

Summary
Though stuttering is manifest in its motor characteristics, the cause of stuttering may not relate purely to impairments in the motor system as stuttering frequency is increased by linguistic factors, such as syntactic complexity and length of utterance, and decreased by changes in perception, such as masking or altering auditory feedback. Using functional and diffusion imaging, we examined brain structure and function in the motor and language areas in a group of young people who stutter. During speech production, irrespective of fluency or auditory feedback, the people who stuttered showed overactivity relative to controls in the anterior insula, cerebellum and midbrain bilaterally and underactivity in the ventral premotor, Rolandic opercular and sensorimotor cortex bilaterally and Heschl’s gyrus on the left. These results are consistent with a recent meta-analysis of functional imaging studies in developmental stuttering. Two additional findings emerged from our study. First, we found overactivity in the midbrain, which was at the level of the substantia nigra and extended to the pedunculopontine nucleus, red nucleus and subthalamic nucleus. This overactivity is consistent with suggestions in previous studies of abnormal function of the basal ganglia or excessive dopamine in people who stutter. Second, we found underactivity of the cortical motor and premotor areas associated with articulation and speech production. Analysis of the diffusion data revealed that the integrity of the white matter underlying the underactive areas in ventral premotor cortex was reduced in people who stutter. The white matter tracts in this area via connections with posterior superior temporal and inferior parietal cortex provide a substrate for the integration of articulatory planning and sensory feedback, and via connections with primary motor cortex, a substrate for execution of articulatory movements. Our data support the conclusion that stuttering is a disorder related primarily to disruption in the cortical and subcortical neural systems supporting the selection, initiation and execution of motor sequences necessary for fluent speech production.
Keywords: speech dysfluency, functional imaging, diffusion tensor imaging, basal ganglia, ventral premotor cortex
Persistent developmental stuttering is a disorder of speech fluency affecting approximately 1% of the adult population (Andrews and Harris, 1964; Bloodstein, 1995). The prevalence of stuttering, however, is even higher than this with estimates of between 4 and 5% of the population having stuttered at some point during development (Andrews and Harris, 1964). Given its prevalence and the opportunity to compare people who persist with those who recover, the study of developmental stuttering offers the possibility to explore the neural basis of speech production more generally, as well as providing insights into mechanisms of plasticity, reorganisation or recovery of function. Unlike patient groups with impairments of speech and language due to genetic abnormalities (e.g. the KE family; Watkins et al., 2002a), brain lesions or other neurological disease, people who stutter are generally healthy, and cognitively, psychiatrically and neurologically unimpaired.
Many view stuttering as primarily a motor-speech disorder, sharing characteristics with other disorders of motor control such as Tourette’s syndrome, dystonia, and Parkinson’s disease (Ludlow and Loucks, 2003). There is evidence, however, that linguistic factors play a role in stuttering frequency (Karniol, 1995). Stuttering occurs more frequently at the beginning of sentences, particularly if the planned utterances are long (Jayaram, 1984) or syntactically complex (Melnick and Conture, 2000) and rarely on single word utterances or word lists. Changes in sensory inputs can dramatically ameliorate the characteristic dysfluencies associated with stuttering. Fluency is enhanced by speaking with auditory masking (white noise), to a rhythmic cue, in unison with other speakers and by singing or by altering auditory feedback of the speaker’s own speech such that it is slightly delayed or changed in frequency (Andrews et al., 1983, for review; Kalinowski and Saltuklaroglu, 2003). The enhancement of fluency by altered perceptual inputs also provides an opportunity to explore mechanisms of sensorimotor integration in relation to speech production.
Despite its prevalence in the healthy population, the neural basis of developmental stuttering is poorly understood. Initially, PET and more recently, functional MRI, were used to examine brain function during fluent and dysfluent speech in people who stutter (Braun et al., 1997; De Nil et al., 2000; De Nil et al., 2003; Fox et al., 1996; Fox et al., 2000; Ingham, 2001; Neumann et al., 2003; Van Borsel et al., 2003). A recent meta-analysis of these studies identified three “neural signatures” of stuttering: people who stutter show more activity than fluent-speaking controls in the cerebellar vermis and in the right anterior insular cortex with an “absence” of activity in the auditory cortices in superior temporal lobe (Brown et al., 2005). These abnormal levels of activity were observed during speech production irrespective of the presence or absence of stuttered speech during scan acquisition. Surprisingly, the meta-analysis did not reveal abnormal levels of activity in the basal ganglia circuitry despite early imaging work on small samples showing abnormal metabolism in these structures in developmental stuttering (Wu et al., 1995; Wu et al., 1997).
Consistent with findings in other developmental disorders such as dyslexia, brain asymmetry both globally and locally in the planum temporale is abnormal in developmental stuttering (Foundas et al., 2003). Furthermore, subtypes of stuttering can be identified according to planum temporale asymmetry and these subtypes respond differently to the fluency-enhancing effects of altered auditory feedback (Foundas et al., 2004). In the inferior frontal gyrus, abnormal and extra diagonal sulci (usually a shallow sulcus in the posterior part of Broca’s area i.e. pars opercularis) are reported in the left or right hemisphere or both in people who stutter (Foundas et al., 2001). Also, extra sulci are described in the opercular cortex (the dorsal surface of the Sylvian fissure) extending from the inferior frontal lobe to the inferior parietal lobe; these were also noted in either left or right hemispheres in the majority, but not all, of people who stutter. A recent study, however, describes abnormal numbers of sulci in the upper bank of the right Sylvian fissure (and not the left) in a group of males who stutter; this study also reported no differences compared to controls in global or local hemispheric asymmetries (Cykowski et al., 2007).
The aforementioned studies used high-resolution images of brain structure to assess the size and shape of cortical areas. Diffusion imaging can be used to assess the integrity of white matter tracts by measuring the preferred direction of diffusion of water in each voxel of the image. Water diffuses most easily along the long axis of a fibre tract, so the signal obtained is used to infer the principle direction of fibres at that location. Using a voxel-wise analysis of diffusion data across the whole brain, one study found reduced white matter integrity in the left Rolandic (central) operculum in people who stutter compared to controls (Sommer et al., 2002). The area of significant difference was located in the white matter underlying the putative sensorimotor representation of the articulators. Similarly, a reduction in white matter integrity in the left superior longitudinal fasciculus was described in children who stutter aged 8-12 years (Chang et al., 2006). This result replicates and extends the original finding in this area (Sommer et al., 2002). It is interesting to speculate on the relationship between this apparently weak or interrupted white matter tract and the functional brain abnormalities considered characteristic of stuttering. The location is suggestive of a disruption in the communication between areas important for auditory perception and motor control of speech. One study describes increased brain activity in the Rolandic operculum following stuttering therapy, suggesting that tissue close to the area of white matter abnormality can compensate in recovery from stuttering (Neumann et al., 2005).
