

Abstract
Background
The purpose of this study was to determine the associations between depression and the likelihood of enrollment in a health plan–sponsored physical activity program and pattern of program participation over 2 years; a secondary aim was to examine the association between participation dose and depression risk. There are no published studies on how depression influences participation in health plan–sponsored physical activity programs and how participation affects depression risk in older adults in nonresearch settings.
Methods
This study used administrative data from a Medicare Advantage plan. Participants (n=4766) were enrolled in the plan for at least 1 year prior to participating in the plan-sponsored health club benefit (Silver Sneakers®). Controls were age- and gender-matched to participants (n=9035). Members were identified as having depression based on ICD-9-CM codes. Multivariate regression and generalized estimating equations models were used. Data were collected between 1998 and 2003 and analyzed in 2008.
Results
Members who had a history of depression were as likely to participate in Silver Sneakers as nondepressed members (OR: 1.03; 95%CI=0.89, 1.20; p=0.67). The risk of lapse in Silver Sneakers attendance was 28%–55% (p<0.05) higher for depressed participants during months 15–24. For nondepressed Silver Sneakers participants, attendance of at least 2 visits/week during Year 1 was significantly associated with lower risk of depression in Year 2 (OR=0.54; 95%CI= 0.37, 0.79; p=0.002); a similar but statistically nonsignificant association was observed for previously depressed participants (OR=0.51; 95%CI=0.26, 1.02; p=0.06).
Conclusions
While depressed older adults are as likely to enroll in a health plan–sponsored physical activity as nondepressed members, they were at higher risk of attendance lapses. Greater participation in the physical activity program was associated with lower depression risk.
Background
Despite the many health benefits of physical activity,1–4 approximately 25% of U.S. adults aged 65 and older engage in less than 10 minutes of moderate- or vigorous-intensity activities a week.5 A number of studies have identified multiple barriers to physical activity adoption and maintenance including perceived poor health, lack of time, lack of social support, limited access to enjoyable physical activity programs, and negative affect or depression.6–8 Depression, which is the focus of this paper, affects between 5% and 10% of older adults seen in primary care and is associated with decreased adherence to self-management behaviors such as exercise, diet, and medication adherence.9, 10
The relationship between physical activity and depression is especially complex in older adults since the influence may be in either direction. Depression can decrease motivation to engage in physical activity, but low physical activity can also lead to the development of chronic conditions that are associated with depression. Although the mechanisms and causal direction are unknown, numerous pathways have been hypothesized, such as increased biosynthesis of monoamines, catecholamines, and endorphins and improved brain blood flow and plasticity.11 Psychosocial mechanisms include enhanced self-efficacy and self-esteem or that physical activity may serve as a buffer against stressful events, and serves to reduce social isolation.
Multiple longitudinal studies of nondepressed adult and older adult community samples that adjusted for pre-existing physical and health problems reported an inverse relationship between physical activity and depressive symptoms.12–20 These findings suggest that the risk of depression may be modifiable with changes in exercise habits. Brown et al.12 showed not only a dose–response relationship between physical activity and depressive symptoms in middle age women, but also that moderate-intensity physical activity below the currently recommended guidelines (60–150 minutes per week) could significantly lower the risk of depressive symptoms by 20%. Experimental studies of physical activity with relatively healthy older adults also showed improvements in emotional well-being.21–23 Evidence from controlled studies on carefully selected depressed adults and older adults suggest that exercise training improves depressive symptoms in the short term.23–29
Prompted by the promise of health benefits with physical activity, many organizations, including health plans, have in recent years expanded their prevention benefits to include formal physical activity programs. Because such benefits can be costly to finance, decision makers need information on who actually use these benefits, barriers associated with use, and what pattern of use results in improved outcomes at the population level. There are no published studies on how depression influences participation in health plan–sponsored physical activity programs and how participation affects depression risk in older adults in nonresearch settings.
Therefore, the research questions were:
Are depressed older adult Medicare Advantage plan members compared to nondepressed members less likely to enroll in a voluntary health plan–sponsored physical activity program (Silver Sneakers®)?
Are the patterns of Silver Sneakers program participation different between depressed and nondepressed Silver Sneakers participants over a 2-year period?
