (BP, DF) then reviewed and coded all the cases again (template coding), coding for how moments of amelioration were detected and how action was initiated, yet remaining open to other themes or issues. Our coding was further refined to group cases in terms of detection and correction of errors by ameliorators. Finally, we calculated frequencies for types of reporters and ameliorators to help characterise the data. We present verbatim excerpts from the error reports to help illustrate our findings. The study protocol has been approved by the Colorado Multiple Institutional Review Board (COMIRB) and the institutional review boards of practices not covered by COMIRB.
Results
Of 754 coded events voluntarily reported to the ASIPS reporting system, 60 were previously coded as ameliorated events (fig 1). Those involved with the direct clinical care of patients—clinicians and nurses—submitted the vast majority of ameliorated cases (83%), and this same group combined with pharmacists were most likely to be ameliorators (table 2). Patients or family members were ameliorators in 15% of the cases. To understand how events are ameliorated, our re‐examination of the report text suggested two necessary components: detection of the error (that is, the opportunity to notice something is not correct) and action taken to correct the error (that is, acting on the dissonant information). The amelioration of an error appears to begin with three types of detection: system, chance or diligence.

Figure 1 Data selection for in‐depth analysis.
Table 2 Identification of ameliorators.
| Ameliorator type | n (%) |
|---|---|
| MD, DO, PA, NP | 17 (28) |
| RN, LPN, MA, lab tech (in clinic) | 13 (21) |
| Office staff* | 6 (10) |
| Lab or lab personnel (facility outside of clinic) | 2 (3) |
| Pharmacist (facility outside of clinic) | 10 (16) |
| Patient/family member | 9 (15) |
| Unknown | 3 (5) |
*Office staff: front office, billing or administrative staff, medical records personnel.
Examples of system detection include cases where established protocols systematically review certain information or processes, such as pharmacy error checking algorithms, or review procedures for known problems based on past experience:
“Patient was given a written prescription in which the dosage was unclear. The pharmacy called the clinic to clarify.”
Our analysis also points to chance detections that occur when a person “just happened to notice” something that was clearly amiss:
“Patient message for a doctor on vacation was left in his box despite a note covering the box stating that he/she was gone for 2 weeks. I happened to see it and called patient; turned out she had been expecting a call back for a over a week.”
“After drawing up the shots, I happened to glance at the back of the chart and found a previous immunization record that the doctor didn't know about. Luckily it was caught early and the child did not have to have any vaccines.”
Finally, our analysis points to detections that occur when dissonant or conflicting information is subtle or minor. In spite of this, the ameliorator chooses to investigate the situation further (diligence). For example, this case of triple‐checking a mislabeled x ray:
“Left hip xray ordered by MD [entire pelvis was shot so right and left hip were visible]. After film developed MD questioned if film labeled correctly [because abnormality was seen on the xray and was also the same side that the pain was on, however this side did not correspond to the side that the patient was complaining about]. [xray got shot again] Second view labeled the same as the first. MD stated: “What are the chances both films are labeled wrong?” MD decided xray finding was on right hip and discharged pt. Advised MD I could not be positive films labeled correctly and would like to re‐xray. Pt. re‐xrayed [still in clinic, didn't have to come back]. Films indeed labeled incorrectly, pt. and MD changed discharge instructions for Tx of fx.”
However, the detection of the error does not necessarily lead to corrective action. There appear to be two primary motivators for action: protocols versus vigilance/attentiveness. Protocols specifically tell the ameliorator to take action and what the action is. For example, pharmacy systems prompt the pharmacist to clarify a prescription or an office protocol directs the event discoverer to double‐check or review charts:
“MD signed off on urine test results of pregnant patient without treating patient. Urine culture was positive E coli>40,000 CFU. [UA was part of initial UA pregnancy screenings. An LPN who is responsible for all OB patients was going through the charts and noticed this error. She approached the reporter (not the same MD as in the event) and asked what to do.] There was a 2 week delay in antibiotic therapy. The patient was fine but she could have the potential of having a miscarriage during this timeframe.”
In other cases, the error is corrected in the absence of system prompts directing action, due to the vigilance and attentiveness of the ameliorator. This may reflect characteristics of individual people, past experience or training. For example, patients who have experienced medication prescribing or dispensing errors become more alert and always check.