Here, we examined brain structure and function and the relationship between the two in a group of adolescents and young people who stutter. We hypothesized that people who stutter would show functional or structural abnormalities in either motor or language areas of the brain or both consistent with current theories of deficits in the execution and planning of speech in stuttering (EXPLAN; Howell, 2004; Howell and Au-Yeung, 2002). Also, we wished to examine the relationship between functionally abnormal brain areas and the underlying structure. We used functional MRI to measure the brain activity during sentence reading. A sparse-sampling design (Hall et al., 1999) was used so that participants spoke during a 7-s silent period between scans. This ensured that speech-related movement artefacts did not contaminate images and that participants could clearly hear the feedback. As the blood oxygenation-level dependant (BOLD) response measured by functional MRI takes 4-5s to peak (Belin et al., 1999; Glover, 1999), brain images acquired at the end of the 7-s silent period coincide with the peak of the brain’s response to the speech produced during that period. Participants read sentences aloud and received auditory feedback that was normal, delayed or frequency-shifted; the latter two conditions typically enhance fluency in people who stutter. Brain structure was examined using a measure of white matter integrity, fractional anisotropy, derived from diffusion tensor images. A novel analysis technique (Tract-Based Spatial Statistics; TBSS; Smith et al., 2006) was applied to this data. TBSS overcomes many of the problems inherent in standard voxel-wise methods of whole-brain analysis of diffusion data, such as averaging of data from grey and white matter by smoothing and problems with between-subject variance in brain structure. The results of the separate functional and structural analyses were compared to assess the relationship between the two.
Methods
Participants
Twelve subjects with developmental stuttering (people who stutter, PWS: 8M:4F; aged 14-27 years, avg. 18y; 1 left-hander) and 10 age- and sex-matched controls (Controls: 6M:4F; aged 14-27 years, avg. 18y; all right-handed) were scanned using functional MRI. In addition, a further 8 subjects (5 PWS, 3 Controls) were scanned with diffusion imaging (PWS: 12M:5F; avg. age 17y; Controls: 8M:5F; avg. age 18 y). The subjects with developmental stuttering ranged in stuttering severity from mild to severe as assessed with the Stuttering Severity Instrument-3 (Riley, 1994); avg. 22.3, range 8-37). The study was conducted under ethical approval from the Central Office for NHS Research Ethics Committees and the Research Ethics Committee for University College London. Subjects gave informed consent or assent (if younger than 16 years, parental consent was also obtained) in accordance with the Declaration of Helsinki and were compensated for their time.
Functional imaging
Functional MRI data were obtained using a 3-T Varian-Siemens scanner with a birdcage head coil. Whole-head T2*-weighted echo-planar images (TE=30msec), acquired every 10s with a delay of 7s (i.e. sparse sampling; Hall et al., 1999), comprised 3-s acquisition of 32 4-mm axial slices (in-plane resolution 4mm × 4mm). During the 7-s silent delay between measurements, subjects saw a stimulus via prism glasses that was either a meaningful sentence or a row of Xs and they read the sentences aloud. Sentences were selected from recommended lists (IEEE, 1969) and varied in syllable length from 7 to 11 syllables (average 9 syllables). Speech was recorded using an MRI-compatible microphone and fed back over headphones to the subjects via a real-time digitizer. Feedback was either (i) normal (ii) delayed by 200ms or (iii) frequency-shifted by half an octave upwards. The average sentence length did not differ among conditions (9 syllables). Twenty-four volumes were acquired under each of the three conditions and the baseline condition presented in a fixed pseudorandom order for a total of 96 volumes (16 mins).
The functional images were analysed using the FMRIB Software Library (FSL; http://www.fmrib.ox.ac.uk/fsl). Motion corrected images were unwarped using a fieldmap and PRELUDE and FUGUE software running in FSL (Jenkinson, 2003). These were then affinely registered via a T1-weighted structural image (1mm3 voxels; FLASH sequence TR=12msecs, TE=5.65msec, flip angle = 19 degrees) to the MNI-152 template, smoothed with an 8-mm full-width at half maximum smoothing kernel and analysed using the general linear model. For individual subjects, statistical maps were generated to show patterns of activation during each condition separately relative to baseline. Group analyses were carried out using FMRIB’s Local Analysis of Mixed Effects stage 1 only (Woolrich et al., 2004). The differences in activity between the PWS and Control groups showed very similar patterns in all of the feedback conditions, suggesting that these differences were common to speech production by PWS and did not reflect the type of feedback received or the fluency attained. The statistical significance of these group differences was established, therefore, with an F-test across the three conditions of feedback. In this analysis peaks were considered significant at a threshold of Z>3.78 (p<0.05, corrected). The peak location and Z value for areas identified as showing a group difference in this F-test are reported (the null hypothesis of this test is that there are no differences between the two groups in any of the three conditions).
Diffusion tensor imaging
Diffusion images were acquired using a 1.5T Siemens Sonata imaging system with a maximum gradient strength of 40 mTm-1. Two sets of echo-planar images of the whole head were acquired (53 × 2.5 mm axial slices, in-plane resolution 2.5mm2). Each set comprised 3 non-diffusion-weighted and 60 diffusion-weighted images acquired with a b-value of 1000 smm-2 uniformly distributed across 60 gradient directions. Diffusion data were preprocessed using FMRIB’s Diffusion Toolbox (v. 1.0). Images were corrected for eddy currents and head motion by using affine registration to the non-diffusion volumes, data were averaged across the two acquisitions to improve signal to noise, and images were created of fractional anisotropy (FA). Voxel-wise statistical analysis of the FA data was carried out using TBSS (Smith et al., 2006). TBSS nonlinearly registers the diffusion images to a target image. It then creates a skeleton of white matter by thinning the average of all the data to find a representation of all tracts, which are common to all the subjects. TBSS projects each subject’s FA data onto the mean FA tract skeleton. The highest data value near the skeleton in each subject is transferred to the skeleton for analysis. The data for the two groups were compared with a t-test at each voxel location in the skeleton. A statistical threshold of t(28)>3.1 (p<0.0025, uncorrected) was used for these analyses.
Results
Functional imaging
Functional brain imaging during normal, delayed and frequency-shifted feedback conditions revealed similar patterns of activation relative to the baseline conditions in controls (N=10) and people who stutter (PWS; N=12). These comprised left inferior frontal gyrus (IFG) extending to the opercular surface and ventral premotor cortex, bilateral pre-supplementary, supplementary and cingulate motor areas, sensorimotor cortex, superior temporal gyrus and sulcus, left thalamus, and superior cerebellum. The activity in this network is consistent with overt speech production and auditory perception of that production.
A comparison of the PWS and control groups revealed a number of differences in brain activity that were seen commonly in each of the feedback conditions. An F-test across the group difference images for the three contrasts comparing speech to baseline revealed that the PWS group had significantly (Z>3.78, p<0.05 corrected) lower activity than the controls in the left ventral premotor cortex, right Rolandic (central) opercular cortex (ventral to the left premotor peak), left and right sensorimotor cortex, spanning the central sulcus at the level of the face representation (Fox et al., 2001), and left anteromedial Heschl’s gyrus (see Figure 1 and Table 1). In contrast, the PWS group had significantly greater activity than controls in the left cingulate sulcus, left and right anterior insula extending to the putamen on the left, a midbrain region with peaks bilaterally at the level of the substantia nigra, but encompassing also the pedunculopontine nucleus, subthalamic nucleus and red nucleus, and the left and right posterior lobes of the cerebellum (see Figure 1 and Table 1).
