

Abstract
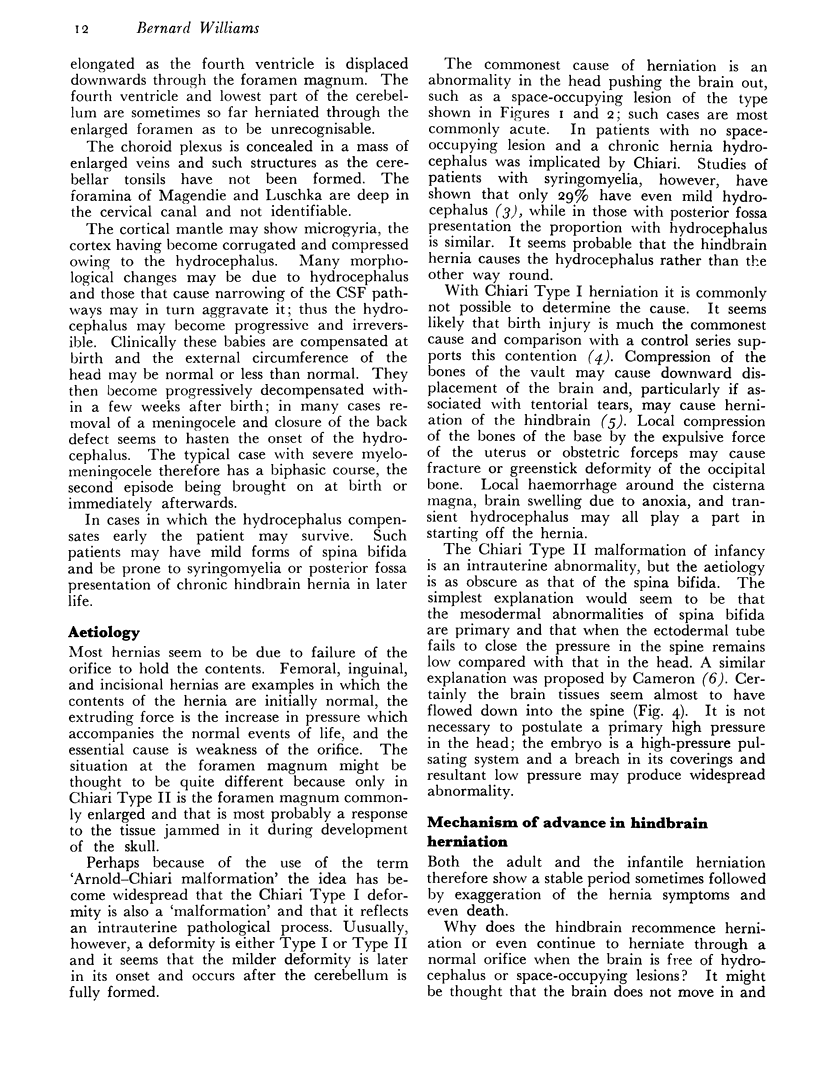
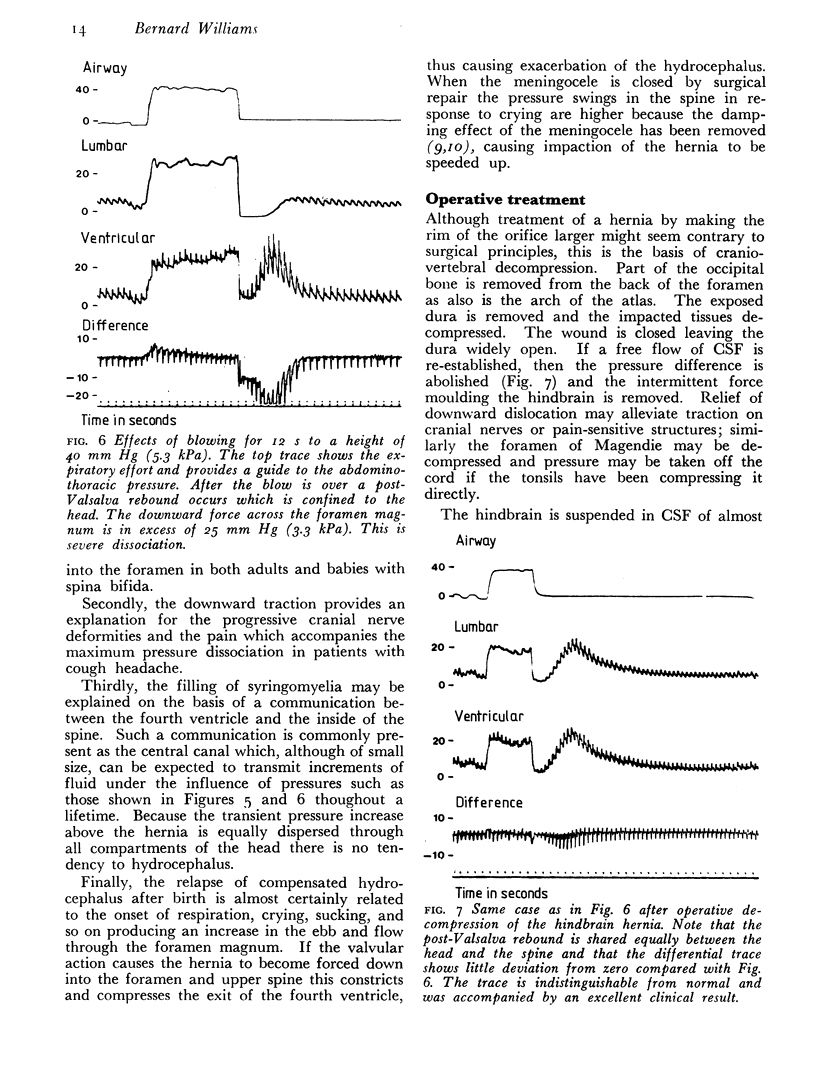
Herniation of the hindbrain occurs when the lowest parts of the cerebellum and sometimes part of the medulla are moved downwards through the foramen magnum, a pressure difference acting across the foramen magnum moulding the tissues into a plug. It is suggested that the clinical course in both adults and babies with spina bifida may be explained by the hindbrain hernia acting as a valve.
The term 'Chiari Type I deformity' is commonly used for an abnormality in which the tonsils and lowermost parts of the cerebellar hemispheres are prolapsed through a normal foramen magnum. Acute herniation may occur as a result of space-occupying lesions. Chronic herniation may be morphologically identical although it tends to be more severe. Sometimes it will produce few symptoms which often may be delayed so that the original causative lesion may not be apparent. Causes include bone softening, tumour, or previous meningitis. Birth injury is probably the commonest cause of the deformity, which presents clinically in adults.
In infants with severe forms of spina bifida a hindbrain herniation is present. This abnormality may be called 'Chiari Type II deformity' or Arnold—Chiari deformity and is an intra-uterine abnormality in which the fourth ventricle and medulla are grotesquely herniated before they are properly developed and the foramen magnum is enlarged.
The commonest clinical presentation of Chiari Type I deformity is syringomyelia, which is usually not diagnosed until adult life. Other presentations include syringobulbia, headache, oscillopsia, attacks of giddiness, lower cranial nerve palsies, and ataxia. Particularly characteristic are cough headache and cough syncope. Syringomyelia and syringobulbia in particular may be irreversible by the time they are diagnosed. Nevertheless, surgical decompression may be successful in relieving symptoms of headache, cough syncope, and long-tract compression; most cases of syringomyelia show some improvement and in others progression of the disease is arrested. Operative techniques for hindbrain herniation are discussed.
Chiari Type II deformity is probably responsible for the progression of hydrocephalus after birth in the majority of babies with spina bifida. Measurement of pressure in the cerebrospinal fluid above and below the foramen magnum shows that intermittent pressure difference is commonly present at times of neurological deterioration. Surgical decompression of the hernia in adults allows correction of the valvular effect, which may be monitored by pressure measurements. In babies the associated hydrocephalus is usually so gross that it requires separate treatment, but pressure monitoring may be of value in assessing the state of the disease.
