

Abstract
Despite the fundamental nature of tonic immobility in anxiety responses, surprisingly little empirical research has focused on the “freeze” response in humans. The present report evaluated frequency and predictors of a freeze response in the context of a biological challenge. A nonclinical sample (N = 404) underwent a 20-sec inhalation of 20% CO2/balance O2. Perceptions of immobility in the context of the challenge were reported in 13% of the sample, compared to 20% reporting a significant desire to flee. Subjective anxiety and panic during the challenge were associated with the freeze response, as were a number of anxiety symptom dimensions.
Keywords: anxiety, freeze, panic, carbon-dioxide
1.1 Background
The phrase “fight or flight” was coined by Cannon (1927, 1929) in the 1920s to describe key behaviors that occur in the context of perceived threat. This term has not only been influential in later conceptual and empirical work on anxiety and its disorders, but the phrase also has become relatively well-known in popular culture. In the context of anxiety research, the alarm or fear response described by Barlow (2002) reflects an interaction between learning and innate, biological systems designed to help animals adapt to threat. The more contemporary notion of a true or false alarm still contains the two primary features of Cannon’s original expression, though the ordering of effects is probably best reversed; flight is the overwhelming action tendency subsequent to an alarm whereas relatively fewer instances of fight responses result from threat (Lang, 1994). Part of Barlow’s (2002) description of an adaptive alarm model suggests that a freeze response may occur in some threatening situations. Specifically, freezing -- or tonic immobility -- may overwhelm other competing action tendencies. For example, when fleeing or aggressive responses are likely to be ineffective, a freeze response may take place.
Similar to the flight/fight response, a freeze response is believed to have adaptive value. In the context of predatory attack, some animals will freeze or “play dead.” This response, often referred to as tonic immobility (Gallup, 1977), includes motor and vocal inhibition with an abrupt initiation and cessation. Ethologists have documented non-volitional freeze responses in several animal species (Arduino & Gould, 1984; Kalin, Shelton, Rickman, & Davidson, 1998). Freezing in the context of an attack seems counterintuitive. However, tonic immobility may be the best option when the animal perceives little immediate chance of escaping or winning a fight (Arduino & Gould, 1984; Korte, Koolhaas, Wingfield, & McEwen, 2005). For example, tonic immobility may be useful when additional attacks are provoked by movement or when immobility may increase the chance of escaping, such as when a predator believes its prey to be dead and releases it.
Despite evidence suggesting that tonic immobility may be a key facet of alarm reactions, freezing has received relatively little scientific attention in humans. One exception is the PTSD/rape literature wherein several studies have described a rape-induced paralysis that appears to share many of the features of tonic immobility (Galliano, Noble, Travis & Puechl, 1993; Mezey & Taylor, 1998; Scaer, 2001; Suarez & Gallup, 1977). This literature suggests that a relatively high percentage of rape victims feel paralyzed and unable to act despite no loss of consciousness during the assault (Burgess & Holmstrom, 1976; Heidt, Marx, & Forsyth, 2005). Since fear, predation, contact, and restraint are common to both rape and the induction of tonic immobility in animals, it has been concluded that these phenomena are essentially isomorphic (Suarez & Gallup, 1979).
Given the general paucity of research on human tendencies to freeze in the context of threat, as well as the general reliance on retrospective reports in the existed literature, we sought to expand knowledge in this area by providing a laboratory-based exploration of the tendency to freeze in the context of threat. Laboratory-based biological challenges offer controlled methods for understanding biological and psychological factors that influence the generation of fear (McNally, 1994; Schmidt et al., 2000; Zvolensky & Eifert, 2001). The primary aim of the present study was to determine whether laboratory-based threat stressors can provoke freeze responses and, if so, to evaluate the frequency and predictors of these responses. Because a CO2 challenge has been found to be a potent stressor (Zvolensky & Eifert, 2001), and a freeze tendency is believed to be a central response to threat, we hypothesized that some participants would report these reactions, although we believed these might be less frequent than flight responses. Although the challenge did not involve physical attack, participants are somewhat physically confined by a breathing apparatus attached around the head, which may simulate some of the parameters relevant to freeze in the context of predatory grasp. The second aim of the research was to determine whether anxiety-related traits or predisposing factors might predict a freeze response. There is little prior work to guide hypotheses but it was generally expected that higher levels of anxiety-relevant traits would be associated with a freeze response. Since these responses have also been documented among some PTSD victims, we expected that PTSD symptoms might be particularly predictive of freeze reactions.
1.2 Method
1.2.1 Participants
Participants took part in a longitudinal, primary prevention study (see Schmidt et al., in press for additional details). Exclusion criteria for this study include age restrictions (i.e., age range = 14–25) and the presence of any current Axis I diagnosis. Participants were recruited from the Columbus, OH metropolitan area school system (n = 46), the Ohio State University (n = 263), and the Columbus, OH community (n = 96). The sample was relatively young (age M = 19.3, SD = 3.9) with the majority being female (61%). The sample was also primarily white (74%) with 10% African-American, 9% Asian-American, 2% Hispanic, and 3% Other. Completion of college was the most frequently endorsed level of parental education with 30% of mothers and 29% of fathers finishing college.