Figure 1. Functional brain differences between controls and people who stutter during speech production with auditory feedback.

Results of functional MRI during speech production in PWS compared to Controls. Coloured maps of the Z-statistic for the F-test across the three feedback conditions are overlaid onto a single representative T1-weighted brain image from the subjects studied (thresholded at Z>3.5 for visualisation). Blue indicates areas where PWS had significantly less activity than Controls in at least one of the feedback conditions. Yellow/orange indicates areas where PWS had significantly more activity than controls in at least one of the feedback conditions. For axial and coronal slices the left side of the brain is shown on the left. Numbers next to each image indicate the coordinate in mm of that slice in x (for sagittal), y (for coronal) and z (for axial) relative to the orthogonal planes through the anterior commissure. vPMC - ventral premotor cortex; cOp - central operculum; SMC - sensorimotor cortex; CgS - cingulate sulcus; sn/stn/rn - substania nigra or subthalamic nucleus or red nucleus; pCbll - posterior lobe of cerebellum; Ins - insula; HG - Heschl’s gyrus.
Table 1.
Brain areas showing differences between people who stutter and controls in activity during speech across the three feedback conditions
| Brain area | X | Y | Z | z-statistic+ |
|---|---|---|---|---|
| Controls greater than PWS | ||||
| Left ventral premotor cortex | -54 | 2 | 24 | 4.14 |
| Right ventral premotor cortex / central (Rolandic) operculum | 66 | 2 | 16 | 4.66 |
| Left sensorimotor cortex (face area)* | -48 | -16 | 46 | 4.20 |
| Right sensorimotor cortex (face area)* | 44 | -10 | 44 | 5.98 |
| Left anteromedial Heschl’s gyrus | -48 | -10 | 6 | 4.08 |
| PWS greater activity than controls | ||||
| Left cingulate sulcus | -10 | 28 | 26 | 3.68 |
| Right anterior insula (dorsal) / putamen* | 30 | 16 | 10 | 4.47 |
| Left anterior insula (dorsal)* | -34 | 12 | 14 | 4.23 |
| Right anterior insula (ventral) | 32 | 14 | -14 | 4.23 |
| Left midbrain (see text for details)* | -8 | -20 | -10 | 5.33 |
| Right midbrain (see text for details)* | 6 | -18 | -12 | 5.36 |
| Left posterior lobe of cerebellum* | -6 | -68 | -48 | 3.97 |
| Right posterior lobe of cerebellum* | 8 | -68 | -48 | 4.49 |
Regions showing symmetrical bilateral differences in activity
Z-statistic for the F-test carried out across 3 conditions of feedback (Z>3.78 is significant at p<0.05, corrected)
The comparisons of delayed or frequency-shifted feedback with normal feedback revealed increased activity bilaterally in the superior temporal cortex in both groups. During delayed feedback relative to normal feedback, both groups showed increased activity in the right inferior frontal cortex. There were no significant differences between the PWS group and the controls for the comparisons between feedback conditions (i.e. the interaction between group and feedback condition; cluster threshold Z>2.3, p<0.05 corrected, or voxel threshold Z>3.1, p<0.001 uncorrected).
Analysis of speech recorded during scanning revealed that the PWS group produced significantly more stuttered syllables than the control group (F(1,20)=6.40, p=0.02; PWS mean 7.6%, SD 8.1; Controls mean 1.8%, SD 1.3) and that both groups produced significantly more stuttered syllables during delayed compared to frequency-shifted auditory feedback (F(1.55,40)=4.32, p<0.031; feedback: normal, mean 4.9%, SD 5.7; delayed, mean 6.6%, SD 8.4; frequency-shifted, mean 3.4%, SD 5.3). There was no difference in the rate of stuttering between the normal feedback and the other two conditions and the interaction between group and feedback condition was not significant (see Table 2). Sentence duration did not differ between PWS and Controls. The durations of sentences spoken with delayed feedback were significantly longer than those spoken with frequency-shifted feedback, which were significantly longer than those spoken with normal feedback (F(2,40)=18.84, p<0.001; feedback: normal, mean 2.87s, SD 0.6; delayed mean 3.34s, SD 0.7; frequency-shifted mean 3.03s, SD 0.5). The interaction between group and feedback condition for sentence duration was not significant (see Table 2).
Table 2.
Data from speech recordings made under different feedback conditions during scanning.
| Measure | PWS (N=12) | CON (N=10) |
|---|---|---|
| Stuttered syllables (%) | ||
| Normal | 7.37 (1.94) | 1.91 (0.37) |
| Delayed | 9.99 (2.98) | 2.56 (1.51) |
| Frequency-shifted | 5.45 (1.90) | 1.00 (0.25) |
| Sentence duration (s) | ||
| Normal | 3.12 (0.22) | 2.58 (0.05) |
| Delayed | 3.57 (0.27) | 3.08 (0.07) |
| Frequency-shifted | 3.19 (0.18) | 2.85 (0.05) |
Structural imaging
Given our a priori hypothesis that the areas of the brain affected in stuttering would be language and motor areas and their homologues in the right hemisphere, we report differences in FA in tracts associated with those areas at a threshold of t(28)>3.1 (p<0.0025, one-tail, uncorrected); many of these areas showed group differences bilaterally (see Table 3 and Figure 2). The joint probability of finding these bilateral differences can be considered p<0.00252. The PWS group (N=17) had significantly lower FA compared to the Control group (N=13) in white matter underlying pars orbitalis in the right IFG, left and right posterior IFG, left and right precentral gyrus (middle), left and right ventral premotor cortex, right posterior supramarginal gyrus and left dorsal supramarginal gyrus, in the right and left cerebellar white matter and in white matter tracts such as the right corticospinal tract (at the level of the midbrain), the medial lemniscus and the right middle cerebellar peduncle. The PWS group had higher FA than controls in the white matter underlying left posterior IFG (ventral to the area of decrease described above), right postcentral gyrus and right supramarginal gyrus.
Table 3.