Keywords: ARNOLD—CHIARI DEFORMITY, CEREBELLAR DISEASES, CEREBROSPINAL FLUID, INTRACRANIAL PRESSURE, SPINA BIFIDA, SYRINGOMYELIA
Full text
PDF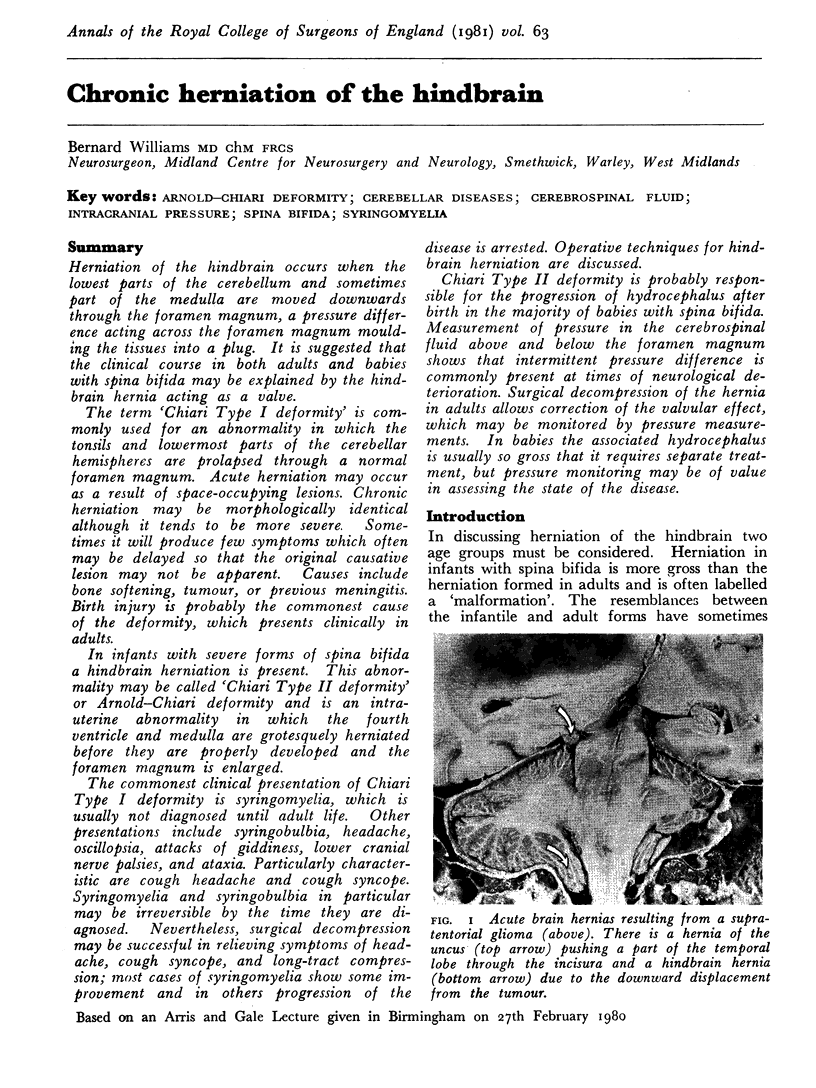




Images in this article




Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ashton F., Geddes R., Fejfar J. Woven silicone rubber as a venous prosthesis. Br Med J. 1969 Aug 16;3(5667):409–410. doi: 10.1136/bmj.3.5667.409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GARDNER W. J. HYDRODYNAMIC MECHANISM OF SYRINGOMYELIA: ITS RELATIONSHIP TO MYELOCELE. J Neurol Neurosurg Psychiatry. 1965 Jun;28:247–259. doi: 10.1136/jnnp.28.3.247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lapras C., Poirier N., Deruty R., Bret P., Jyeux O. Le cathétérisme de l'aqueduc de Sylvius Sa place actuelle dans le traitement chirurgical des sténoses de l'aqueduc de Sylvius, des tumeurs de la F.C.P. et de la syringomyélie. Neurochirurgie. 1975 Mar-Apr;21(2):101–109. [PubMed] [Google Scholar]
- Mohr P. D., Strang F. A., Sambrook M. A., Boddie H. G. The clinical and surgical feature in 40 patients with primary cerebellar ectopia (adult Chiari malformation). Q J Med. 1977 Jan;46(181):85–96. [PubMed] [Google Scholar]
- West R. J., Williams B. Radiographic studies of the ventricles in syringomyelia. Neuroradiology. 1980 Aug;20(1):5–16. doi: 10.1007/BF00346855. [DOI] [PubMed] [Google Scholar]
- Williams B. A demonstration analogue for ventricular and intraspinal dynamics (DAVID). J Neurol Sci. 1974 Nov;23(3):445–461. doi: 10.1016/0022-510x(74)90161-0. [DOI] [PubMed] [Google Scholar]
- Williams B. Cerebrospinal fluid pressure changes in response to coughing. Brain. 1976 Jun;99(2):331–346. doi: 10.1093/brain/99.2.331. [DOI] [PubMed] [Google Scholar]
- Williams B. Difficult labour as a cause of communicating syringomyelia. Lancet. 1977 Jul 9;2(8028):51–53. doi: 10.1016/s0140-6736(77)90060-5. [DOI] [PubMed] [Google Scholar]