

Abstract
Context:
The effects of prophylactic ankle braces on lower extremity functional performance in healthy participants have not been studied extensively.
Objective:
To determine if prophylactic ankle braces affected multidirectional reach distances during a test of dynamic balance.
Design:
Crossover.
Setting:
Laboratory.
Patients or Other Participants:
Thirty-six healthy, physically active volunteers (18 men, 18 women; age = 23.6 ± 2.7 years, height = 173.8 ± 9.3 cm, mass = 74.4 ± 12.7 kg, reach-leg length = 91.9 ± 5.1 cm).
Intervention(s):
Volunteers performed balance testing in 3 conditions: unbraced, while wearing a semirigid ankle brace, and while wearing a lace-up ankle brace.
Main Outcome Measure(s):
We used the Star Excursion Balance Test, calculating the mean of 3 attempts in 8 directions (anterior, anterior-medial, medial, posterior-medial, posterior, posterior-lateral, lateral, and anterior-lateral), normalized by the participant's reach-leg length. Data were collected after 6 practice attempts for each of the conditions according to a balanced Latin square.
Results:
Bracing condition had no effect (P > .05) on any of the Star Excursion Balance Test directional measures. The largest mean difference due to bracing was 2.5% between the lace-up brace condition and the control in the posterior reach direction. This indicates that the actual reach differences due to bracing were less than 5.08 cm (2 inches) in length.
Conclusions:
Clinicians can be confident that the prophylactic use of ankle braces does not disrupt lower extremity dynamic balance during a reaching task in healthy participants.
Keywords: single-limb stance, dynamic balance, postural stability
Key Points.
Compared with no brace, semirigid and lace-up ankle braces had no effect on any Star Excursion Balance Test measures in healthy volunteers.
Clinicians can feel confident that the prophylactic use of ankle braces in healthy participants does not disrupt lower extremity dynamic balance during a reaching task.
The ankle is often injured during sporting events.1 As a result, many athletes and sports medicine personnel recommend the use of prophylactic ankle braces to reduce the rate of injury, regardless of a previous history of ankle injury.2,3 In addition to the prophylactic effects of ankle braces, researchers have shown proprioceptive4–6 and mechanical5,6 benefits. Prophylactic ankle braces, classified as either lace-up or semirigid, limit ankle motions associated with lateral ankle sprains (plantar flexion and inversion).7 However, each classification of bracing limits the motions differently and to various degrees.7 Semirigid braces restrict more inversion range of motion (ROM), whereas lace-up style ankle braces more effectively decrease plantar-flexion and dorsiflexion ROM.7 Thus, functional performance may be affected differently depending on the style of brace worn, even in a healthy person.
The results of past research have not been consistent regarding the effects of ankle bracing on performance.8–14 This lack of consensus may be due to the variety of methods and measures used to assess brace efficacy. Authors investigating whole-body performance tasks, such as vertical jump height,9,10 sprint speed,9,10 agility drills,9,10 and 1-legged static balance tests,11,12 reported no effect of bracing on such measures. However, other authors indicated that bracing did affect 1-legged static balance13 and 2-legged drop landing measures.14 When an individual uses an ankle brace during functional tasks, the body may compensate mechanically by relying more on gross movements elsewhere in the kinetic chain, such as at the hip and knee, than on isolated movements of the ankle. Other investigators may have attempted to identify bracing effects on static single-limb variables in order to limit mechanical compensation.8,11,12 By using static, single-limb tasks to measure the effects of bracing, it is understandable that postural control variables would be improved,8 not affected,11,12 or negatively affected13 by ankle bracing. However, information regarding the effects of ankle bracing during single-limb, closed-chain, multiplanar tasks remains limited.
Single-limb dynamic balance can be assessed in multiple directions using the Star Excursion Balance Test (SEBT).15,16 Participants assume a single-leg stance and reach as far as possible in 8 directions, thereby challenging their dynamic balance.17 Previous researchers and ankle brace manufacturers identified restricted ROMs while participants wore ankle braces.7,18 However, this factor has not been assessed under dynamic balance conditions, such as those induced by the SEBT. In the SEBT, contralateral-limb reach distances may be affected, especially in directions purportedly limited by the style of the prophylactic ankle brace. For example, if plantar flexion and dorsiflexion are limited by a lace-up style brace, reach in the anterior and posterior SEBT directions may be limited. Similarly, if inversion and eversion are restricted by a semirigid brace, we expect to see decreased performance in the medial and lateral SEBT directions. Therefore, our study had 2 purposes: (1) to determine if bracing had an overall effect on SEBT reach distance, and (2) to compare the effects of 2 ankle braces on SEBT reach distance in healthy participants.