Differences between people who stutter and controls in structural integrity of white matter tracts
| White matter region | X | Y | Z | t-statistic |
|---|---|---|---|---|
| PWS lower FA than Controls | ||||
| Right inferior frontal gyrus (pars orbitalis) | 47 | 36 | -10 | 4.36 |
| Left inferior frontal gyrus (posterior)* | -43 | 25 | 14 | 4.75 |
| Right inferior frontal gyrus (posterior)* | 44 | 20 | 12 | 4.6 |
| Right precentral gyrus * | 59 | 7 | 33 | 3.37 |
| Left precentral gyrus * | -51 | 4 | 32 | 4.04 |
| Right ventral premotor* | 55 | 4 | 13 | 3.56 |
| Left ventral premotor* | -54 | 0 | 20 | 3.39 |
| Right corticospinal tract (top of midbrain) | 17 | -15 | -8 | 3.28 |
| Right supramarginal / angular gyrus | 46 | -46 | 28 | 3.90 |
| Left supramarginal gyrus | -40 | -56 | 40 | 4.13 |
| Left dorsal pons (medial lemniscus) * | -6 | -37 | -34 | 4.66 |
| Right dorsal pons (medial lemniscus) * | 5 | -37 | -36 | 3.55 |
| Right middle cerebellar peduncle | 13 | -42 | -38 | 4.42 |
| Right anterior cerebellar lobe | 36 | -49 | -30 | 3.71 |
| Left posterior cerebellar lobe* | -21 | -63 | -39 | 3.56 |
| Right posterior cerebellar lobe* | 27 | -67 | -37 | 3.80 |
| PWS higher FA than Controls | ||||
| Left inferior frontal gyrus (posterior and ventral) | -47 | 24 | 4 | 3.57 |
| Right postcentral gyrus | 45 | -19 | 44 | 4.58 |
| Right supramarginal gyrus | 45 | -37 | 35 | 4.03 |
Regions showing symmetrical bilateral differences in FA
Figure 2. Structural white matter differences between controls and people who stutter.

Results of analysis of diffusion imaging data in PWS compared to Controls. The skeleton (green) is overlaid onto the average fractional anisotropy (FA) image of the subjects studied. Blue indicates areas where PWS had lower FA than controls. Yellow/orange indicates areas where PWS had higher FA than controls. (Note: statistical maps were thresholded at t(28)>3.1 (p<0.0025, one-tail) and the surviving clusters of voxels were dilated for visualisation purposes only). Numbers above each image indicate the coordinate in mm of that slice in y relative to the vertical coronal plane through the anterior commissure. See Table 1 for further details.
By superimposing the statistical maps of the comparisons between PWS and Controls we were able to demonstrate the relationship between the functional and structural differences. The reduced functional activations in the left ventral premotor cortex and even more ventrally located right premotor (Rolandic/central opercular) cortex in the PWS group lay directly above regions of white matter showing reduced integrity in that group (see Figure 3).
Figure 3. Structural and functional abnormalities in the premotor cortex and underlying white matter in people who stutter.
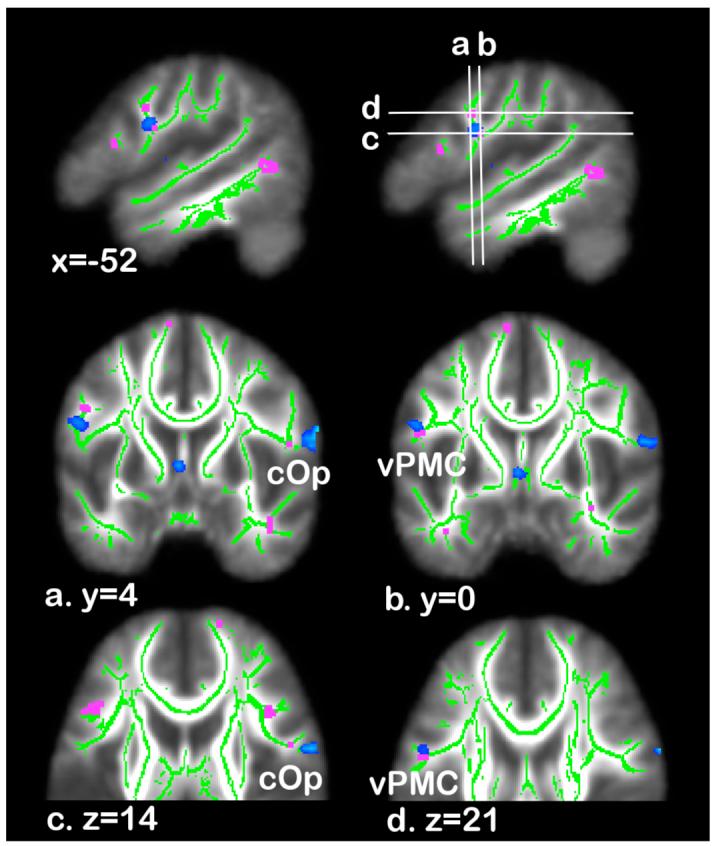
Functional and structural imaging differences between controls and PWS. The skeleton (green) is overlaid onto the average fractional anisotropy (FA) image of the subjects studied. Blue indicates areas where PWS had significantly less activity than controls during speech production, across the three feedback conditions (see Figure 1 for details). Pink indicates areas where PWS had lower FA than controls (see Figure 2 for details). Sagittal image in the top right of figure shows the position of the axial and coronal slices shown below (a.-d.). For axial and coronal slices the left side of the brain is shown on the left. vPMC - ventral premotor cortex; cOp - central operculum.
Discussion
Using a combination of structural and functional brain image analysis in people who stutter, we have identified a relationship between abnormal brain function of the ventral premotor cortex in both hemispheres and the integrity of white matter connections lying underneath this area. The affected areas were not perfectly symmetrical in the left and right hemispheres, being more ventral and anterior on the right than on the left (see central operculum in Table 1 and Figure 1). In the monkey, ventral premotor cortex (Brodmann’s area 6) and adjacent area 44 receive inputs from the supramarginal gyrus and adjacent parietal operculum (Petrides and Pandya, 2002) and the posterior insula (Mesulam and Mufson, 1982). Also, ventral premotor cortex projects to the primary motor cortex in the precentral sulcus/gyrus (area 4) (Barbas and Pandya, 1987). Disruption of white matter tracts underlying the ventral premotor cortex is likely to interfere with the integration of sensory and motor information necessary for fluent speech production. Brain activity in the left frontal precentral cortex (-48 -4 32), at a location slightly posterior and dorsal to the peak in ventral premotor cortex reported here (-54 2 24), is reported to be significantly lower compared to controls in people who stutter prior to therapy (Neumann et al., 2003). When studied at follow-up, after therapy, activity in this region (-46 -2 24; IFG) was significantly increased (Neumann et al., 2003). Functionally, the ventral premotor cortex subserves complex sequences of movements, including those involved in speech (Wise et al., 1999). In the monkey, mirror neurons responding to both production of actions and the sounds made by these actions are located in ventral premotor cortex (Kohler et al., 2002), providing further evidence that this area is critical for linking sensory and motor representations of actions.