What is the association between Silver Sneakers participation in Year 1 and depression risk in Year 2 for members who were either depressed or not depressed before enrolling in the Silver Sneakers program?
The hypotheses were that (1) members with a history of depression are less likely to enroll in Silver Sneakers compared to members with no history of depression; (2) depressed Silver Sneakers participants are more likely to have participation lapses, defined as no visits made to a Silver Sneakers fitness facility in any given month; and (3) higher attendance at the Silver Sneakers program is associated with a lower risk of recurrent or incident depression among previously depressed and nondepressed members, respectively.
Methods
Study Design
A case–control design was used to answer the first research question with depression as the exposure variable and participation in the Silver Sneakers program as the outcome. A retrospective cohort design was used to answer the second and third questions with pre-existing depression as the exposure and Silver Sneakers participation as the outcome, and Silver Sneakers participation as the exposure and subsequent depression as the outcome, respectively. Automated administrative and claims data were used from Group Health Cooperative (GHC), a consumer-governed, mixed-model HMO with over 500,000 members. GHC members reflect the demographic composition of Seattle and western Washington, which is predominantly Caucasian (88%) with 6% Asian Americans, 4% African Americans, and 3% Latino and other minorities.10 The IRBs at the University of Washington and GHC approved the study protocol.
Study Subjects
A total of 8269 members aged ≥65 who enrolled in the GHC Medicare Advantage plan and were continuously enrolled at GHC for at least 1 year prior to the date of joining the program, and participated in Silver Sneakers between January 1, 1998 and December 31, 2003 were studied. Up to three age- and gender-matched GHC Medicare Advantage enrollees (n=21,377) who never used the program served as controls for each Silver Sneakers participant. Participants and their matched controls were each assigned an index date representing the month that the participant first visited Silver Sneakers to create similar pre-exposure and follow-up time periods.
Members who had long-term care costs at baseline that would have made it impossible for them to participate in Silver Sneakers (n=1288), had less than 2 years of continuous enrollment after their index date (n=11,033), or were an unmatched Silver Sneakers participant or control (n=3524) were excluded, leaving 4766 Silver Sneakers participants and 9035 matched controls for analysis (Figure 1).
Figure 1.
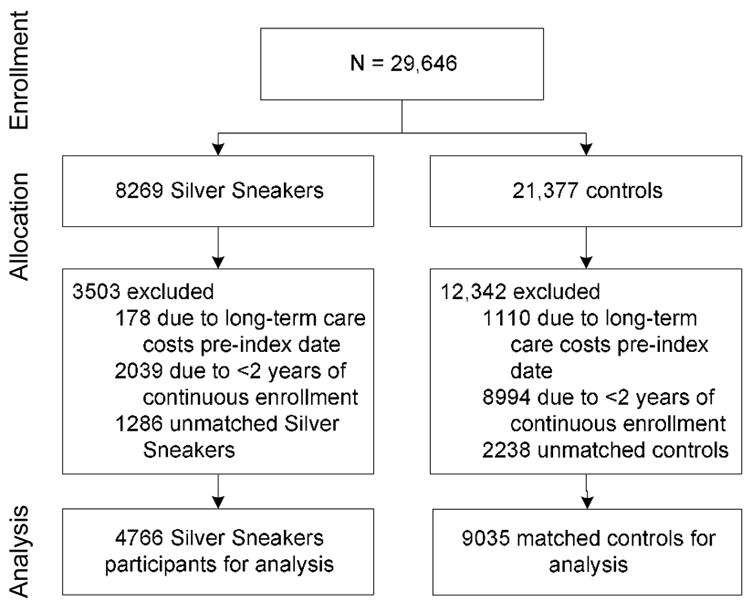
Participant flow diagram
Measures
Depression
Members were identified as depressed based on diagnostic codes obtained from outpatient visit problem lists for major depression, dysthymic disorder, or depression not otherwise specified (ICD-9-CM: 296.2, 296.3, 300.4, 311) in the 12 months preceding the index date of Silver Sneakers enrollment and over the 2 years after the index enrollment date.
