

Abstract
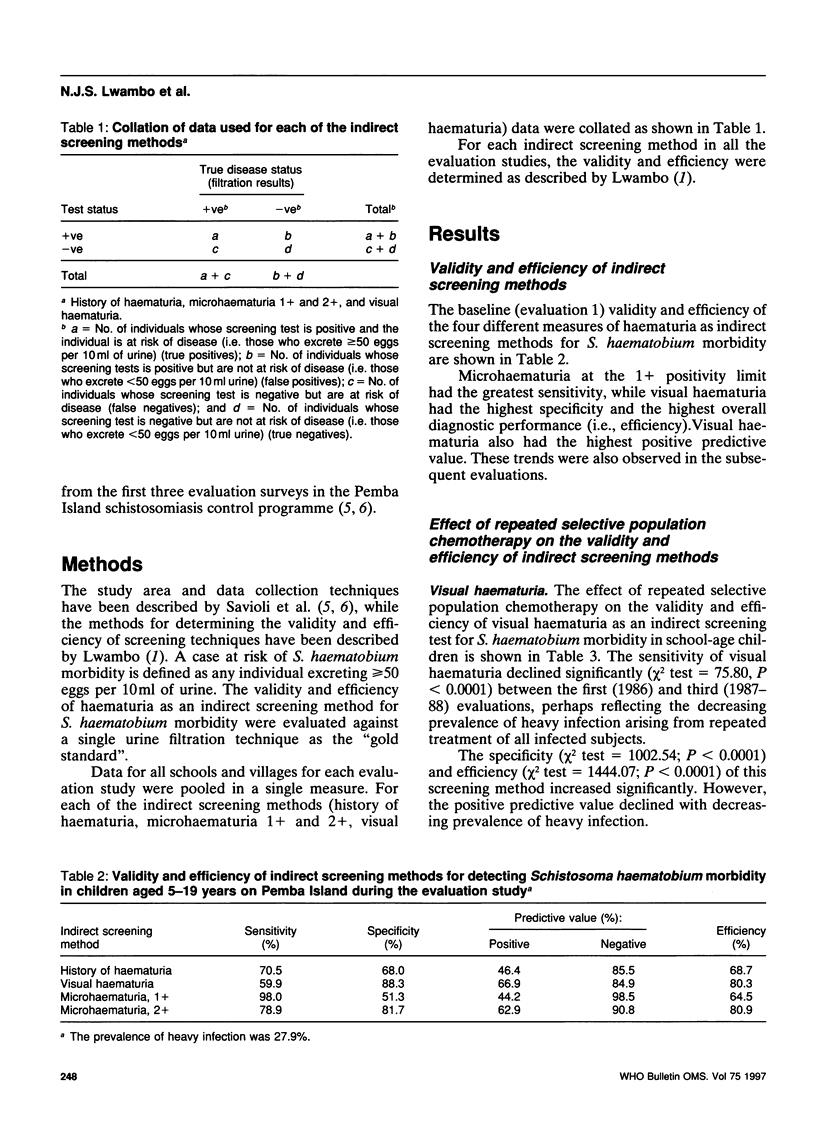
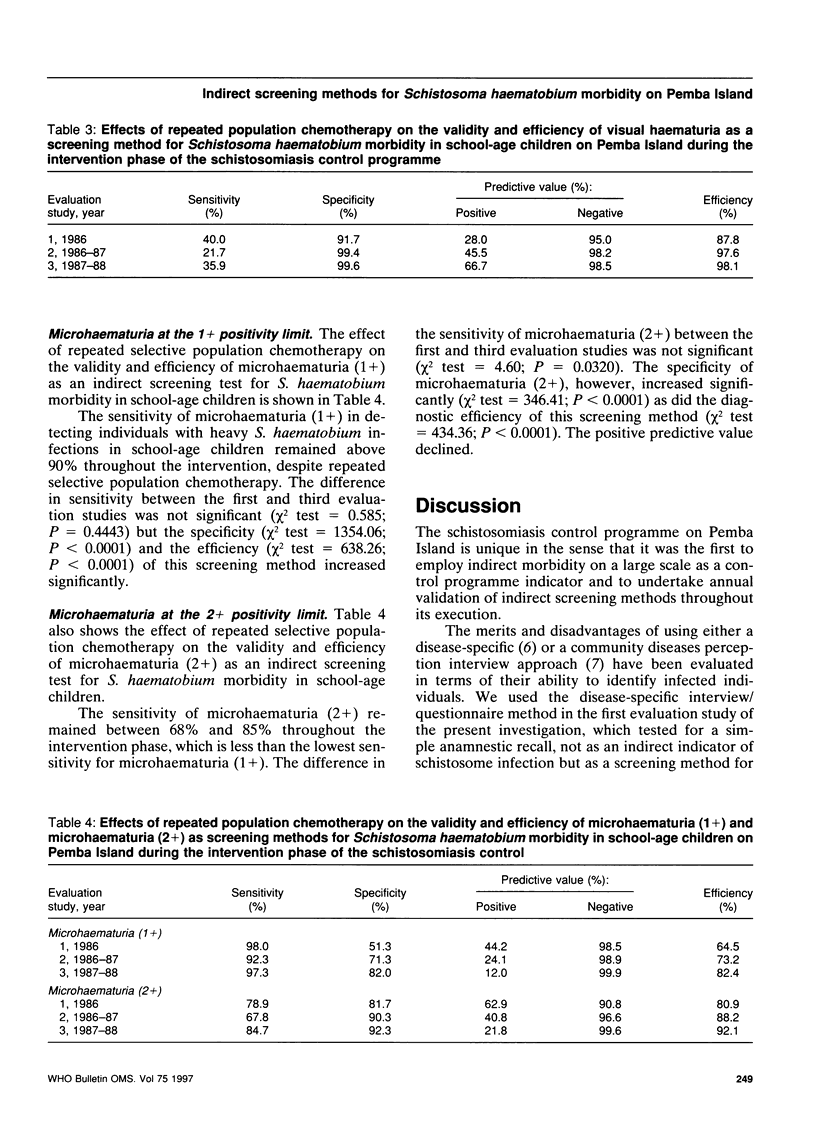
Four indirect screening methods for the detection of Schistosoma haematobium morbidity are compared (history of haematuria, visual haematuria, and microhaematuria at the 1+ and 2+ positivity limit by reagent strips) in terms of their diagnostic performance under conditions of progressive decrease in prevalence of infection, intensity and risk of morbidity as a result of repeated schistosomiasis control programmes on Pemba Island, United Republic of Tanzania. The results show that the sensitivity of a history of haematuria was higher (71%) in children but lower in adults (40%), similar to the findings for visual haematuria in children (60%) and adults (40%) at baseline. However, visual haematuria had a higher specificity, positive predictive value, and efficiency than a history of haematuria in both children and adults. Microhaematuria at the 1+ positivity limit (by reagent strips) had the highest sensitivity of all the methods investigated, but the lowest specificity, positive predictive value, and efficiency. Quantitatively, the indirect methods tended to increase in specificity, negative predictive value, and efficiency during the course of the intervention programme. In contrast, positive predictive value tended to decrease, while the sensitivity remained fairly stable. Overall, these findings suggest that a history of haematuria and/or visual haematuria are appropriate methods for preliminary screening of communities to identify those at risk of morbidity. Thereafter, microhaematuria (1+ positivity limit) may be the more appropriate method for targeting intervention at the individual level.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Hatz C., Savioli L., Mayombana C., Dhunputh J., Kisumku U. M., Tanner M. Measurement of schistosomiasis-related morbidity at community level in areas of different endemicity. Bull World Health Organ. 1990;68(6):777–787. [PMC free article] [PubMed] [Google Scholar]