In human development, focal unilateral lesions rarely lead to persistent speech or language abnormalities, presumably due to the capacity of the immature brain to reorganise and recover these functions (Bates et al., 1999; Hécaen, 1976). In developmental disorders with no overt neurological cause, we suspect, therefore, that the underlying abnormalities are bilateral and diffuse (Watkins et al., 2002b). Consistent with this claim, we saw bilateral structural and functional abnormalities in the people who stutter. Similarly, previous reports of brain structural differences in people who stutter have described differences in both hemispheres (Cykowski et al., 2007; Foundas et al., 2001). A previous study in developmental stuttering used diffusion imaging to identify an area of reduced white matter integrity in the left Rolandic operculum (Sommer et al., 2002). In our study, the reductions in white matter integrity in PWS seen in the left and right hemispheres were both located slightly more anterior (17mm in the y-axis) to the unilateral left-hemisphere difference previously reported. Another study reported reduction in white matter integrity in the left superior longitudinal fasciculus underlying Brodmann areas 43, 6, 40 and 22 in children who stutter (Chang et al., 2006). Area 43 is the cortical area known as the Rolandic (or central) operculum, overlying the region identified by Sommer and colleagues (2002) and seen in our study on the right to be both functional underactive and structurally abnormal (central operculum in Table 1 and Figure 1). Area 6 is premotor cortex and another area identified in our study on the left to be both functional underactive and show reduced white matter integrity (see ventral premotor cortex in Table 1 and Figure 1). Tracts in these areas, namely the superior longitudinal fasciculus and, more posteriorly located, the arcuate fasciculus, provide a substrate for communication with posterior superior temporal and inferior parietal cortex, which is likely to be a critical circuit for integrating motor plans and sensory feedback during speech production.
During acquisition of functional imaging data, the participants who stuttered produced significantly more stuttered speech than controls. However, this group difference did not interact with feedback condition; both groups produced more stuttered speech during delayed feedback than during frequency-shifted feedback but neither condition differed significantly from the normal feedback condition. In the participants who stutter, the small number of epochs of stuttered speech may have been due to fluency-enhancing effects of the scanning environment, which produces rhythmic and loud noise bursts. Also, reading of a single sentence remote from a listener might have influenced fluency in a positive way. As expected during speech production and perception of that production, both groups showed brain activity in a network of areas comprising left inferior frontal gyrus extending to the opercular surface and ventral premotor cortex, bilateral medial frontal cortex (encompassing supplementary, pre-supplementary and cingulate motor areas), sensorimotor cortex (about the level of the face representation), superior temporal gyrus and sulcus, left thalamus, and anterior cerebellum (vermal zone and both hemispheres laterally). In both groups, altered auditory feedback (delayed or frequency-shifted) resulted in increased activity in the superior temporal cortex bilaterally compared with normal feedback, consistent with previous reports (Fu et al., 2006; Hashimoto and Sakai, 2003). Delayed feedback also resulted in increased activity in the right inferior frontal gyrus compared with normal and with frequency-shifted feedback. As both groups produced significantly more stuttering during this condition relative to the frequency-shifted one, this increased activity might be related to the amount of stuttered speech produced or to compensatory activity related to the effect of delayed feedback on speech fluency. As for speech fluency, the differences in brain activity between the groups did not differ among feedback conditions. Rather, analysis of the feedback conditions separately revealed common differences during speech production between the controls and the participants who stutter. We consider these differences, therefore, to reflect a characteristic pattern of activity in the stuttering brain during speech production unrelated to the fluency attained, or the type of auditory feedback received.
The increased areas of activity in the PWS group in the right anterior insula and the cerebellum relative to the Control group are consistent with two of the three neural signatures described in the recent meta-analysis of previous functional imaging studies (Brown et al., 2005). The third neural signature, an “absence” of activity in the auditory cortices of the superior temporal lobe bilaterally, was not observed in our study. We did, however, observe a unilateral decrease in activity in left Heschl’s gyrus in people who stutter relative to controls. The reduced auditory activity reported in the meta-analysis was attributed to increased suppressive effects from repeated motor activation (efference copy; Brown et al., 2005). During vocalisation in nonhuman primates, neural activity in auditory cortex is thought to be similarly modulated by cortical vocal production centres (Eliades and Wang, 2005). In functional MRI studies using BOLD, however, it is not possible to disambiguate inhibitory and excitatory inputs as both are thought to increase the signal (Logothetis, 2002). A conservative interpretation of the decreased Heschl’s gyrus activity seen in our study, therefore, is that the input to this auditory area is reduced in people who stutter relative to controls. This might reflect reduced inputs from the motor system during speech production as activity at the level of the face representation was also reduced in people who stutter relative to controls.
In the right anterior insula, two areas showed greater activity in people who stutter relative to controls. The more dorsal peak was symmetric with a peak in the left insula. The coordinates for the more ventral peak (34 14 -14) are close to those previously reported as active in people who stutter but not in controls in the right inferior frontal cortex (frontal operculum: 36 18 -16) and negatively correlated with stuttering severity (Preibisch et al., 2003).
A striking area of overactivity was seen in the midbrain in the people who stutter relative to controls. The peaks of this activity are located bilaterally about 8mm lateral to the midline in an axial plane through the inferior colliculi. The closest structure to these peaks is the substantia nigra pars compacta, just caudal to the red nucleus and subthalamic nucleus (STN), but also very close to the putative location of the pedunclopontine nucleus (PPN). Given data averaging, normal anatomical variability and the resolution of our functional imaging data, it is not possible to be confident about which or how many of these structures contribute to the overactivity observed in our study. However, most of these nuclei are part of the basal ganglia circuitry, with reciprocal connections between PPN and cerebral cortex, STN and globus pallidus (pars interna) for example, and outputs from PPN to cortex, striatum and substania nigra, etc. The PPN is thought to be involved in the initiation and modulation of stereotyped movements, principally gait, and along with the STN is a target for therapy in the treatment of Parkinson’s disease (see Pahapill and Lozano, 2000 for review). Treatment for Parkinson’s disease with deep brain stimulation of the STN can reversibly worsen stuttering severity (Burghaus et al., 2006). Activity in the red nucleus was reported to increase in small group of subjects following stuttering therapy (Neumann et al., 2003) and, more recently, a negative correlation between stuttering severity and activity in the substantia nigra was described both before and after therapy (Giraud et al., 2007).
We have many other reasons to suspect abnormal function in cortical-striatal-thalamic loops in stuttering: fluency typically improves following the administration of dopamine antagonists e.g. haloperidol, risperidone and olanzapine (Lavid et al., 1999; Maguire et al., 2000) and worsens after treatment with a dopamine agonist e.g. levodopa (Anderson et al., 1999). Acquired stuttering is associated with lesions in the striatum or thalamus (Carluer et al., 2000) and the occurrence of basal ganglia disorders, such as Parkinson’s disease, often leads to a re-emergence of recovered developmental stuttering (Shahed and Jankovic, 2001). The overactivity of the midbrain in people who stutter seen here revives the debate about the involvement of the basal ganglia in normal and abnormal speech production (Alm, 2004; Fox et al., 1996; Klein et al., 1994; Watkins et al., 2002b; Wu et al., 1995). As mentioned above it is also consistent with previous reports of changes in basal ganglia activity associated with stuttering therapy (Giraud et al., 2007; Neumann et al., 2003). Dysfunction of the basal ganglia loops or the dopaminergic system or both may also be related to the cortical abnormalities seen in our study of developmental stuttering as it is hypothesised that the basal ganglia act in the focussed selection of movements via outputs to the premotor system and by inhibition of competing motor programs (Mink, 1996; Mink, 2003). Dysfunction in such a system for speech motor programs might lead to the production of repeated syllables and extraneous oral and facial movements, which are common features of stuttered speech.