“Wife of a 64 year old male patient picked up his Aricept for dementia and noticed when she got home that it looked different than before. She returned to the pharmacy and discovered that he had been given Aciphex (for stomach acid). This was a refill of an existing prescription so there was no error from the doc's office to the pharmacy. They apologized and corrected the problem. This same person was talking with her mother, who takes a number of medications and is also my patient. Her mother told her that she finds an incorrectly filled prescription (almost all from refills) several times a year and takes them back.”
“Phone messages that were taken shortly before 5:00 … The phone person answers these calls. One call was from a woman with tingling lips and was light headed. The phone person took the message from the woman with the tingling lips and told her that she probably wouldn't be getting a call back today because it was after 5pm. She then told the medical records person don't bother pulling the chart because I told her she wouldn't get a call back. The med records person was uncomfortable with this, pulled the chart and gave it to a physician who was still in the practice. This was a near‐miss because the medical records person did give the message to the doctor who called the patient back.”
Finally, we found that in four cases (7%), amelioration resulted in system changes. These changes were: (1) clarifying and fixing procedures for reviewing diagnostic test results, (2) improving intake procedures for patients on warfarin, (3) consolidation of vaccination information in medical charts, and (4) placement of signs for clinicians to confirm correct vials are taken when drawing up similar‐looking vaccinations.
“Although there is a form used for vaccinations in this office, there was no systematic way of dealing with previous records. There is now a new protocol in place because this event, although rare, occurred several times in the past few weeks. The MA came up with the new plan.”
“A general problem, not event‐specific: tetanus immunization and TB multi‐dose vials look very much the same. We really need to be careful. Except for a small dot on one of them, they are very similar and are usually stored near/next to each other. Reporter plans to put big note by fridge where bottles kept.”
Discussion
Extensive patient safety literature has been devoted to describing how medical care goes wrong; however, less attention has been given to what goes right. Amelioration likely occurs routinely as clinicians and staff correct errors as a matter of course, but little is known about the characteristics of how people take action to interrupt the cascade before it affects the patient. This study is the first to systematically investigate such events in primary care.
Our evidence points to one possible framework for developing a culture of patient safety. System fixes can be effective in stopping cascades by catching mistakes and directing action; this represents the ideal situation. Chance plays a role in uncovering other problems. Even in cases in which errors are detected, there must be enough time to correct errors before they affect patients, and potential ameliorators must have the resolve to follow through with corrective action. Detecting errors is necessary, but not sufficient (fig 2). Importantly, we found that patients can also be effective ameliorators.
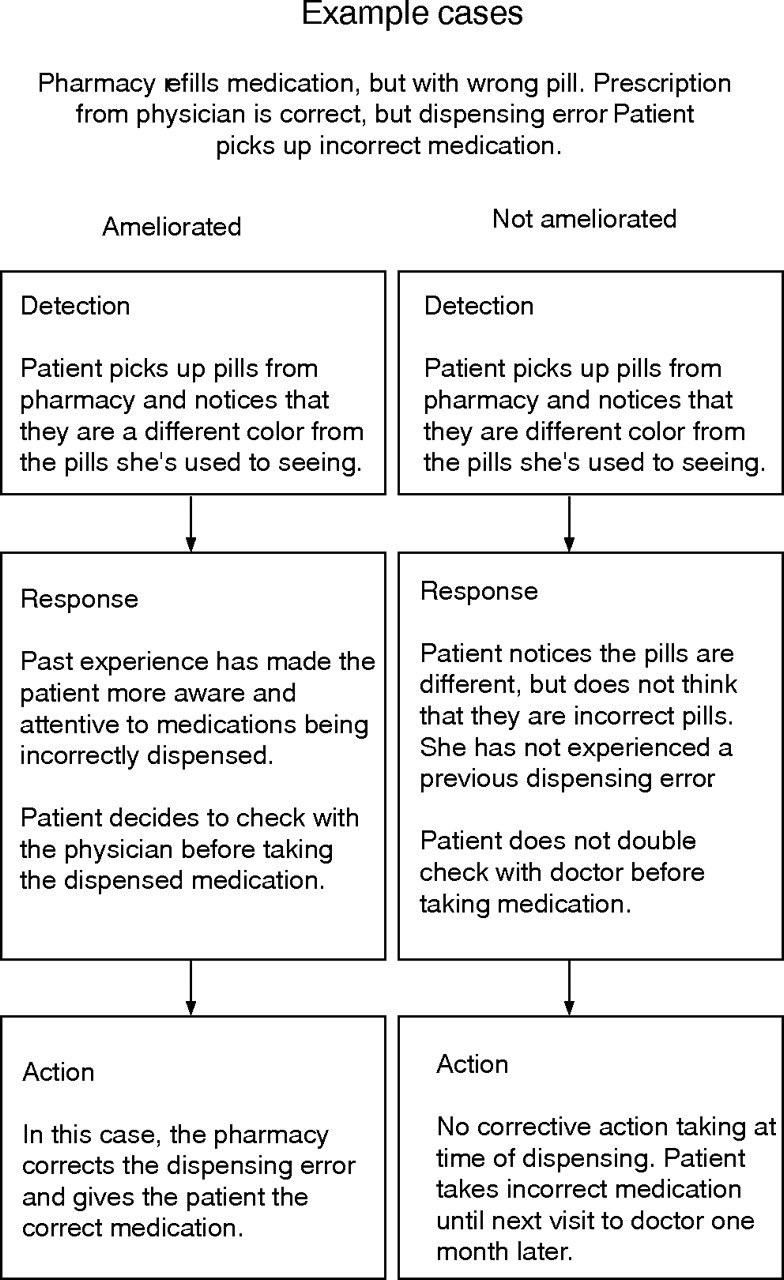