Methods
Design
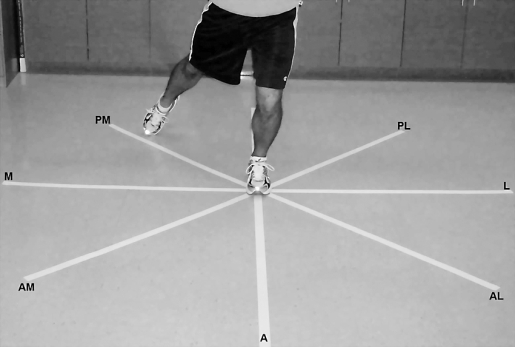
We used a crossover design with brace condition (unbraced [UB], semirigid [SR], or lace-up [LU]) as the independent variable. The dependent variables were the mean SEBT reach distance of 3 attempts in each of the 8 directions (anterior [A], anterior-medial [AM], medial [M], posterior-medial [PM], posterior [P], posterior-lateral [PL], lateral [L], and anterior-lateral [AL]; Figure). Normalization procedures were based on those of Gribble and Hertel,17 who used the leg length (%LL) of the reach leg (nondominant leg performing the reach in each direction). All testing was performed in the laboratory setting.
Figure. Star Excursion Balance Test grid for left-leg dominant participants. (Posterior direction not shown.) Abbreviations: A, anterior; AM, anterior-medial; M, medial; PM, posterior-medial; P, posterior; PL, posterior-lateral; L, lateral; AL, anterior-lateral.
Participants
Thirty-six physically active, healthy male and female college-aged volunteers (18 men, 18 women; age = 23.6 ± 2.7 years, height = 173.8 ± 9.3 cm, mass = 74.4 ± 12.7 kg, reach-leg length = 91.9 ± 5.1 cm, right-leg dominant = 28, left-leg dominant = 8) consented to participate. Individuals were excluded if they reported any (1) somatosensory condition that could impair balance, (2) previous head injury resulting in a loss of consciousness, (3) lower extremity injury or feelings of “giving way” that resulted in any time loss of physical activity from practice or competition within the past year, (4) feelings of either ankle giving way at the time of the study and unrelated to previous injury, (5) flu-like or cold-like symptoms within the past 6 weeks, which could impair balance, or (6) pregnancy. Lastly, volunteers were excluded if they were unable to perform the SEBT during the practice session. This study was approved by the university's institutional review board.
Instruments
The SEBT is a multidirectional test designed to measure dynamic balance. The SEBT grid, as shown in the Figure, was constructed using 16 interlocking mats (61.0 cm × 61.0 cm × 1.27 cm) to form a 243.8 × 243.8-cm2 mat. Four 243.8 × 3.8-cm2 white lines were painted on the mats, with each centimeter marked and every 5 cm labeled. The directions were labeled in reference to the reach direction in relation to the stance limb and consisted of A, AM, M, PM, P, PL, L, and AL. Each direction was at a 45° angle to the next direction. The SEBT testing procedures used were the same as those previously reported.15–17,19–23 Reliability for the SEBT has been determined, with intraclass correlation coefficients ranging from .67 to .87.15 Intratester values were established during pilot testing and post hoc analyses for each direction in attempts 1 and 2 in each brace condition for all 36 participants. All analyses were based on procedures described by Portney and Watkins.24 The intratester values (intraclass correlation coefficients 3,1) calculated for each direction were as follows: A = .96, AM = .95, M = .97, PM = .97, P = .98, PL = .97, L = .96, and AL = .94.
Procedures
Each volunteer reported to the laboratory dressed in shorts, a T-shirt, and his or her own low-cut athletic shoes for 1 session lasting approximately 45 minutes. The session included screening, familiarization, and data collection.