Previous studies have suggested that the increased number of males who stutter relative to females may be due to greater recovery from developmental stuttering in the latter. In our study, both males and females were studied but due to the small number of females it was not possible to examine sex differences. However, differences in brain activity between males and females who stutter were reported specifically for correlations with stuttered speech rather than with fluent or stutter-free speech; regions in which brain activity correlates with the latter are described as “very similar for both sexes” (Ingham et al., 2004). Given that in our study, the functional differences between people who stutter and controls replicate across feedback conditions, two of which were designed to enhance fluency in people who stutter, and the low incidence of stuttered speech during scanning, we feel that any sex differences that exist would be small and reduce our sensitivity to true positive results due to additional variance. Future studies, however, will hopefully contribute further information on sex differences in both the structure and function of the brain in people who stutter.
We hypothesized on the basis of Howell’s EXPLAN theory of fluent speech control (Howell, 2004; Howell and Au-Yeung, 2002), and previous results from imaging studies (Brown et al., 2005) that both motor and language related brain areas would be abnormal in people who stutter. The central assumption of the EXPLAN theory is that language (PLAN) and motor (EX) processes are involved in speech control. On this view, the linguistic system produces serial output in correct order. When speech is progressing fluently, the motor system produces the first output and when this is complete, the next linguistic output is ready and produced. If there is an element in the sequence that is difficult for the linguistic system to generate and whose processing is delayed, speech-motor output cannot continue fluently. Speakers can deal with this by stalling, which involves either repeating speech already produced (whole words) or pausing, allowing the speaker time to complete the linguistic plan that he or she is having difficulty with. Alternatively, speakers can continue with the part of the plan available (advancing) and during the time that the available part is produced attempt to complete the remainder. If there is not sufficient time, speech will falter (speakers may prolong the first part of the word as in “ssssister”, repeat it as in “suh-suh-sister” or put in a pause as in “s-ister”). Dysfluencies are reflected in either motor activity (stalling repeats motor programs already available that do not have to be planned linguistically) or linguistic activity (advancing the speech interferes with language processing). Our findings of abnormalities in both motor and language areas in PWS are in general agreement with EXPLAN. The white matter abnormality underlying premotor cortex likely disrupts tracts in this area, which via connections with posterior superior temporal and inferior parietal cortex provide a substrate for the integration of articulatory planning and sensory feedback, and via connections with primary motor cortex, a substrate for execution of articulatory movements. Future work should classify fluent, stalled and advanced sentences to examine whether abnormalities in the motor and language systems can be separately identified.
In conclusion, we have found functional abnormalities in many cortical and subcortical motor areas related to speech production and the selection and initiation of motor sequences more generally. Structural white matter abnormalities underlie the functional ones in ventral premotor cortex, an area critical for integration of sensory and motor information. We suspect that the structural abnormalities cause the functional ones but we cannot rule out the possibility that a history of stuttering during development might have resulted in abnormal development of these white matter tracts. Longitudinal studies starting early in development should help us to address these alternative hypotheses.
Acknowledgements
We wish to thank Tim Behrens, Heidi Johansen-Berg and Clare Mackay for their assistance with the diffusion imaging data acquisition and analysis and for useful discussions; Ned Jenkinson for discussions on the pedunculopontine nucleus; and Joe Devlin for his helpful comments on the manuscript. This study was funded by an MRC New Investigator Award to KW and the Wellcome Trust (PH). We thank all the participants in this study for their continued contribution to our research.
Abbreviations
- BOLD
blood oxygenation-level dependant
- FA
fractional anisotropy
- FSL
FMRIB software library
- IFG
inferior frontal gyrus
- PPN
pedunculopontine nucleus
- PWS
people who stutter
- STN
subthalamic nucleus
- TBSS
tract-based spatial statistics
References
- Alm PA. Stuttering and the basal ganglia circuits: a critical review of possible relations. J Commun Disord. 2004;37:325–69. doi: 10.1016/j.jcomdis.2004.03.001. [DOI] [PubMed] [Google Scholar]
- Anderson JM, Hughes JD, Gonzalez Rothi LJ, Crucian GP, Heilman KM. Developmental stuttering and Parkinson’s disease: the effects of levodopa treatment. Journal of Neurology, Neurosurgery and Psychiatry. 1999;66:776–778. doi: 10.1136/jnnp.66.6.776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andrews G, Craig A, Feyer AM, Hoddinott S, Howie P, Neilson M. Stuttering: a review of research findings and theories circa 1982. J Speech Hear Disord. 1983;48:226–46. doi: 10.1044/jshd.4803.226. [DOI] [PubMed] [Google Scholar]
- Andrews G, Harris M. The Syndrome of Stuttering. London, UK: William Heinemann Medical Books; 1964. [Google Scholar]
- Barbas H, Pandya DN. Architecture and frontal cortical connections of the premotor cortex (area 6) in the rhesus monkey. J Comp Neurol. 1987;256:211–28. doi: 10.1002/cne.902560203. [DOI] [PubMed] [Google Scholar]
- Bates E, Vicari S, Trauner D. Neural mediation of language development: perspectives from lesion studies of infants and children. In: Tager-Flusberg H, editor. Neurodevelopmental Disorders. Cambridge, MA: MIT Press; 1999. pp. 533–581. [Google Scholar]
- Belin P, Zatorre RJ, Hoge R, Evans AC, Pike B. Event-related fMRI of the auditory cortex. NeuroImage. 1999;10:417–429. doi: 10.1006/nimg.1999.0480. [DOI] [PubMed] [Google Scholar]
- Bloodstein O. Handbook on stuttering. San Diego: Singular; 1995. [Google Scholar]