Silver Sneakers participation
The Silver Sneakers program provided older adult GHC Medicare Advantage members access to local fitness facilities in an unstructured format. Participants had access to conditioning classes designed for older adults, exercise equipment, pool, sauna, and other amenities that varied across facilities; visits to these facilities do not necessarily equate with actual exercise. A subcontractor administered the program and interfaced with the fitness facilities. Members learned about the Silver Sneakers program from targeted mailings, a benefits website, or through their health providers during routine preventive visits. The total number of fitness facility visits per month was provided to GHC by the Silver Sneakers program subcontractor. Some Silver Sneakers participants registered >30 visits/month, which could be due to multiple visits in one day or errors in data collection; the maximum number of visits in any particular month was capped at 30 visits. Since Silver Sneakers is a voluntary program with no attendance requirements relevant to calculation of adherence, the term, “attendance lapse” defined a lapse as no visit to a Silver Sneakers fitness facility in a given month was used for Aim Two.30,31 For the third aim, Silver Sneakers participants were classified according to two schemes, by the public health frequency dose (PHFD) recommendation of 5 visits per week32, 33 and by total visit quartiles.
Covariates
RxRisk, a validated measure of chronic disease burden and comorbidity 34, 35 was included as a covariate since it could be associated with depression and participation in physical activity. RxRisk was calculated for each member based on age, gender, and pharmacy utilization data for a 6-month period prior to the index date.36 Since individuals who are prevention focused might be more likely enroll in Silver Sneakers, a preventive services index was created to adjust for this potential selection bias for the first aim. The index was derived from the sum of the number of times a participant received colon cancer screening (fecal occult blood test or flexible sigmoidoscopy); a screening mammogram; prostate cancer screening; an influenza vaccine; or a pneumococcal vaccine during the 2 years preceding the index date.37 Also, since depressed individuals are likely to use more health services38 and therefore avail themselves to more opportunities for physical activity advice from health providers, the total number of primary care visits in the year prior to the index date, derived from claims data, was included as a covariate for the first aim. Distance, previously shown to be related to Silver Sneakers enrollment and participation, was included as a covariate for the first and second aims.39 The home addresses and fitness facilities were geocoded (MapMarker v 9.3) and the direct distance in km between the two points was calculated.39
Data Analysis
Chi square and unpaired t-tests were used to compare baseline sample characteristics. Logistic regression models were used to predict initial enrollment in Silver Sneakers according to baseline depression status. Covariates included age, gender, RxRisk, preventive services index, distance, and number of primary care visits. To capture the “recycling” pattern that is characteristic of exercise behavior and to account for the correlated outcome, generalized estimating equations with an exchangeable correlation structure were used to compare the repeated binary outcome of attendance lapse every month for 2 years between depressed and nondepressed Silver Sneakers participants. Time to the first Silver Sneakers attendance lapse (first month in which no visits were made to the fitness facility) was analyzed by means of a log-rank test. Cox proportional hazards regression models were also used to account for baseline covariates described above. Logistic regression models, adjusted for age, gender, and RxRisk, were used to determine risk of depression in Year 2 following 1 year of Silver Sneakers participation based on the PHFD threshold and Silver Sneakers visit quartiles. Nondepressed and depressed participants were analyzed separately to capture the risk of incident and recurrent depression, respectively. All statistical procedures were performed in 2008 with Stata 9.0.
Results
Silver Sneakers participants and controls who were included in this study (n=13,801) were slightly younger, more often women, had lower RxRisk, and had a higher preventive services index compared to members who were excluded (n=15,845). Compared to matched controls, Silver Sneakers participants were slightly older, more often men, had a lower chronic disease burden, and used more preventive services (Table 1).
Table 1.