1.2.2 Assessments
1.2.2.1 Interview Measures
1.2.2.1.1
Psychiatric diagnoses were made using structured diagnostic interviews (SCID-IP; First, Spitzer, Gibbon, & Williams, 1994). Interviews were conducted by advanced graduate students in clinical psychology who had received extensive training in SCID administration and scoring. A consensus method of diagnosis was used at weekly staff meetings where positive diagnostic findings were reviewed. The typical inter-rater reliability evaluation was not conducted due to participant selection criteria at baseline (i.e., absence of Axis I pathology).
1.2.2.1.2 Family History of Anxiety
Family history of anxiety disorders was assessed using a semi-structured interview that was embedded within the SCID. Similar methods of assessing family history have been used in prior studies of anxiety pathology (Plehn & Peterson, 2002; Yehuda, Halligan, & Bierer, 2001), and it appears to be a valid and reliable method (Andreasen et al., 1977). Following the anxiety disorders section of the SCID, the interviewer asked participants whether they were aware of any first degree relatives that had been diagnosed and treated for anxiety disorders or were likely to have suffered from these conditions despite a lack of treatment. A score of very likely, likely, or unlikely was assigned for mother, father and any siblings. In the present report, participants received a score of 1 for any “very likely” designation. The range of scores include (0 (negative across all family members) to 3 (positive for mother, father, and at least one sibling).
1.2.2.1.3 Panic Disorder Severity Scale (PDSS)
The PDSS is a semi-structured interview rating scale for panic disorder (Shear et al., 1997). In the present report, only the PDSS item indexing spontaneous panic frequency during the past month was utilized since the majority of items were not appropriate for a nonclinical sample.
1.2.2.2 Self-Report Measures
1.2.2.2.1 Acute Panic Inventory (API)
The API is a 17-item inventory for assessing symptoms of arousal associated with panic attacks (Liebowitz, Gorman, Fyer, Dillon, & Klein, 1984). The API has been used extensively in panic provocation studies (Fyer et al., 1987; Schmidt, Eggleston, Trakowski, & Smith, 2005). Participants rate the severity of each symptom from 0 (absent) to 3 (severe). The API includes a SUDS rating of self-reported anxiety (0 - No Anxiety, 100 - Extreme Anxiety). In addition to the standard API items, several additional items were added including one that assessed freeze (e.g., During the procedure (or resting period), I felt that I could not move) and another that assessed flight (e.g., During the procedure (or resting period), I felt that I wanted to flee). Each of these items was rated on a 0 (Not at all) to 100 (Extreme) scale.
1.2.2.2.2 Anxiety Sensitivity Index (ASI)
The ASI (Reiss et al., 1986) is a 16 item self-report measure of the fear of bodily sensations associated with arousal (Schmidt & Joiner, 2002; Zinbarg, Barlow, & Brown, 1997; Zvolensky, McNeil, Porter, & Stewart, 2001).
1.2.2.2.3 Impact of Events Scale – Revised (IES-R)
The IES-R is update of the popular IES that is used to measure intrusion and avoidance behaviors resulting from traumatic events (Weiss & Marmar, 1997).
1.2.2.2.4 Panic Attack
The API was used to index panic responding. In accordance with DSM-IV panic attack criteria describing the discrete and abrupt onset of fear and symptoms, the presence of a panic attack was determined by a composite index including: (a) reporting a 40 point increase in SUDS from baseline to challenge indicating a significant increase in anxiety, and (b) reporting four or more DSM symptoms as moderate to severe during the challenge. This method as well as similar methods of operationalizing panic response has been utilized in other reports (Schmidt, Eggleston, Trakowski, & Smith, in press; Schmidt, Miller, Lerew, Woolaway-Bickel, & Fitzpatrick, 2002)
1.2.2.2.5 Penn State Worry Questionnaire (PSWQ)
The PSWQ is a self-report measure of pathological worry (Brown et al., 1992; Gillis et al., 1995; Meyer et al., 1990).
1.2.2.2.6 Social Interaction Anxiety Scale (SIAS)
The SIAS assesses fears of social interaction and is well validated with good psychometric properties (Mattick & Clark, 1998).
1.2.2.2.7 Trait Anxiety (STAI)
The STAI assesses state and trait anxiety (Knight, Waal-Manning, & Spears, 1983). Only the trait scale, which measures general levels of anxiety, was utilized in the present study. Raw scores were used for analyses by summing responses to this scale (after reverse scoring negatively-worded items).
1.2.2.3 Challenge
1.2.2.3.1 20% CO2 Challenge
A 20% CO2-enriched (balance O2) biological challenge provided an index of fear responding to a novel stimulus. To control for different expectancies regarding the consequences of breathing CO2-enriched air, all participants were informed of several possible symptomatic consequences of breathing CO2-enriched air including: breathlessness, dizziness, chest pain, and tachycardia. Participants were not informed regarding the onset, timing, dose, or offset of the inhalation of CO2. Participants underwent a 20-s gas inhalation (20% CO2, 80% O2) administered through a continuous positive air pressure Downs C-Pap Mask with nose clip and head strap. Attached to one free port of a manually controlled 3-Way Stop Cock valve (Hans Rudolph, Inc.) was a 30-L meteorological balloon, which was inflated with the CO2 mixture. Participants breathed the CO2 gas directly from the balloon reservoir to minimize detection from pressurized CO2 to nonpressurized room air. The C-Pap mask was connected to a free 22-mm port of the Stop Cock Valve via 1.8-m of aerosol tubing and the remaining port was left unattached and fed room air. A remote device was used to control of the 3-Way Stop Cock valve for unobtrusive switching between CO2-enriched air and room air.