Figure 2 Comparative case examples.
We found that attentiveness, vigilance, and perseverance were present in many cases, and often represented the only mechanism that arrests a cascade. Some people appear to have these characteristics such that, in the presence of an error, there is a persistent sense that something is not right and it must be pursued until a satisfactory level of assurance is reached. As noted by Leonard et al,21 these characteristics may also be taught by cultivating a culture of safety: one that inculcates attentiveness, safe questioning, and resolution among clinicians, staff and patients. This culture of safety has the potential to increase the likelihood of (1) chance discovery of events through attentiveness, and (2) corrective action even in the absence of protocols. Of equal importance, we found that even errors detected by chance can lead to system changes in a environment that promotes patient safety.
Descriptions of error recovery in a hospital pharmacy and emergency department suggest the importance of detection through attentiveness (for example, double‐checking, knowledge, experience, anticipation) and correction through vigilance (patient advocacy, clarification, reasoning).13,14 Staff and clinicians may benefit from regular review of real de‐identified events.9,12,13 Noting exceptional examples of how co‐workers take corrective action might encourage others to take action. In addition, all staff should be encouraged to double‐check or second‐guess when things do not seem right or are different from the routine. This calls for wider training of all office personnel to be more attentive to what they are doing, and the potential consequences of both their action and inaction—similar to what has been advocated for clinicians.22 Providing incentives for such initiative may further enhance the safety culture.10
Because of the limitations inherent in a voluntary reporting system, there may be common types of ameliorated cases that were not reported and thus not described in this report, and the true distribution of ameliorator types is unknown. In addition, the true incidence of ameliorated events is unknown, and it is likely that they are much more common but underreported.
The focus of most patient safety studies has been on preventing errors. While an admirable goal, it is also clear that it will be impossible to prevent all errors in our current healthcare system. Identifying the characteristics of our healthcare system, its personnel and its patients that lead to termination of the error cascade may play an important role in improving patient outcomes. Our findings are consistent with others in terms of detection and correction, but this first look at ameliorated events in ambulatory settings highlights that people—in the absence of protocolised error recovery systems—make a difference. This further reinforces the need for a medical culture that empowers all stakeholders—clinicians, staff, administrators and patients—to ask questions and act on the cues of an error.
Abbreviations
ASIPS - Applied Strategies for Improving Patient Safety
Footnotes
Funding: Funding for this study was provided by the Agency for Healthcare Research and Quality, grant # 1U18HS011878‐01, Wilson D Pace, principal investigator.
Competing interests: None declared.
Portions of this were presented at the North American Primary Care Research Group Annual Meeting, October 2004, Orlando, Florida.