Sample characteristics
| Controls
(n=9035) |
Silver Sneakers participants
(n=4766) |
Total included
(n=13,801) |
Excluded
(n=15,845) |
|
|---|---|---|---|---|
| Demographics | ||||
| Age, mean (SD), years | 72 ± 5 | 73 ± 5 | 72 ± 5 | 73 ± 6** |
| Gender (% female) | 5987 (66) | 3012 (63)* | 8999 (65) | 8791 (55)** |
| Comorbiditiesa | ||||
| RxRisk | 2557 ± 1676) | 2416 ± 1443* | 2508 ± 1600 | 2719 ± 2490** |
| Arthritis | 1364 (15) | 961 (20)* | 2325 (17) | 2516 (16)** |
| Coronary artery disease (CAD) | 1087 (12) | 593 (12) | 1680 (12) | 2195 (14)** |
| Heart registry | 1681 (19) | 917 (19) | 2598 (19) | 3295 (21)** |
| Congestive heart failure (CHF) | 412 (5) | 145 (3)* | 557 (4) | 1245 (8)** |
| Hypertension (HTN) | 2233 (25) | 1129 (24) | 3362 (24) | 4508 (28)** |
| Diabetes | 1427 (16) | 620 (13)* | 2047 (15) | 2536 (16)** |
| Preventive services indexb | 1.8 ± 1.7 | 2.4 ± 1.8* | 2.0 ± 1.7 | 1.6 ± 1.7** |
| Distance to fitness facility (km)c | 4.0 ± 3.5 | 4.4 ± 6.0* | 4.1 ± 4.5 | 4.1 ± 4.0 |
Values are means ± SD or n (%) unless otherwise stated
RxRisk is expressed as predicted 6-month costs. Higher costs represent higher comorbidity; co-morbid conditions (arthritis, CAD, CHF, HTN, and diabetes) were derived from problem lists for outpatient visits.
Preventive services index is the total number of preventive services that an individual used in the 2 years preceding the index date (colon cancer screening [fecal occult blood test or flexible sigmoidoscopy]; a screening mammogram; prostate cancer screening; an influenza vaccine; or a pneumococcal vaccine [range 0–8]).
Distance to fitness facility for controls was calculated from control’s home address to the nearest possible fitness facility.
p<0.001, controls vs Silver Sneakers participants;
p<0.05 included members versus excluded members; long-term care costs at baseline; <2years of continuous enrollment in health plan or unmatched controls or participants
Association Between Depression and Enrollment in the Silver Sneakers Program
There were similar proportions of Silver Sneakers participants (6.8%) and controls (6.5%) with a diagnosis of depression at any time in the 12 months preceding the index start date. Depression in the 12 months preceding the Silver Sneakers index start date was not significantly associated with Silver Sneakers enrollment in both unadjusted (OR=1.06; 95%CI=0.92, 1.22; p=0.43) and adjusted models (OR=1.03; 95%CI=0.89, 1.20; p=0.67).
Association Between Depression and Time Course of Silver Sneakers Participation
Depressed participants consistently made fewer visits per month compared to nondepressed participants (range= − 0.64 to −1.5 visits). The risk of participation lapse for any month over the 2 years, adjusting for lapses in other months, was significantly higher for depressed participants starting at the 15th month and extending through the 24th month (relative risk [RR]= 1.28, 1.55; p<0.05) (Figure 2). The overall risk of participation lapse was 19% (hazard ratio=1.19; 95%CI=1.04, 1.37; p=0.01) higher in members who were depressed at baseline compared to nondepressed members in the model that adjusted for age, gender, distance, and RxRisk.
Figure 2.
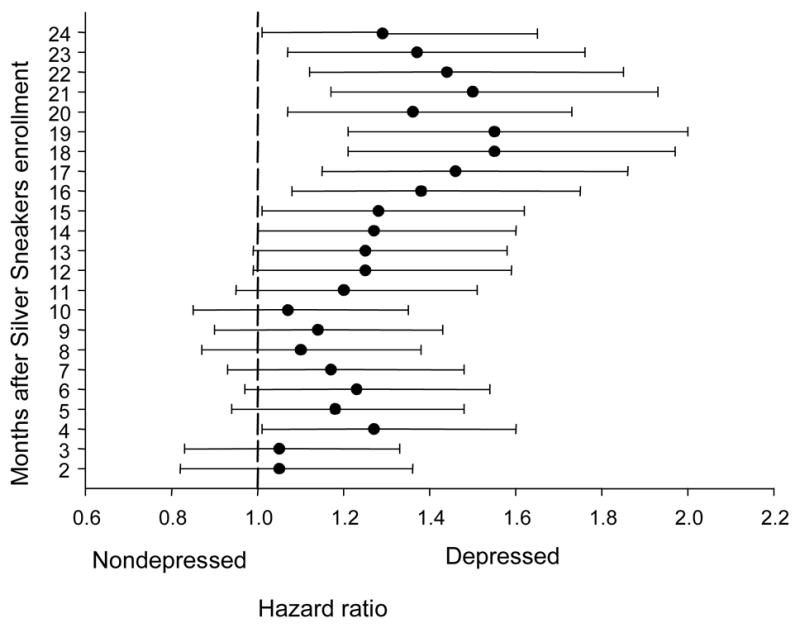
Risk of lapse in Silver Sneakers program attendance over 2 years by baseline depression status (nondepressed: n=4319; depressed: n=326) adjusted for age, gender, RxRisk, and distance to the nearest Silver Sneakers fitness facility. Missing Year 2 attendance for nodepressed Silver Sneakers participants (n=121).