1.2.3 Procedure
These data are derived from a primary prevention study that included both an experimental and a prospective design. “At risk” participants (i.e., those with high anxiety sensitivity) with no current or recent psychiatric illness were randomly assigned to a risk reduction or control condition and followed for approximately 24 months (see Schmidt et al., (2007) for more details). The experimental manipulation was modeled after educational and behavioral procedures commonly used with patients with anxiety disorders. This presentation describes the nature of stress and the effects of stress on the body. The goal of the presentation is to emphasize the benign nature of stress in regard to its immediate effects on the body. This process is explained along with a description of behavioral exercises that are designed to correct interoceptive conditioning (Schmidt & Trakowski, 2004). Approximately half of the participants were randomized to a health and nutrition condition designed to control for any effects of general education and time spent with the experimenter. These participants received a computer-based presentation of equal length. In the present report, we statistically control for experimental condition in all relevant analyses.
Participants initially completed the SCID and, if eligible, the remaining interviews and self-report measures. Eligible participants were then randomly assigned to one of two conditions that are not relevant to the present report (see Schmidt et al., 2007, for details). As an additional check that the pattern of findings was not accounted for by the experimental manipulation, all relevant analyses were re-run after excluding participants assigned to the treatment condition. These analyses revealed the same pattern of findings. At this point, participants were led to a comfortable recliner in a dimly lit sound attenuated chamber and fitted with the CO2 apparatus (e.g., mask). Participants completed an API following a 5-minute adaptation period. After approximately 3 minutes, participants received a 20-s inhalation of CO2-enriched air. Immediately following the inhalation, participants returned to breathing normal room air and completed another API. Community and high school participants received $25 as compensation for the baseline assessment whereas college students received course credit.
1.3 Results
1.3.1 Prevalence of a Freeze Response to the Challenge
To evaluate the prevalence of a freeze response to the challenge, we examined the frequency distribution of the freeze item added to the API (see Table 1). Prior to the challenge, the majority of participants (84%) rated this item between 0 and 10 and only 5% gave a rating of 40 or greater. For comparative purposes, the baseline ratings on the desire to flee item indicated a comparable percentage of individuals endorsing both little or no desire to flee (82% scoring 10 or less) or moderate desire to flee (6% scoring 40 or greater).
Table 1.
Intercorrelations, Means and Standard Deviations among the Primary Variables of Interest at Baseline Assessment
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | M | SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. API total | - | 13.1 | 8.5 | |||||||||||
| 2. PDSS (PA frequency) | .10 ns | - | .1 | .3 | ||||||||||
| 3. IES-R | .41 | .02 ns | - | 5.3 | 1.9 | |||||||||
| 4. PSWQ | .50 | .08 ns | .48 | - | 43.9 | 14.4 | ||||||||
| 5. SIAS | .51 | .10 | .39 | .52 | - | 36.0 | 11.8 | |||||||
| 6. STAI | .32 | .40 | .40 | .43 | .38 | - | 44.6 | 4.5 | ||||||
| 7. Family History of Anxiety | .18 | .07 | .17 | .22 | .19 | .06 ns | - | .3 | .5 | |||||
| 8. API (Pre CO2; Highest Fear) | .25 | −.01 ns | .17 | .13 | .12 | .11 | .10 ns | - | 7.4 | 9.5 | ||||
| 9. API (Pre CO2; Desire to Escape) | .23 | .01 ns | .01 ns | .14 | .17 | .09 ns | .04 ns | .56 | - | 8.2 | 13.0 | |||
| 10. API (Pre CO2; Feeling Immobile) | .33 | −.02 ns | .15 | .14 | .24 | .12 | .10 ns | .51 | .58 | - | 7.2 | 13.3 | ||
| 11. API (Post CO2; Highest Fear) | .27 | .01 ns | .01 | .20 | .14 | .16 | .07 ns | .51 | .43 | .40 | - | 18.2 | 19.8 | |
| 12. API (Post CO2; Desire to Escape) | .26 | .05 ns | .12 | .20 | .15 | .14 | .02 ns | .42 | .57 | .42 | .83 | - | 17.7 | 22.2 |
| 13. API (Post CO2; Feeling Immobile) | .36 | .04 ns | .16 | .19 | .29 | .22 | .06 ns | .42 | .47 | .62 | .67 | .74 | 13.7 | 19.4 |
Note. N = range from 380 – 404. All ps < .05 except when noted nonsignificant (ns). API = Acute Panic Inventory; PDSS = Panic Disorder Severity Scale (Panic Attack Frequency); IES-R = Impact of Events Scale-Revised; PSWQ= Penn State Worry Questionnaire; SIAS = Social Interaction Anxiety Scale; STAI = Spielberger Trait Anxiety.