Screening consisted of providing informed consent, completing a health-history questionnaire, determining the dominant leg, and measuring the nondominant-leg length. Once inclusion criteria were met, the participant's dominant or stance leg was determined according to which limb was used in at least 2 of the 3 following tests: recovering balance after a posterior push, stepping up on a box, and kicking a ball through a goal.25 The first test to determine leg dominance involved perturbing the volunteer in the anterior direction, applied midway between the scapulae, with enough force to displace the center of gravity and require the participant to step forward to recover balance. The leg used to recover balance was deemed dominant. The second test used a 20-cm step; the leg that performed the step up was considered the dominant leg. The third test involved kicking a ball through a 1-m goal using a single kick while standing 10 m from the goal. The leg used to kick the ball was determined to be dominant.
Because the nondominant leg was used as the reach limb during data collection, its limb length was measured from the anterior superior iliac spine to the center of the medial malleolus of the ipsilateral leg. This measure (cm) was taken while the participant lay supine on a treatment table. The leg length was used to normalize the reach distances, so that treatment effects could be compared among volunteers.17
Participants completed SEBT practice sessions before data collection. One attempt included 1 reach in each of the 8 test directions. Six attempts were performed under each brace condition, for a total of 18 practice attempts, to reduce learning effects, as suggested by Hertel et al.19 Data collection consisted of SEBT attempts for each brace condition, for a total of 9 attempts. The order of braced conditions was randomized according to a balanced Latin square. Data collection occurred immediately after the practice session in each brace condition to limit loss of any learning effect gained from the practice attempts.
The lace-up brace (Ankle Stabilizer Orthosis; Medical Specialties, Inc, Charlotte, NC) and semirigid brace (T2 Active Ankle; Active Ankle Systems, Jeffersonville, IN) were sized and fitted according to manufacturer's specifications before that condition's practice session. The same certified athletic trainer applied all braces for practice and test attempts. The participants wore socks supplied by the investigators for all practice and data collection SEBT attempts. Volunteers wore their own athletic shoes; the condition and amount of wear varied.
The participant began by standing on the dominant leg at the center of the SEBT grid (Figure). The plantar aspect of the first metatarsophalangeal joint (“ball of the foot”) was positioned on the intersecting lines at the center of the grid to maintain consistency in foot placement among brace conditions. Using the reach leg and starting on the ground from the center of the grid, the volunteer was instructed to reach the maximal distance possible and touch the line using the most distal part of the reach foot, without supporting the body weight with the reach leg, while maintaining the dominant leg in the center of the grid. The reach leg was then immediately returned to the start position. The next directional reach was performed, without rest, until all 8 directions were completed for each attempt. The order of the directional reaches was as follows: A, AM, M, PM, P, PL, L, AL.16,17,19 Individuals were encouraged to reach as far as possible but were not provided feedback on their strategy or movement pattern to complete the task. After a successful attempt, the participant rested for approximately 15 seconds before the next attempt19 or up to 5 minutes17 between bracing conditions. During the time between bracing conditions, the volunteer was fitted for the subsequent condition. Each individual completed 27 attempts, including 6 practice attempts and 3 data collection attempts for each of the 3 bracing conditions.
A mistrial was operationally defined if any of the following occurred: (1) the participant placed more body weight than a light touch on the reach leg to stop the body from falling in that direction, (2) the reach leg came to rest on the mat, (3) the stance leg's ball of the foot moved from the center of the grid, or (4) the reach leg could not be returned to the center of the grid under control as subjectively determined by the primary investigator.17 Data from mistrials were discarded and recollected. Maximums of 6 mistrials during practice sessions and 2 mistrials during data collection were allowed. However, all participants tested were able to perform the SEBT, and no one was excluded from the study due to mistrials.
The primary investigator (L.H.) marked a dot on the SEBT line to correspond with the touch of the reach foot in each of the test directions. Reach distances were measured at the completion of testing for each brace condition while the volunteer was resting. Reach distances were measured to the nearest 0.5 cm with a tape measure and recorded from the center of the grid to the investigator's dot mark for each of the 8 directions. The dot marks were removed from the SEBT mat after each brace condition, so the individual was blinded to his or her previous performance.