- Braun AR, Varga M, Stager S, Schulz G, Selbie S, Maisog JM, et al. Altered patterns of cerebral activity during speech and language production in developmental stuttering. An H2(15)O positron emission tomography study. Brain. 1997;120(Pt 5):761–84. doi: 10.1093/brain/120.5.761. [DOI] [PubMed] [Google Scholar]
- Brown S, Ingham RJ, Ingham JC, Laird AR, Fox PT. Stuttered and fluent speech production: An ALE meta-analysis of functional neuroimaging studies. Human Brain Mapping. 2005;25:105–117. doi: 10.1002/hbm.20140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burghaus L, Hilker R, Thiel A, Galldiks N, Lehnhardt FG, Zaro-Weber O, et al. Deep brain stimulation of the subthalamic nucleus reversibly deteriorates stuttering in advanced Parkinson’s disease. J Neural Transm. 2006;113:625–31. doi: 10.1007/s00702-005-0341-1. [DOI] [PubMed] [Google Scholar]
- Carluer L, Marie RM, Lambert J, Defer GL, Coskun O, Rossa Y. Acquired and persistent stuttering as the main symptom of striatal infarction. Mov Disord. 2000;15:343–6. doi: 10.1002/1531-8257(200003)15:2<343::aid-mds1026>3.0.co;2-i. [DOI] [PubMed] [Google Scholar]
- Chang S, Erikcson KI, Ambrose NG, Hasegawa-Johnson M, Ludlow CL. Deficient white matter development in left hemisphere speech-language regions in chilren who stutter; 2006; Atlanta, GA. Society for Neuroscience; 2006 Neuroscience Meeting Planner. Online. [Google Scholar]
- Cykowski MD, Kochunov PV, Ingham RJ, Ingham JC, Mangin JF, Riviere D, et al. Perisylvian Sulcal Morphology and Cerebral Asymmetry Patterns in Adults Who Stutter. Cereb Cortex. 2007 doi: 10.1093/cercor/bhm093. [DOI] [PubMed] [Google Scholar]
- De Nil LF, Kroll RM, Kapur S, Houle S. A positron emission tomography study of silent and oral single word reading in stuttering and nonstuttering adults. J Speech Lang Hear Res. 2000;43:1038–53. doi: 10.1044/jslhr.4304.1038. [DOI] [PubMed] [Google Scholar]
- De Nil LF, Kroll RM, Lafaille SJ, Houle S. A positron emission tomography study of short- and long-term treatment effects on functional brain activation in adults who stutter. J Fluency Disord. 2003;28:357–79. doi: 10.1016/j.jfludis.2003.07.002. quiz 379-80. [DOI] [PubMed] [Google Scholar]
- Eliades SJ, Wang X. Dynamics of auditory-vocal interaction in monkey auditory cortex. Cereb Cortex. 2005;15:1510–23. doi: 10.1093/cercor/bhi030. [DOI] [PubMed] [Google Scholar]
- Foundas AL, Bollich AM, Corey DM, Hurley M, Heilman KM. Anomalous anatomy of speech-language areas in adults with persistent developmental stuttering. Neurology. 2001;57:207–15. doi: 10.1212/wnl.57.2.207. [DOI] [PubMed] [Google Scholar]
- Foundas AL, Bollich AM, Feldman J, Corey DM, Hurley M, Lemen LC, et al. Aberrant auditory processing and atypical planum temporale in developmental stuttering. Neurology. 2004;63:1640–6. doi: 10.1212/01.wnl.0000142993.33158.2a. [DOI] [PubMed] [Google Scholar]
- Foundas AL, Corey DM, Angeles V, Bollich AM, Crabtree-Hartman E, Heilman KM. Atypical cerebral laterality in adults with persistent developmental stuttering. Neurology. 2003;61:1378–85. doi: 10.1212/01.wnl.0000094320.44334.86. [DOI] [PubMed] [Google Scholar]
- Fox PT, Huang A, Parsons LM, Xiong JH, Zamarippa F, Rainey L, et al. Location-probability profiles for the mouth region of human primary motor-sensory cortex: model and validation. Neuroimage. 2001;13:196–209. doi: 10.1006/nimg.2000.0659. [DOI] [PubMed] [Google Scholar]
- Fox PT, Ingham RJ, Ingham JC, Hirsch TB, Downs JH, Martin C, et al. A PET study of the neural systems of stuttering. Nature. 1996;382:158–61. doi: 10.1038/382158a0. [DOI] [PubMed] [Google Scholar]
- Fox PT, Ingham RJ, Ingham JC, Zamarripa F, Xiong J-H, Lancaster JL. Brain correlates of stuttering and syllable production. A PET performance-correlation analysis. Brain. 2000;123:1985–2004. doi: 10.1093/brain/123.10.1985. [DOI] [PubMed] [Google Scholar]
- Fu CH, Vythelingum GN, Brammer MJ, Williams SC, Amaro E, Jr., Andrew CM, et al. An fMRI study of verbal self-monitoring: neural correlates of auditory verbal feedback. Cereb Cortex. 2006;16:969–77. doi: 10.1093/cercor/bhj039. [DOI] [PubMed] [Google Scholar]
- Giraud AL, Neumann K, Bachoud-Levi AC, von Gudenberg AW, Euler HA, Lanfermann H, et al. Severity of dysfluency correlates with basal ganglia activity in persistent developmental stuttering. Brain Lang. 2007 doi: 10.1016/j.bandl.2007.04.005. [DOI] [PubMed] [Google Scholar]
- Glover GH. Deconvolution of impulse response in event-related BOLD fMRI. Neuroimage. 1999;9:416–29. doi: 10.1006/nimg.1998.0419. [DOI] [PubMed] [Google Scholar]
- Hall DA, Haggard MP, Akeroyd MA, Palmer AR, Summerfield AQ, Elliott MR, et al. “Sparse” temporal sampling in auditory fMRI. Human Brain Mapping. 1999;7:213–223. doi: 10.1002/(SICI)1097-0193(1999)7:3<213::AID-HBM5>3.0.CO;2-N. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hashimoto Y, Sakai KL. Brain activations during conscious self-monitoring of speech production with delayed auditory feedback: An fMRI study. Human Brain Mapping. 2003;20:22–28. doi: 10.1002/hbm.10119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hécaen H. Acquired aphasia in children and the ontogenesis of hemispheric functional specialization. Brain and Language. 1976;3:114–134. doi: 10.1016/0093-934x(76)90009-2. [DOI] [PubMed] [Google Scholar]
- Howell P. Assessment of some contemporary theories of stuttering that apply to spontaneous speech. Contemporary Issues in Communicative Sciences and Disorders. 2004;39:122–139. [PMC free article] [PubMed] [Google Scholar]
- Howell P, Au-Yeung J. The EXPLAN theory of fluency control and the diagnosis of stuttering. In: Fava E, editor. Pathology and therapy of speech disorders. Amsterdam: John Benjamins; 2002. pp. 75–94. [Google Scholar]
- IEEE SoSM IEEE Recommended Practices for Speech Quality Measurements. IEEE Trans. Audio Electroacoust. 1969;AU-17:227–246. [Google Scholar]
- Ingham RJ. Brain imaging studies of developmental stuttering. J Commun Disord. 2001;34:493–516. doi: 10.1016/s0021-9924(01)00061-2. [DOI] [PubMed] [Google Scholar]
- Ingham RJ, Fox PT, Ingham JC, Xiong J, Zamarripa F, Hardies LJ, et al. Brain correlates of stuttering and syllable production: gender comparison and replication. J Speech Lang Hear Res. 2004;47:321–41. doi: 10.1044/1092-4388(2004/026). [DOI] [PubMed] [Google Scholar]
- Jayaram M. Distribution of stuttering in sentences: relationship to sentence length and clause position. J Speech Hear Res. 1984;27:338–41. doi: 10.1044/jshr.2703.338. [DOI] [PubMed] [Google Scholar]