Following the challenge, a frequency distribution indicated that 69% reported little or no feelings of immobility (10 or less), 18% endorsed mild feelings of immobility (11–39), and 13% reported modest or greater feelings of immobility (40 or greater). The comparison item for fleeing indicated that 61% reported little or no desire to flee (10 or less), 19% endorsed a mild desire to flee (11–39), and 20% reported a modest or greater desire to flee (40 or greater). A repeated measures MANOVA evaluating changes in freeze and flee pre-post challenge indicated significant increases as a result of undergoing the challenge (F(1,349) = 82.97, p < .01, Partial eta2 = .19), significant differences between variables such that participants tended to report a greater desire to flee than to freeze (F(1,349) = 14.39, p < .01, Partial eta2 = .04) as well as a significant time × variable interaction (F(1,349) = 7.69, p < .01, Partial eta2 = .02). As expected, tests of the simple effects of the interaction revealed that while both variables increased significantly from baseline to challenge, the flee variable increased to a greater extent (Freeze: F(1, 349) = 60.60, p < .01, partial eta2 = .15; Flee: F(1, 398) = 104.18, p < .01, partial eta2 = .21 ). Consistent with hypothesis, these analyses suggest that flight responses are somewhat more common than freeze responses but that a sizable percentage of individuals endorsed significant immobility feelings during the stressor.
1.3.2 Descriptive Data and Zero-Order Relations among Theoretically-Relevant Variables
Table 1 provides correlations, means and standard deviations of the relevant predictor and criterion variables. Trait anxiety was significantly related to desire to flee as well as feeling immobile. Anxiety sensitivity also exhibited significant and somewhat stronger associations with these ratings (all ps < .01). Consistent with expectation, subjective anxiety was also strongly associated with flight and freeze ratings. Subjective anxiety ratings (SUDS) were highly associated with desire to flee (r = .83, p < .01) as well as perceived immobility (r = .68, p < .01). The flee and immobility items were also strongly associated (r = .74, p < .01). The family history of anxiety, history of panic attacks, and trauma-relevant variables, on the other hand, did not show significant associations with the flee or immobility variables.
1.3.3 Association between Freeze and Panic Symptoms
Based on the criteria utilized, approximately 6% (24/404) of the sample met criteria for panic challenge. Logistic regression analyses controlling for experimental condition as well as during the CO2 baseline levels of freeze indicated that panic was significantly associated with the freeze variable (Exp β = 1.06, 95% CI = 1.04–1.08; Wald = 28.36, p < .001). Similar analyses indicated that panic was also associated with the flight variable (Exp β = 1.09, 95% CI = 1.06–1.12; Wald = 36.3, p < .001). When both freeze and flight variables were simultaneously entered, only flight remained as a significant predictor (Exp β = 1.09, 95% CI = 1.05–1.13; Wald = 24.1, p < .001). Correlations between the freeze item and other API items were examined to provide a more detailed analysis of the association between freeze and other symptoms. These analyses indicated that 9 API items showed substantial correlations with the freeze item (r range = .45 – .60) compared to the remaining items, which showed a more modest association in the range of .20–.35. The majority of items that were more highly associated with freeze included those focused on cognitive symptoms of anxiety (e.g., confusion, unreality, detached, concentration, inner shakiness) as well as fear of losing control.
1.3.4 Predicting “Freeze” Responses
Hierarchical linear regression analyses were performed with each of the primary dependent measures (see Table 2). At level 1 in the model, experimental condition was included as a covariate (entered) to ensure any observed effects were not due to this factor. In addition, the baseline measure of “freeze” was entered to yield a prediction of reactivity. At level 2 in the model, the predictor variable of interest was entered. In this model, any observed effects for variables at level 2 in the model are unique and cannot be attributed to variance with factors in level 1 (Cohen & Cohen, 1983). Consistent with expectation, the pattern of findings suggested that higher levels of anxiety-related traits were associated with increased perceptions of immobility. Interestingly, the IES-R did not significantly predict freeze.
Table 2.
Anxiety Variables Predicting Perceived Immobility During a 20% CO2 Challenge
| Predicted Variable | Predictors in Set | ΔR2 | t for each Predictors | β |
|---|---|---|---|---|
| Post CO2 Inhalation API-Freeze | ||||
| Step 1 | .39 | |||
| Condition | −.69 | −.03 | ||
| Baseline-API-Freeze | 14.72** | .62 | ||
| Step 2a | ||||
| ASI | .02 | 4.05** | .18 | |
| Step 2b | ||||
| IES-R | .00 | 1.53 | .07 | |
| Step 2c | ||||
| SIAS | .01 | 3.50** | .15 | |
| Step 2d | ||||
| STAI | .01 | 3.58** | .15 | |
| Step 2e | ||||
| PSWQ | .01 | 2.34* | .10 | |
| Step 2f | ||||
| PDSS | .00 | 1.28 | .06 | |
Note. p<.05,
p<.01; API-Freeze = the degree to which you felt that you could not move; ASI = Anxiety Sensitivity Inventory; IES-R= Impact of Events Scale-Revised; SIAS= Social Interaction Anxiety Scale; STAI = Spielberger Trait Anxiety; PSWQ= Penn State Worry Questionnaire; PDSS = Panic Disorder Severity Scale (Panic Attack Frequency).
Since trait anxiety was a significant predictor and may represent an overarching vulnerability factor that encompasses elements of the other symptom measures, we conducted follow-up analyses that were similar but also included trait anxiety as a covariate. Thus, we evaluated whether the other psychological risk factors continued to add unique variance to the prediction of freeze. These analyses indicated that the ASI (β = .14, t = 3.11, p < .01) and the SIAS (β = .15, t = 3.49, p < .001) contributed to the prediction of freeze after controlling for trait anxiety. However, the PSWQ was no longer significantly associated with freeze after accounting for trait anxiety (β = .05, t = 1.11, p > .10).