- King C. H., Lombardi G., Lombardi C., Greenblatt R., Hodder S., Kinyanjui H., Ouma J., Odiambo O., Bryan P. J., Muruka J. Chemotherapy-based control of schistosomiasis haematobia. I. Metrifonate versus praziquantel in control of intensity and prevalence of infection. Am J Trop Med Hyg. 1988 Sep;39(3):295–305. doi: 10.4269/ajtmh.1988.39.295. [DOI] [PubMed] [Google Scholar]
- Lengeler C., Komba S., Morona D. Urinary schistosomiasis: influence of the circadian variation of hematuria and proteinuria on reagent stick testing. Acta Trop. 1991 Feb;48(4):313–317. doi: 10.1016/0001-706x(91)90019-g. [DOI] [PubMed] [Google Scholar]
- Lengeler C., de Savigny D., Mshinda H., Mayombana C., Tayari S., Hatz C., Degrémont A., Tanner M. Community-based questionnaires and health statistics as tools for the cost-efficient identification of communities at risk of urinary schistosomiasis. Int J Epidemiol. 1991 Sep;20(3):796–807. doi: 10.1093/ije/20.3.796. [DOI] [PubMed] [Google Scholar]
- Savioli L., Dixon H., Kisumku U. M., Mott K. E. Control of morbidity due to Schistosoma haematobium on Pemba Island: programme organization and management. Trop Med Parasitol. 1989 Jun;40(2):189–194. [PubMed] [Google Scholar]
- Savioli L., Dixon H., Kisumku U. M., Mott K. E. Control of morbidity due to Schistosoma haematobium on Pemba island; selective population chemotherapy of schoolchildren with haematuria to identify high-risk localities. Trans R Soc Trop Med Hyg. 1989 Nov-Dec;83(6):805–810. doi: 10.1016/0035-9203(89)90336-2. [DOI] [PubMed] [Google Scholar]
- Savioli L., Hatz C., Dixon H., Kisumku U. M., Mott K. E. Control of morbidity due to Schistosoma haematobium on Pemba Island: egg excretion and hematuria as indicators of infection. Am J Trop Med Hyg. 1990 Sep;43(3):289–295. doi: 10.4269/ajtmh.1990.43.289. [DOI] [PubMed] [Google Scholar]
- Savioli L., Mott K. E. Urinary schistosomiasis on Pemba Island: low-cost diagnosis for control in a primary health care setting. Parasitol Today. 1989 Oct;5(10):333–337. doi: 10.1016/0169-4758(89)90129-4. [DOI] [PubMed] [Google Scholar]