References
- 1.Fernald D H, Pace W D, Harris D M.et al Event reporting to a primary care patient safety reporting system: a report from the ASIPS Collaborative. Ann Fam Med 20042327–332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Woolf S H, Kuzel A J, Dovey S M.et al A string of mistakes: the importance of cascade analysis in describing, counting, and preventing medical errors. Ann Fam Med 20042317–326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Elder N C, Dovey S M. Classification of medical errors and preventable adverse events in primary care: a synthesis of the literature. J Fam Pract 200251927–932. [PubMed] [Google Scholar]
- 4.Kuzel A J, Woolf S H, Gilchrist V J.et al Patient reports of preventable problems and harms in primary health care. Ann Fam Med 20042333–340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dovey S M, Meyers D S, Phillips R L., Jret al A preliminary taxonomy of medical errors in family practice. Qual Saf Health Care 200211233–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gandhi T K, Weingart S N, Borus J.et al Adverse drug events in ambulatory care. N Engl J Med 20033481556–1564. [DOI] [PubMed] [Google Scholar]
- 7.Hickner J M, Fernald D H, Harris D M.et al Issues and initiatives in the testing process in primary care physician offices. Jt Comm J Qual Patient Saf 20053181–89. [DOI] [PubMed] [Google Scholar]
- 8.Toxic cascades: a comprehensive way to think about medical errors Am Fam Physician. 2001;63:847. [PubMed] [Google Scholar]
- 9.National Center for Patient Safety Department of Veterans Affairs. Culture change: prevention, not punishment. 2006. Available at http://www.patientsafety.gov/vision.html (accessed September 2006)
- 10.Weeks W B, Bagian J P. Developing a culture of safety in the Veterans Health Administration. Eff Clin Pract 20003270–276. [PubMed] [Google Scholar]
- 11.Helmreich R L. On error management: lessons from aviation. BMJ 2000320781–785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Carroll J S, Rudolph J W, Hatakenaka S. Lessons learned from non‐medical industries: root cause analysis as culture change at a chemical plant. Qual Saf Health Care 200211266–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kanse L, van der Schaaf T W, Vrijland N D.et al Error recovery in a hospital pharmacy. Ergonomics 200649503–516. [DOI] [PubMed] [Google Scholar]
- 14.Henneman E A, Blank F S, Gawlinski A.et al Strategies used by nurses to recover medical errors in an academic emergency department setting. Appl Nurs Res 20061970–77. [DOI] [PubMed] [Google Scholar]
- 15.Westfall J M, Fernald D H, Staton E W.et al Applied Strategies for Improving Patient Safety: a comprehensive process to improve care in rural and frontier communities. J Rural Health 200420355–362. [DOI] [PubMed] [Google Scholar]
- 16.Pace W D, Staton E W, Higgins G S.et al Database design to ensure anonymous study of medical errors: a report from the ASIPS Collaborative. J Am Med Inform Assoc 200310531–540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pace W D, Fernald D H, Harris D.et al Developing a taxonomy for coding ambulatory medical errors: a report from the ASIPS Collaborative. In: Advances in patient safety: from research to implementation. Volume 2. Concepts and methodology. AHRQ Publication No 05–0021–2. Rockville, MD: Agency for Healthcare Research and Quality, 2005 [PubMed]
- 18.West D, Westfall J M, Araya‐Guerra R.et al Using reported primary care errors to develop and implement patient safety interventions: a report from the ASIPS Collaborative. In: Advances in patient safety: from research to implementation. Volume 3. Implementation issues AHRQ Publication No 05‐0021‐3. Rockville, MD: Agency for Healthcare Research and Quality, 2005 [PubMed]
- 19.The ASIPS Collaborative Dimensions of medical outcome. The ASIPS‐Victoroff taxonomy. 2005. Available at http://www.errorsinmedicine.net/taxonomy/ (accessed December 2006)
- 20.Crabtree B F, Miller W L. Using Codes and Code Manuals. In: Crabtree BF, Miller WL (eds). Doing qualitative research. Thousand Oaks, CA: Sage Publications, 1999163–177.
- 21.Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care 200413(Suppl 1)i85–i90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Borrell‐Carrio F, Epstein R M. Preventing errors in clinical practice: a call for self‐awareness. Ann Fam Med 20042310–316. [DOI] [PMC free article] [PubMed] [Google Scholar]