1.3.5 Unique prediction of Freeze
Because highly anxiously individuals may have a response style that leads to a consistent overendorsement of anxiety-related variables, additional analyses were used to ascertain whether freeze response was able to predict fear and panic responses beyond the effects of desire to flee. Hierarchical regression analyses similar to those described above were used. In level 1, baseline fear, baseline freeze, and experimental condition were entered along with desire to flee during the procedure. At level 2, perceptions of immobility during the challenge were entered. As would be expected from the panic analyses reported above, immobility was not predictive of panic response. However, immobility was a significant incremental predictor of subjective anxiety to the challenge (β = .13, t = 2.18, p = .03).
1.4 Discussion
Although freeze responses are believed to be fundamental to the well-known fight-flight alarm action tendencies (Barlow, 2002), to our knowledge the current report is the first to empirically document a relationship between tonic immobility and a laboratory-based stressor in humans. This is a novel and potentially meaningful contribution to current theory, given that researchers have long hypothesized that tonic immobility may be a native biological response to extreme stress. Indeed, the current results are highly consistent with this conceptualization, inasmuch as we found that tonic immobility was most often reported by those individuals who also experienced significant fear during the challenge.
There was relatively little endorsement of freeze behavior prior to the challenge, with significant variability in this domain emerging only after the challenge. Specifically, the majority of nonclinical participants reported little or no feelings of immobility, with about 1/5 endorsing mild feelings of immobility, and approximately 13% reporting modest or greater feelings of immobility. Thus, even among nonclinical persons undergoing a 20% CO2 challenge, there appears to be variability in the experience of freezing. Further inspection of these data indicated that endorsement of a flight response was highly associated with the freeze response. Similarly, panic endorsement was highly associated with perceptions of tonic immobility as would be predicted by models of panic (Barlow, 2002). This suggests that panic and significant desire to flee appear to be fairly closely linked with perceptions of immobility. An interpretational problem arises with the high correlation between freeze and flight because these behaviors are potentially incompatible. One possibility is that the freeze item asked for the experience of immobility but the flight item asked for the wish to flee. It is conceivable that an individual may experience immobility, combined with the wish to flee (but not being able to execute it). Another explanation is that the responses, as per the model of Braca (2004), naturally follow each other. We attempted to dismantle these reactions statistically by evaluating whether perceptions of immobility could uniquely predict panic and fear responses while controlling for endorsement of desire to flee. Findings with regard to anxiety, but not panic, were consistent with the idea that immobility does add something unique to the desire to flee. More sophisticated designs are needed to more clearly delineated these associations. Overall, the pattern of findings is consistent with the view that the freeze response may be an integral part of the overall syndrome of psychological responses to acutely stressful circumstances.
Other findings indicated that theoretically-relevant individual difference factors are also related to perceptions of tonic immobility. However, the predictors did not demonstrate a great deal of specificity (i.e. nearly every anxiety-relevant variable was somewhat related to tonic immobility), which leaves open the possibility that the anxiety variables indexed were all tapping into a more general trait vulnerability. However, additional analyses suggest that after controlling for trait anxiety, social anxiety and anxiety sensitivity possessed some unique predictive relation to tonic immobility. Thus, it may be that these variables possess a unique relation to tonic immobility. However, it is more likely that these are particularly robust indicators of the general tendency to react fearfully to the CO2 challenge, which, in turn, is related to a freeze response. In any case, that anxiety-related individual differences moderate exhibition of the freeze response is consistent with previous primate studies indicating that high basal cortisol levels, which are related to heightened stress responses - are predictive of freeze responses in the presence of immediate threat (e.g., Kalin et al., 1998).
Some of our data suggested that reports of freeze were more highly associated with certain cognitive symptoms of anxiety (e.g., confusion, unreality, detached, concentration, inner shakiness). This leads to some very interesting speculation regarding whether freeze responses are also manifested cognitively (i.e., the cognitive system, together with the behavioral system, being shut down). There has been some speculation that a form of cognitive paralysis occurs due to immense cognitive demands that occur in the context of life-threatening situations or stressors (Leach, 2005). Unfortunately, there are currently many questions regarding cognitive paralysis, including what cognitive components might be involved in this. A better understanding of freeze in both the cognitive and behavioral domains is highly relevant to better understand extreme reactions during stress.
A number of interpretative caveats should be considered. As with any initial foray, this study possessed a number of limitations that warrant consideration but also provide potential fruitful directions for future research. First, we could not investigate the temporal relations as outlined by Bracha (2004) in terms of freeze-flight-fight-fright in this study. However, there were clear relationships between subjective anxiety and the tendency to want to flee as well as perceptions of tonic immobility, which is consistent with current alarm models that link these variables. A second limitation is that only perceptions of freeze were measured; the study did not include a behavioral demonstration of immobility. Additional work is needed to more carefully establish that behavioral immobility occurs in humans in the context of threats. In addition, it may be important to clarify the relationship between subjective perceptions of immobility and actual behavioral manifestations of immobility. Third, as with all non-experimental designs, causal relations cannot be unambiguously inferred, leaving the results open to a number of alternative interpretations. Forth, the present sample is limited in the sense that it is comprised of a relatively homogenous group of young adults who volunteered to participate in the study as part of a prevention-oriented investigation. Therefore, to rule out the possibility that the present results are somehow related to a self-selection bias among persons with these characteristics, it will be important for researchers to draw from a more diverse population as well as to utilize different recruitment tactics (e.g., random sampling procedures). Fifth, the experimental procedure informed participants that they could expect certain types of symptoms. The process of providing such information is likely to have attenuated fear responding to some degree (Schmidt & Telch, 1994). There is evidence to suggest that unanticipated or unpredictable CO2-induced sensations are likely to increase fear responding (Zvolensky et al., 2001). On the other hand, IRB restrictions on challenge research and ethical constraints on fear-induction procedures must be balanced with procedural considerations.