Association Between Silver Sneakers Participation and Depression Risk
Only 151 (3%) of the nondepressed and 4 (1%) depressed Silver Sneakers participants met the recommended PHFD threshold of 5 visits/week (Table 2). For nondepressed Silver Sneakers participants, meeting this threshold was not associated with lower risks for depression in Year 2. However, when comparing visit quartiles, those who made between 121 and 365 total visits over the year, which translates to at least 2 visits per week had a 46% reduction in depression risk in Year 2 (OR=0.54; 95%CI =0.37, 0.79; p=0.002). Similar to the nondepressed participants, the highest visit quartile was significantly associated with lower depression risk in the unadjusted model but was no longer significant in the adjusted model (OR=0.51; 95%CI=0.26, 1.02; p=0.06) in the depressed participants (Table 3).
Table 2.
Risk of incident depression in Year 2 according to attendance dose in Year 1 for nondepressed Silver Sneakers participantsa
| n | Unadjusted OR (95% CI) | p value | Adjustedb OR (95% CI) | p value | |
|---|---|---|---|---|---|
| Silver Sneakers Participation | 4440 | ||||
| <5/week | 4289 | 1.0 | – | 1.0 | – |
| ≥5/week | 151 | 0.83 (0.38, 1.78) | 0.63 | 0.98 (0.45, 2.13) | 0.97 |
| Q1: 0–11 visits/year | 1105 | 1.0 | – | 1.0 | – |
| Q2: 12–49 visits/year | 1086 | 0.70 (0.50, 1.0) | 0.05 | 0.70 (0.50, 1.0) | 0.05 |
| Q3: 50–120 visits/year | 1142 | 0.82 (0.59, 1.13) | 0.23 | 0.83 (0.59, 1.16) | 0.28 |
| Q4: 121–365 visits/year | 1107 | 0.49 (0.34, 0.72) | <0.001 | 0.54 (0.37, 0.79) | 0.002 |
No diagnostic codes for major depression or dysthymic disorder (ICD-9: 296.2, 296.3, 300.4, 311) were assigned in the 12 months preceding Silver Sneakers enrollment.
Adjusted for age, gender, and RxRisk
Table 3.
Risk of recurrent depression in Year 2 according to attendance dose in Year 1 for depressed Silver Sneakers participantsa
| n | Unadjusted OR (95% CI) | p value | Adjustedb OR (95% CI) | p value | |
|---|---|---|---|---|---|
| Silver Sneakers Participation | 326 | ||||
| <5/week | 322 | 1.0 | – | 1.0 | – |
| ≥5/week | 4 | 0.54 (.06, 5.27) | 0.60 | 0.66 (0.06, 7.5) | 0.74 |
| Q1: 0–11 visits/year | 98 | 1.0 | – | 1.0 | – |
| Q2: 12–49 visits/year | 97 | 1.21 (0.68, 2.16) | 0.51 | 1.24 (0.67, 2.25) | 0.47 |
| Q3: 50–120 visits/year | 58 | 0.76 (0.39, 1.51) | 0.44 | 0.87 (0.43, 1.74) | 0.70 |
| Q4: 121–365 visits/year | 73 | 0.47 (0.24, 0.92) | 0.03 | 0.51 (0.26, 1.02) | 0.06 |
At least one diagnostic code for major depression or dysthymic disorder (ICD-9: 296.2, 296.3, 300.4, 311) was assigned in the 12 months preceding Silver Sneakers enrollment
Adjusted for age, gender, and RxRisk
Discussion
The main findings from this study were that: (1) older depressed members of a Medicare HMO were about equally likely to enroll in a health plan–sponsored physical activity benefit as nondepressed members; (2) depressed Silver Sneakers participants were at greater risk for lapse in program attendance over 2 years compared to nondepressed Silver Sneakers participants; and (3) greater participation in the Silver Sneakers program in the first year was associated with lower depression risk in Year 2 for all participants, although this association was significant only for those without previous depression.