Statistical Analysis
The mean of the 3 attempts in each direction was calculated for each brace condition and normalized to %LL. The computed %LL in each direction was used in the analysis.
We computed 8 separate 1-way (brace) analyses of variance with repeated measures to assess the effect of brace condition on SEBT direction (A, AM, M, PM, P, PL, L, AL) scores using Number Cruncher Statistical Software (version 2004; NCSS, Kaysville, UT). The α level was set a priori at .05.
Results
Bracing condition had no effect on any of the SEBT directional measures (P > .05; Table 1). To reduce the chance of a type II error, we calculated 95% confidence intervals using the Tukey-Kramer multiplier to compare data with a 5%LL practical difference, which represents a 4.6-cm (∼2-in) reach distance difference (Table 2). None of the confidence intervals exceeded the 5% practical difference.
Table 1.
Normalized Reach Scores (%LL) for Condition and Direction (Mean ± SD)a

Table 2.
Tukey-Kramer Simultaneous Confidence Intervals for the Multiple Comparisons of the Braced and Unbraced Conditions (%LL)a

Discussion
We investigated the effect of 2 common styles of ankle braces on the ability to reach with the opposite limb in 8 directions and found that neither brace diminished dynamic balance compared with the control condition. Although previous researchers7 found that prophylactic ankle braces restricted motion, these restrictions did not affect dynamic balance in our study. Our results are in agreement those of previous authors,9,10,12,14,26 who demonstrated that ankle bracing did not reduce functional performance.
We expected a difference among bracing conditions in the SEBT directions due to previous findings5,7,18,27,28 of restricted ROM with semirigid and lace-up ankle braces. The semirigid brace restricted more frontal-plane ROM than did the lace-up brace, whereas the lace-up brace restricted more sagittal-plane ROM.7,18 We expected differences among bracing conditions, because if ROM was restricted with ankle brace use, then opposite-limb reach distances also would decrease due to the motion needed in the braced stance leg. Earlier studies of ROM with ankle braces involved single-plane measures; ours incorporated measures in multiple planes of movement. The multidirectional nature of the SEBT and lack of significant findings in our study may suggest that performance on a dynamic balance task is maintained in healthy individuals, regardless of whether a brace is worn. Whether ankle ROM is limited by the brace, causing other segments in the kinetic chain to compensate and achieve necessary motion, is unknown.
Several groups9,10,14,26 have examined brace effectiveness during functional testing. However, to our knowledge, no one has examined the effect of prophylactic bracing on healthy individuals during dynamic balancing tasks. We believe it is important to examine dynamic balance to gain insight into how ankle braces affect motion in specific directions. Restricted motion in a single direction may affect one's performance or risk of injury and, therefore, whether a brace should be used for prophylactic purposes in a healthy athlete must be carefully considered. Our results showed that reach distance was not affected by either the semirigid or lace-up ankle brace in healthy individuals. These findings support the continued use of prophylactic ankle braces and provide evidence that dynamic balance can be sustained, even while wearing ankle braces that are claimed to limit ROM.
The trends of our data for reach directions were similar to those of Gribble and Hertel17: SEBT reach distances were greater in the posterior and medial directions and less in the anterior and lateral directions. These findings may be due to the ease of moving the reach leg in the posterior and medial directions and the greater difficulty moving in the anterior and lateral directions, while maintaining a stable base of support on the dominant leg.
Limitations of our study should be considered. The dynamic balance we tested is not the same as that involved in more dynamic sporting activities, such as running or jumping. Additionally, we did not attempt to study the injury reduction rate of the brace. Thus, other factors such as level of protection, cost, fit, and comfort should be of more importance when selecting a prophylactic brace. It is also possible that fatigue may have affected performance on the SEBT attempts. Subjective reports of feeling tired led us to further analyze our data to determine whether fatigue was a factor. Separate analyses between attempts 1 and 3 of each bracing condition revealed no differences, suggesting that subjective fatigue was not a factor on performance.
In trying to differentiate between statistical and practical significance, we chose a practical change of 5%LL, which is approximately a 2-in (5.08-cm) reach difference. As in most sporting events, a 2-in (5.08-cm) difference in reach can mean a great deal. Because the largest difference was 2.5%LL, we can conclude assuredly that the bracing did not influence the reach distance and, therefore, will not influence a healthy athlete's performance.