Finally, there may be other types of threat stressors or challenges that are more likely to provoke a freeze response. Thus, one could argue that it would be most appropriate to understand the present findings in reference to anxiety focused on bodily sensations and perceived intensity of symptoms but not intense terror/panic. We have attempted to provide a measure of panic responding that suggests that higher levels of anxiety or panic may be more intimately related to freeze responses. However, future work should employ other challenge procedures to evoke greater variability in anxiety and bodily sensations to better understand the relation between freeze and affect intensity. One way to conduct such work would be to sample clinical as well as nonclinical participants.
We based our study hypotheses and analyses on contemporary theories of fear behavior (Barlow, 2002). Building from this work, it would be worthwhile to extend this type of research to a broader array of processes related to fear behavior. For example, researchers could examine various parameters of freeze behavior during the challenge and how such responsivity relates to theoretically-relevant processes such as recovery time, duration of activation, and variability in other specific response components, as well as other cognitive and affective processes known to accompany fearful responses. Such emotional reactivity dimensions may inform researchers of clinically relevant individual variation in affective vulnerability related to freeze responses.
In conclusion, the present investigation addresses the nature of fear behavior in the context of a CO2 challenge. The present findings indicate that there is meaningful variability in freeze behavior among nonclinical participants and that this variability is related to other theoretically-relevant constructs such as subjective anxiety and panic. By continuing to utilize the integrative framework of emotion theory to understanding the nature of freeze responding, there likely will be new insights into anxiety and its disorders.
Figure 1.
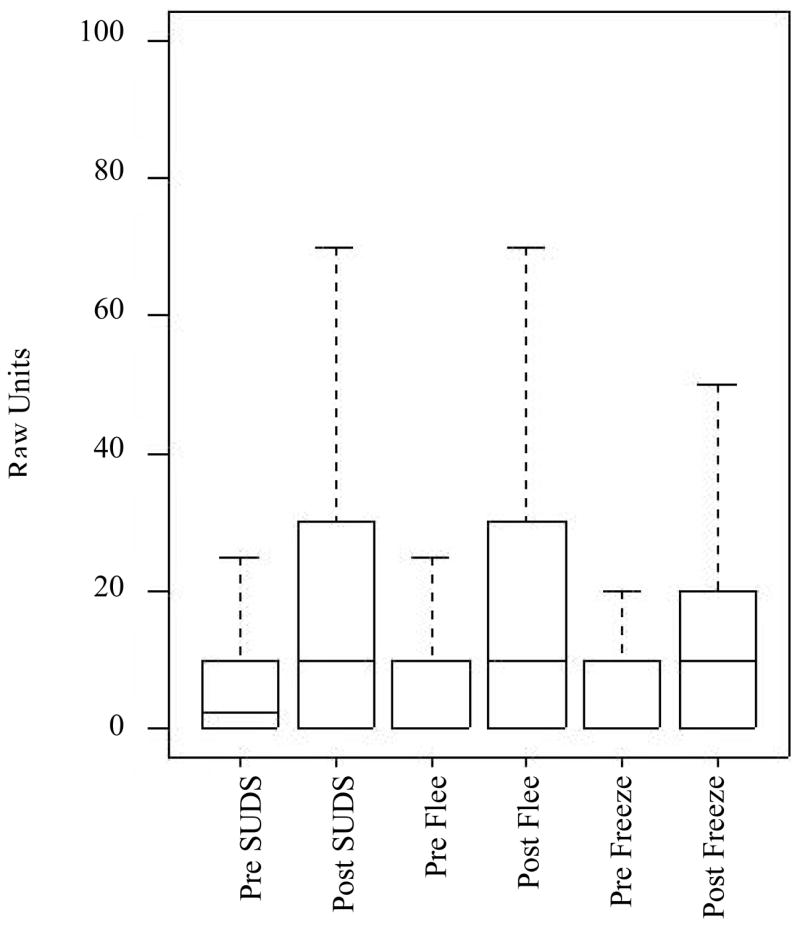
Distributions (raw unit means and interquartile range) indicating Fearful Responding (SUDS), Desire to Flee, and Perceptions of Immobility in Response to the CO2 challenge
Acknowledgments
This project was supported an Ohio Department of Mental Health research grant (737111) and by a National Institute Mental Health grant (MH62056).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
This PDF receipt will only be used as the basis for generating PubMed Central (PMC) documents. PMC documents will be made available for review after conversion (approx. 2-3 weeks time). Any corrections that need to be made will be done at that time. No materials will be released to PMC without the approval of an author. Only the PMC documents will appear on PubMed Central -- this PDF Receipt will not appear on PubMed Central.