- Jenkinson M. Fast, automated, N-dimensional phase-unwrapping algorithm. Magn Reson Med. 2003;49:193–7. doi: 10.1002/mrm.10354. [DOI] [PubMed] [Google Scholar]
- Kalinowski J, Saltuklaroglu T. Choral speech: the amelioration of stuttering via imitation and the mirror neuronal system. Neurosci Biobehav Rev. 2003;27:339–47. doi: 10.1016/s0149-7634(03)00063-0. [DOI] [PubMed] [Google Scholar]
- Karniol R. Stuttering, language, and cognition: a review and a model of stuttering as suprasegmental sentence plan alignment (SPA) Psychol Bull. 1995;117:104–24. doi: 10.1037/0033-2909.117.1.104. [DOI] [PubMed] [Google Scholar]
- Klein D, Zatorre RJ, Milner B, Meyer E, Evans AC. Left putaminal activation when speaking a second language: evidence from PET. NeuroReport. 1994;5:2295–2297. doi: 10.1097/00001756-199411000-00022. [DOI] [PubMed] [Google Scholar]
- Kohler E, Keysers C, Umilta MA, Fogassi L, Gallese V, Rizzolatti G. Hearing sounds, understanding actions: action representation in mirror neurons. Science. 2002;297:846–848. doi: 10.1126/science.1070311. [DOI] [PubMed] [Google Scholar]
- Lavid N, Franklin DL, Maguire GA. Management of child and adolescent stuttering with olanzapine: three case reports. Ann Clin Psychiatry. 1999;11:233–6. doi: 10.1023/a:1022365513865. [DOI] [PubMed] [Google Scholar]
- Logothetis NK. The neural basis of the blood-oxygen-level-dependent functional magnetic resonance imaging signal. Philos Trans R Soc Lond B Biol Sci. 2002;357:1003–37. doi: 10.1098/rstb.2002.1114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ludlow CL, Loucks T. Stuttering: a dynamic motor control disorder. Journal of Fluency Disorders. 2003;28:273–295. doi: 10.1016/j.jfludis.2003.07.001. [DOI] [PubMed] [Google Scholar]
- Maguire GA, Riley GD, Franklin DL, Gottschalk LA. Risperidone for the treatment of stuttering. J Clin Psychopharmacol. 2000;20:479–82. doi: 10.1097/00004714-200008000-00013. [DOI] [PubMed] [Google Scholar]
- Melnick KS, Conture EG. Relationship of length and grammatical complexity to the systematic and nonsystematic speech errors and stuttering of children who stutter. Journal of Fluency Disorders. 2000;25:21–45. [Google Scholar]
- Mesulam MM, Mufson EJ. Insula of the old world monkey. III: Efferent cortical output and comments on function. J Comp Neurol. 1982;212:38–52. doi: 10.1002/cne.902120104. [DOI] [PubMed] [Google Scholar]
- Mink JW. The basal ganglia: focused selection and inhibition of competing motor programs. Prog Neurobiol. 1996;50:381–425. doi: 10.1016/s0301-0082(96)00042-1. [DOI] [PubMed] [Google Scholar]
- Mink JW. The Basal Ganglia and involuntary movements: impaired inhibition of competing motor patterns. Arch Neurol. 2003;60:1365–8. doi: 10.1001/archneur.60.10.1365. [DOI] [PubMed] [Google Scholar]
- Neumann K, Euler HA, von Gudenberg AW, Giraud AL, Lanfermann H, Gall V, et al. The nature and treatment of stuttering as revealed by fMRI A within- and between-group comparison. J Fluency Disord. 2003;28:381–409. doi: 10.1016/j.jfludis.2003.07.003. quiz 409-410. [DOI] [PubMed] [Google Scholar]
- Neumann K, Preibisch C, Euler HA, von Gudenberg AW, Lanfermann H, Gall V, et al. Cortical plasticity associated with stuttering therapy. J Fluency Disord. 2005;30:23–39. doi: 10.1016/j.jfludis.2004.12.002. [DOI] [PubMed] [Google Scholar]
- Pahapill PA, Lozano AM. The pedunculopontine nucleus and Parkinson’s disease. Brain. 2000;123(Pt 9):1767–83. doi: 10.1093/brain/123.9.1767. [DOI] [PubMed] [Google Scholar]
- Petrides M, Pandya DN. Association pathways of the prefrontal cortex and functional observations. In: Stuss DT, Knight RT, editors. Principles of Frontal Lobe Function. New York: Oxford University Press; 2002. pp. 31–50. [Google Scholar]
- Preibisch C, Neumann K, Raab P, Euler HA, von Gudenberg AW, Lanfermann H, et al. Evidence for compensation for stuttering by the right frontal operculum. Neuroimage. 2003;20:1356–64. doi: 10.1016/S1053-8119(03)00376-8. [DOI] [PubMed] [Google Scholar]
- Riley GD. SSI-3 Stuttering Severity Instrument for Children and Adults. Austin, TX: Pro-Ed; 1994. [DOI] [PubMed] [Google Scholar]
- Shahed J, Jankovic J. Re-emergence of childhood stuttering in Parkinson’s disease: a hypothesis. Mov Disord. 2001;16:114–8. doi: 10.1002/1531-8257(200101)16:1<114::aid-mds1004>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- Smith SM, Jenkinson M, Johansen-Berg H, Rueckert D, Nichols TE, Mackay CE, et al. Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Neuroimage. 2006;31:1487–505. doi: 10.1016/j.neuroimage.2006.02.024. [DOI] [PubMed] [Google Scholar]
- Sommer M, Koch MA, Paulus W, Weiller C, Buchel C. Disconnection of speech-relevant brain areas in persistent developmental stuttering. Lancet. 2002;360:380–3. doi: 10.1016/S0140-6736(02)09610-1. [DOI] [PubMed] [Google Scholar]
- Van Borsel J, Achten E, Santens P, Lahorte P, Voet T. fMRI of developmental stuttering: a pilot study. Brain Lang. 2003;85:369–76. doi: 10.1016/s0093-934x(02)00588-6. [DOI] [PubMed] [Google Scholar]
- Watkins KE, Dronkers NF, Vargha-Khadem F. Behavioural analysis of an inherited speech and language disorder: comparison with acquired aphasia. Brain. 2002a;125:452–64. doi: 10.1093/brain/awf058. [DOI] [PubMed] [Google Scholar]
- Watkins KE, Vargha-Khadem F, Ashburner J, Passingham RE, Connelly A, Friston KJ, et al. MRI analysis of an inherited speech and language disorder: structural brain abnormalities. Brain. 2002b;125:465–78. doi: 10.1093/brain/awf057. [DOI] [PubMed] [Google Scholar]
- Wise RJ, Greene J, Buchel C, Scott SK. Brain regions involved in articulation. The Lancet. 1999;353:1057–1061. doi: 10.1016/s0140-6736(98)07491-1. [DOI] [PubMed] [Google Scholar]
- Woolrich MW, Behrens TE, Beckmann CF, Jenkinson M, Smith SM. Multilevel linear modelling for FMRI group analysis using Bayesian inference. Neuroimage. 2004;21:1732–47. doi: 10.1016/j.neuroimage.2003.12.023. [DOI] [PubMed] [Google Scholar]
- Wu JC, Maguire G, Riley G, Fallon J, LaCasse L, Chin S, et al. A positron emission tomography [18F]deoxyglucose study of developmental stuttering. Neuroreport. 1995;6:501–5. doi: 10.1097/00001756-199502000-00024. [DOI] [PubMed] [Google Scholar]
- Wu JC, Maguire G, Riley G, Lee A, Keator D, Tang C, et al. Increased dopamine activity associated with stuttering. Neuroreport. 1997;8:767–70. doi: 10.1097/00001756-199702100-00037. [DOI] [PubMed] [Google Scholar]