Conclusions
Clinicians can be confident that the prophylactic use of semirigid and lace-up style ankle braces does not disrupt the ability to maintain dynamic balance in healthy individuals. Athletic trainers and athletes should consider the role of prophylactic ankle braces in preventing ankle sprains and be certain that the ankle braces will not alter a healthy individual's ability to balance under dynamic conditions.
Acknowledgments
This study was partially funded by the School of Graduate Studies at Indiana State University in Terre Haute, Indiana.
Footnotes
Lisa Hardy, MS, ATC, contributed to conception and design; acquisition and analysis and interpretation of the data; and drafting, critical revision, and final approval of the article. Kellie Huxel, PhD, LAT, ATC, contributed to conception and design and drafting, critical revision, and final approval of the article. Jody Brucker, PhD, LAT, ATC, contributed to conception and design, analysis and interpretation of the data, and drafting, critical revision, and final approval of the article. Thomas Nesser, PhD, CSCS, HFI, contributed to conception and design and drafting, critical revision, and final approval of the article.
References
- 1.Garrick J.G, Requa R.K. The epidemiology of foot and ankle injuries in sports. Clin Podiatr Med Surg. 1989;6(3):629–637. [PubMed] [Google Scholar]
- 2.Olmsted L.C, Vela L.I, Denegar C.R, Hertel J. Prophylactic ankle taping and bracing: a numbers-needed-to-treat and cost-benefit analysis. J Athl Train. 2004;39(1):95–100. [PMC free article] [PubMed] [Google Scholar]
- 3.Osborne M.D, Rizzo T.D., Jr Prevention and treatment of ankle sprain in athletes. Sports Med. 2003;33(15):1145–1150. doi: 10.2165/00007256-200333150-00005. [DOI] [PubMed] [Google Scholar]
- 4.Callaghan M.J. Role of ankle taping and bracing in the athlete. Br J Sports Med. 1997;31(2):102–108. doi: 10.1136/bjsm.31.2.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cordova M.L, Ingersoll C.D, Palmieri R.M. Efficacy of prophylactic ankle support: an experimental perspective. J Athl Train. 2002;37(4):446–457. [PMC free article] [PubMed] [Google Scholar]
- 6.Hume P.A, Gerrard D.F. Effectiveness of external ankle support: bracing and taping in rugby union. Sports Med. 1998;25(5):285–312. doi: 10.2165/00007256-199825050-00001. [DOI] [PubMed] [Google Scholar]
- 7.Cordova M.L, Ingersoll C.D, LeBlanc M.J. Influence of ankle support on joint range of motion before and after exercise: a meta-analysis. J Orthop Sports Phys Ther. 2000;30(4):170–182. doi: 10.2519/jospt.2000.30.4.170. [DOI] [PubMed] [Google Scholar]
- 8.Jerosch J, Thorwesten L, Bork H, Bischof M. Is prophylactic bracing of the ankle cost effective. Orthopedics. 1996;19(5):405–414. doi: 10.3928/0147-7447-19960501-10. [DOI] [PubMed] [Google Scholar]
- 9.Gross M.T, Everts J.R, Roberson S.E, Roskin D.S, Young K.D. Effect of Donjoy Ankle Ligament Protector and Aircast Sport-Stirrup orthoses on functional performance. J Orthop Sports Phys Ther. 1994;19(3):150–156. doi: 10.2519/jospt.1994.19.3.150. [DOI] [PubMed] [Google Scholar]
- 10.Rosenbaum D, Kamps N, Bosch K, Thorwesten L, Volker K, Eils E. The influence of external ankle braces on subjective and objective parameters of performance in a sports-related agility course. Knee Surg Sports Traumatol Arthrosc. 2005;13(5):419–425. doi: 10.1007/s00167-004-0584-7. [DOI] [PubMed] [Google Scholar]
- 11.Kinzey S.J, Ingersoll C.D, Knight K.L. The effects of selected ankle appliances on postural control. J Athl Train. 1997;32(4):300–303. [PMC free article] [PubMed] [Google Scholar]