Contributor Information
Norman B. Schmidt, Florida State University
J. Anthony Richey, Florida State University.
Michael J. Zvolensky, University of Vermont
Jon K. Maner, Florida State University
References
- Andreasen NC, Endicott J, Spitzer RL, Winokur G. The family history method using diagnostic criteria: Reliability and validity. Archives of General Psychiatry. 1977;34:1229–1235. doi: 10.1001/archpsyc.1977.01770220111013. [DOI] [PubMed] [Google Scholar]
- Arduino PJ, Gould JL. Is tonic immobility adaptive? Animal Behavior. 1984;32:921–923. [Google Scholar]
- Barlow DH. Anxiety and its disorders. 2. New York: Guilford Press; 2002. [Google Scholar]
- Bracha HS. Freeze, flight, fight, fright, faint: Adaptionist perspectives on the acute stress response spectrum. CNS Spectrums. 2004;9:679–685. doi: 10.1017/s1092852900001954. [DOI] [PubMed] [Google Scholar]
- Brown TA, Antony MM, Barlow DH. Psychometric properties of the Penn State Worry Questionnaire in a clinical anxiety disorders sample. Behaviour Research and Therapy. 1992;30:33–37. doi: 10.1016/0005-7967(92)90093-v. [DOI] [PubMed] [Google Scholar]
- Burgess AW, Holmstrom LL. Coping behavior of the rape victim. American Journal of Psychiatry. 1976;133:413–418. doi: 10.1176/ajp.133.4.413. [DOI] [PubMed] [Google Scholar]
- Cannon WB. The James-Lange theory of emotions: A critical examination and an alternative theory. American Journal of Psychology. 1927;39:106–124. [PubMed] [Google Scholar]
- Cannon WB. Bodily changes in pain, hunger, fear and rage. 2. New York: Appleton, Century, Crofts; 1929. [Google Scholar]
- Cohen J, Cohen P. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences. 2. Hillsdale, NJ: Erlbaum; 1983. [Google Scholar]
- First M, Spitzer R, Gibbon M, Williams J. Structured clinical interview for DSM-IV Patient Edition. (Version 2.0) New York: Biometrics Research Department; 1994. [Google Scholar]
- Fyer MR, Uy J, Martinez J, Goetz R. CO2 challenge of patients with panic disorder. American Journal of Psychiatry. 1987;144:1080–1082. doi: 10.1176/ajp.144.8.1080. [DOI] [PubMed] [Google Scholar]
- Galliano G, Noble LM, Travis LA, Puechl C. Victim reactions during rape/sexual assault: A preliminary study of the immobility response and its correlates. Journal of Interpersonal Violence. 1993;8:109–114. [Google Scholar]
- Gallup GG. Tonic immobility: The role of fear and predation. Psychological Record. 1977;27:41–61. [Google Scholar]
- Gillis MM, Haaga DA, Ford GT. Normative values for the Beck Anxiety Inventory, Fear Questionnaire, Penn State Worry Questionnaire, and Social Phobia and Anxiety Inventory. Psychological Assessment. 1995;7:450–455. [Google Scholar]
- Heidt JM, Marx BP, Forsyth JP. Tonic immobility and childhood sexual abuse: a preliminary report evaluating the sequela of rape-induced paralysis. Behavior Research and Therapy. 2005;43:1157–71. doi: 10.1016/j.brat.2004.08.005. [DOI] [PubMed] [Google Scholar]
- Kalin NH, Shelton SE, Rickman M, Davidson RJ. Individual differences in freezing and cortisol in infant and mother rhesus monkeys. Behavioral Neuroscience. 1998;112:251–254. doi: 10.1037//0735-7044.112.1.251. [DOI] [PubMed] [Google Scholar]
- Korte SM, Koolhaas JM, Wingfield JC, McEwen BS. The Darwinian concept of stress: Benefits of allostasis and costs of allostatic load and the trade-offs in health and disease. Neuroscience & Biobehavioral Reviews. 2005;29:3–38. doi: 10.1016/j.neubiorev.2004.08.009. [DOI] [PubMed] [Google Scholar]
- Knight RG, Waal-Manning HJ, Spears GF. An examination of the psychometric properties of the crown-crisp experiential index. New Zealand Journal of Psychology. 1983;12:53–56. [Google Scholar]
- Lang PJ. The varieties of emotional experience: A meditation on James-Lange theory. Psychological Review. 1994;101:211–221. doi: 10.1037/0033-295x.101.2.211. [DOI] [PubMed] [Google Scholar]
- Leach J. Cognitive paralysis in an emergency: The role of the supervisory attentional system. Aviation Space and Environmental Medicine. 2005;76:134–136. [PubMed] [Google Scholar]
- Liebowitz MR, Gorman JM, Fyer AJ, Dillon DJ, Klein DF. Effects of naltrexone on patients with panic attacks. American Journal of Psychiatry. 1984;141:995–997. doi: 10.1176/ajp.141.8.995. [DOI] [PubMed] [Google Scholar]
- Mattick RP, Clarke JC. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behaviour Research and Therapy. 1998;36:455–470. doi: 10.1016/s0005-7967(97)10031-6. [DOI] [PubMed] [Google Scholar]
- Mcnally RJ. Panic Disorder: A Critical Analysis. New York: Guilford Press; 1994. [Google Scholar]
