

Abstract
Signs of early myocardial ischaemia are the most powerful available predictors of myocardial infarction and CHD death. The main primary risk factors are of undiminished importance in such persons, but screening for myocardial ischaemia is not recommended without evidence that intervention at this late stage is effective.
Estimates are presented of the relative importance to individuals of the main primary risk factors. Their importance as population risk factors is different, depending on the product of attributable risk and prevalence: a high risk with low prevalence, as from severe hypercholesterolaemia, is of small importance compared with that arising from the numerous individuals with smaller elevations. Most cases of CHD arise from the common and therefore inconspicuous combination of slight increases in two or three factors in the same individual. Selective and opportunistic risk factor screening is recommended, not a general service.
An extension of clinical responsibility in the direction of preventive responsibility is generally accepted as proper, even though it is slow in being applied. When someone with symptomless hypertension is given hypotensive drugs with the object of reducing the risk of stroke, that is preventive medicine. The subject having made no complaint is not strictly a patient: but the clinician accepts a responsibility for him because of the high risk that he will become a patient if nothing is done. This is an analogy for our concern with identifying subjects with a high coronary risk, and the attempt in such persons to prevent the onset of major ischaemia.
Full text
PDF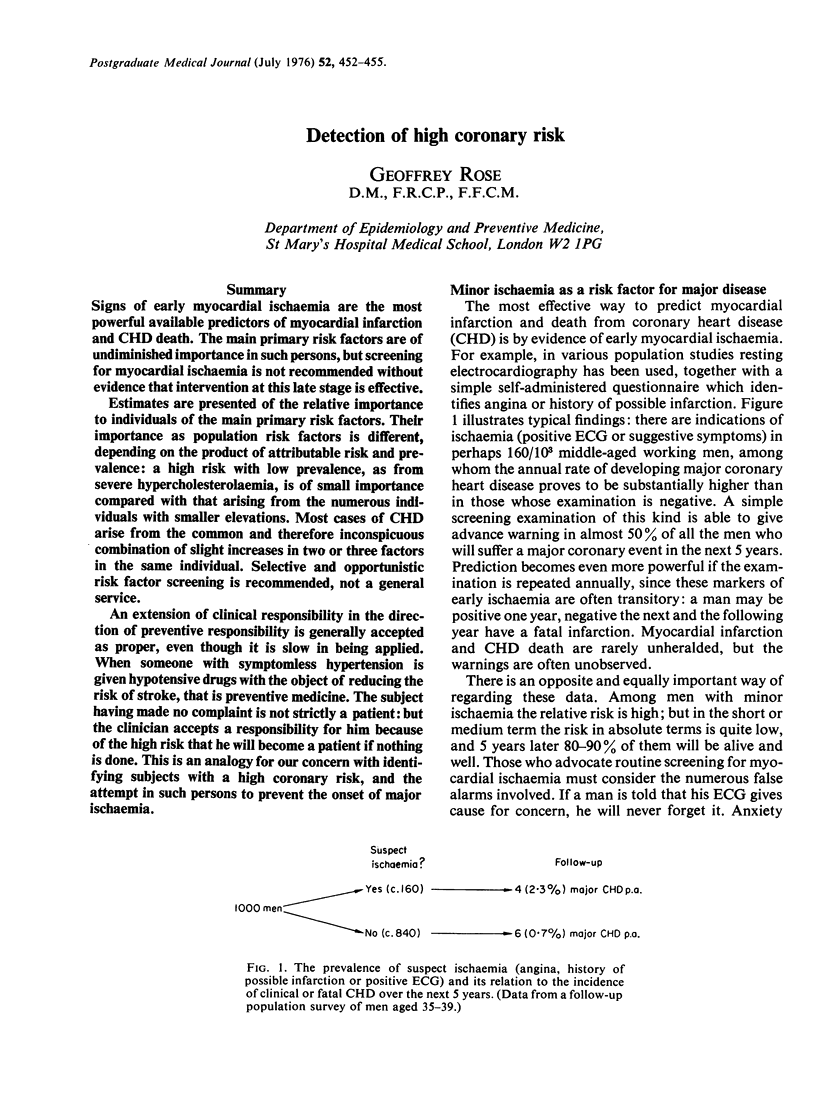

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Blackburn H. Concepts and controversies about the prevention of coronary heart disease. Postgrad Med J. 1976 Jul;52(609):417–423. doi: 10.1136/pgmj.52.609.417. [DOI] [PMC free article] [PubMed] [Google Scholar]