- 12.Barkoukis V, Sykaras E, Costa F, Tsorbatzoudis H. Effectiveness of taping and bracing in balance. Percept Mot Skills. 2002;94(2):566–574. doi: 10.2466/pms.2002.94.2.566. [DOI] [PubMed] [Google Scholar]
- 13.Bennell K.L, Goldie P.A. The differential effects of external ankle support on postural control. J Orthop Sports Phys Ther. 1994;20(6):287–295. doi: 10.2519/jospt.1994.20.6.287. [DOI] [PubMed] [Google Scholar]
- 14.McCaw S.T, Cerullo J.F. Prophylactic ankle stabilizers affect ankle joint kinematics during drop landings. Med Sci Sports Exerc. 1999;31(5):702–707. doi: 10.1097/00005768-199905000-00013. [DOI] [PubMed] [Google Scholar]
- 15.Kinzey S.J, Armstrong C.W. The reliability of the star-excursion test in assessing dynamic balance. J Orthop Sports Phys Ther. 1998;27(5):356–360. doi: 10.2519/jospt.1998.27.5.356. [DOI] [PubMed] [Google Scholar]
- 16.Nakagawa L, Hoffman M. Performance in static, dynamic, and clinical tests of postural control in individuals with recurrent ankle sprains. J Sport Rehabil. 2004;13:255–268. [Google Scholar]
- 17.Gribble P.A, Hertel J. Considerations for normalizing measures of the Star Excursion Balance Test. Measure Phys Educ Exerc Sci. 2003;7:89–100. [Google Scholar]
- 18.Eils E, Demming C, Kollmeier G, Thorwesten L, Volker K, Rosenbaum D. Comprehensive testing of 10 different ankle braces: evaluation of passive and rapidly induced stability in subjects with chronic ankle instability. Clin Biomech (Bristol, Avon) 2002;17(7):526–535. doi: 10.1016/s0268-0033(02)00066-9. [DOI] [PubMed] [Google Scholar]
- 19.Hertel J, Miller S.J, Denegar C.R. Intratester and intertester reliability during the Star Excursion Balance Tests. J Sport Rehabil. 2000;9(2):104–116. [Google Scholar]
- 20.Olmsted L.C, Carcia C.R, Hertel J, Shultz S.J. Efficacy of the Star Excursion Balance Tests in detecting reach deficits in subjects with chronic ankle instability. J Athl Train. 2002;37(4):501–506. [PMC free article] [PubMed] [Google Scholar]
- 21.Gribble P.A, Hertel J, Denegar C.R, Buckley W.E. The effects of fatigue and chronic ankle instability on dynamic postural control. J Athl Train. 2004;39(4):321–329. [PMC free article] [PubMed] [Google Scholar]
- 22.Earl J.E, Hertel J. Lower-extremity muscle activation during the Star Excursion Balance Tests. J Sport Rehabil. 2001;10(2):93–104. [Google Scholar]
- 23.Gray G.W. Lower Extremity Functional Profile. Adrian, MI: Wynn Marketing Inc; 1995. [Google Scholar]
- 24.Portney L, Watkins M. Foundations of Clinical Research: Applications to Practice. 2nd ed. Upper Saddle River, NJ: Prentice Hall, Inc; 2000. [Google Scholar]
- 25.Hoffman M, Schrader J, Applegate T, Koceja D. Unilateral control of the functionally dominant and nondominant extremities of healthy subjects. J Athl Train. 1998;33(4):319–322. [PMC free article] [PubMed] [Google Scholar]
- 26.Gudibanda A, Wang Y. Effect of the Ankle Stabilizing Orthosis on foot and ankle kinematics during cutting maneuvers. Res Sports Med. 2005;13(2):111–126. doi: 10.1080/15438620590956115. [DOI] [PubMed] [Google Scholar]
- 27.Johnson R.E, Veale J.R, McCarthy G.J. Comparative study of ankle support devices. J Am Podiatr Med Assoc. 1994;84(3):107–114. doi: 10.7547/87507315-84-3-107. [DOI] [PubMed] [Google Scholar]
- 28.Jerosch J, Hoffstetter I, Bork H, Bischof M. The influence of orthoses on the proprioception of the ankle joint. Knee Surg Sports Traumatol Arthrosc. 1995;3(1):39–46. doi: 10.1007/BF01553524. [DOI] [PubMed] [Google Scholar]