- Meyer TJ, Miller ML, Metzger RL, Borkovec TD. Development and validation of the Penn State Worry Questionnaire. Behaviour Research & Therapy. 1990;28:487–495. doi: 10.1016/0005-7967(90)90135-6. [DOI] [PubMed] [Google Scholar]
- Mezey GC, Taylor PJ. Psychological reactions of women who have been raped- A descriptive and comparative study. British Journal of Psychiatry. 1998;152:330–339. doi: 10.1192/bjp.152.3.330. [DOI] [PubMed] [Google Scholar]
- Plehn K, Peterson RA. Anxiety sensitivity as a predictor of the development of panic symptoms, panic attacks, and panic disorder: A prospective study. Journal of Anxiety Disorders. 2002;16:455–474. doi: 10.1016/s0887-6185(02)00129-9. [DOI] [PubMed] [Google Scholar]
- Reiss S, Peterson RA, Gursky DM, McNally RJ. Anxiety sensitivity, anxiety frequency, and the prediction of fearfulness. Behaviour Research and Therapy. 1986;24:1–8. doi: 10.1016/0005-7967(86)90143-9. [DOI] [PubMed] [Google Scholar]
- Scaer RC. The neurophysiology of dissociation and chronic disease. Applied Psychophysiology & Biofeedback. 2001;26:73–91. doi: 10.1023/a:1009571806136. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Eggleston AM, Woolaway-Bickel K, Fitzpatrick KK, Vasey MW, Richey JA. Anxiety Sensitivity Amelioration Training (ASAT): A Longitudinal Primary Prevention Program Targeting Cognitive Vulnerability. Journal of Anxiety Disorders. 2007;21:302–319. doi: 10.1016/j.janxdis.2006.06.002. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Eggleston AM, Trakowski JH, Smith JA. Does coping predict CO2-induced panic in patients with panic disorder. Behaviour Research and Therapy. 2005;10:1311–1319. doi: 10.1016/j.brat.2004.09.007. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Joiner T., Jr Structure of the anxiety sensitivity index: Psychometrics and factor structure in a community sample. Journal of Anxiety Disorders. 2002;16:33–49. doi: 10.1016/s0887-6185(01)00087-1. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Miller J, Lerew DR, Woolaway-Bickel K, Fitzpatrick K. Imaginal provocation of panic in patients with panic disorder. Behavior Therapy. 2002;33:149–162. [Google Scholar]
- Schmidt NB, Storey J, Greenberg BD, Santiago HT, Li Q, Murphy DL. Evaluating gene × psychological risk factor effects in the pathogenesis of anxiety: A new model approach. Journal of Abnormal Psychology. 2000;109:308–320. [PubMed] [Google Scholar]
- Schmidt NB, Telch MJ. Role of fear of fear and safety information in moderating the effects of voluntary hyperventilation. Behavior Therapy. 1994;25:197–208. [Google Scholar]
- Schmidt NB, Trakowski J. Interoceptive assessment and exposure in patients with panic disorder: A descriptive study. Cognitive and Behavioral Practice. 2004;11:81–91. [Google Scholar]
- Shear MK, Brown TA, Barlow DH, Money RDE, Woods SW, Sholomskas DE, Woods SW, Gorman JM, Papp LA. Multicenter collaborative panic disorder severity scale. American Journal of Psychiatry. 1997;154:1571–1575. doi: 10.1176/ajp.154.11.1571. [DOI] [PubMed] [Google Scholar]
- Suarez SD, Gallup GG. Tonic immobility as a response to rape in humans: A theoretical note. The Psychological Record. 1979;29:315–320. [Google Scholar]
- Weiss DS, Marmar CR. The impact of event scale – revised. In: Wilson JP, Keane TM, editors. Assessing psychological trauma and PTSD. New York: Guildford; 1997. pp. 399–411. [Google Scholar]
- Yehuda R, Halligan SL, Bierer LM. Relationship of parental trauma exposure and PTSD to PTSD, depressive and anxiety disorders in offspring. Journal of Psychiatric Research. 2001;35:261–270. doi: 10.1016/s0022-3956(01)00032-2. [DOI] [PubMed] [Google Scholar]
- Zinbarg RE, Barlow DH, Brown TA. Hierarchical structure and general factor structure saturation of the Anxiety Sensitivity Index: Evidence and implications. Psychological Assessment. 1997;9:277–284. [Google Scholar]
- Zvolensky MJ, Eifert GH. A review of psychological factors/processes affecting anxious responding during voluntary hyperventilation and inhalations of carbon dioxide-enriched air. Clinical Psychology Review. 2001;21:375–400. doi: 10.1016/s0272-7358(99)00053-7. [DOI] [PubMed] [Google Scholar]
- Zvolensky MJ, Eifert GH, Lejuez CW. Offset control during recurrent 20% carbon dioxide-enriched air induction: relation to individual difference variables. Emotion. 2001;1:148–165. doi: 10.1037/1528-3542.1.2.148. [DOI] [PubMed] [Google Scholar]
- Zvolensky MJ, McNeil DW, Porter CA, Stewart SH. Assessment of anxiety sensitivity in young American Indians and Alaska natives. Behaviour Research and Therapy. 2001;39:477–493. doi: 10.1016/s0005-7967(00)00010-3. [DOI] [PubMed] [Google Scholar]