Physical inactivity and depression separately and combined place a considerable economic burden on the healthcare system and society.40–42 This is the first study to examine the association between depression and participation in a health plan–sponsored physical activity program in a large cohort of older adults over an extended period of time.
These notable strengths are not without limitations. First, ICD-9-CM diagnostic codes were used to identify members with depression and no pharmacy records were available from the data set, separate from RxRisk, to account for antidepressant use or to cross-validate with the diagnostic codes. Therefore, members who had depression (with or without treatment) but did not receive an ICD-9-CM depression diagnosis during the observation period may have been misclassified as nondepressed. Thus, the study may have included more severely depressed older adults in the group of depressed participants. Nonetheless, the point prevalence for depression in this sample across all 3 years was comparable to estimates from other population-based studies.43 Second, visits to the Silver Sneakers program were used as a proxy for physical activity and there were no information on the exact dose of exercise that members engaged in at the fitness facilities, the “density” of these visits for any particular month, or physical activity that members engaged in outside of the Silver Sneakers program. Third, no data were available on physiological, psychological, or functional measures that might help explain the relationship between depression and physical activity. Finally, although the study was conducted in a large health plan, generalizing these findings to other populations could be limited since GHC members tend to be largely Caucasian and well-educated and those who were included in the study tended to be healthier compared to excluded members.
While contrary to the study hypothesis, the finding that depressed members were as likely to enroll in the Silver Sneakers program as nondepressed members provides some assurance to health plans that uptake of such benefits are comparable across these subpopulations. Public health messages about the influence of physical activity on emotional health in recent years may have increased awareness and prompted depressed members to enroll in physical activity programs. A recent survey showed that adults with a history of clinical depression rated exercise a superior strategy for the management of depression compared to antidepressants and psychotherapy.44 More positive attitudes about exercise, expectations of response, and limited adverse effects are all potential reasons for why older depressed adults in this HMO were equally likely to enroll in the physical activity program as nondepressed members.
Although depressed members were as likely to enroll in the Silver Sneakers program, they consistently made fewer visits to the fitness facilities and had a greater risk of attendance lapse compared to nondepressed Silver Sneakers participants. Previous studies showed that depressed patients have a seven to nine times greater odds of drop-out from short-term rehabilitation programs.45,46 Adherence is also suboptimal.24,26 The Silver Sneakers program may not be the most ideal format for depressed older adults since it includes mostly unsupervised exercise at a fitness facility. Behavioral changes to remain physically active require motivation, confidence, and sustained effort. While exercise may be an effective primary or adjunctive treatment for depression, the benefits will not be realized without ongoing behavioral support for physical activity maintenance.47 The study of physical activity patterns over time in older adults is an area that requires further work including longitudinal modeling of multiple individual, interpersonal, socio-environmental, and exercise-specific variables; understanding how depression interacts with these variables will be essential for developing more cost effective, patient-centered supportive physical activity intervention schemes.
The results of the third exploratory aim that examined the association between participation and risk of receiving a depression diagnosis a year later are partially consistent with published literature. A key limitation of the analyses was the reliance on Silver Sneakers program attendance records as a measure of physical activity. Thus, many Silver Sneakers participants could have been misclassified as not meeting the public health exercise frequency “dose” threshold when they may have if their physical activity outside of the Silver Sneakers program had been counted. The model based on quartiles of Silver Sneakers visits suggests that for nondepressed Silver Sneakers participants, as few as two visits per week to the Silver Sneakers program may translate to lower risk of incident depression if the association is truly causal. The estimate of effects for the depressed participants was limited by the smaller sample size. Some studies showed that fitness was associated with reduction of symptoms while others demonstrated reduction in symptoms without increased fitness. Blumenthal et al.24 showed that greater attendance and higher exercise intensity were related to improvements in aerobic capacity and that change in aerobic capacity was related to reductions in depressive symptoms in older adults. Three months of aerobic exercise performed in an exercise laboratory at a cumulative caloric dose consistent with public health physical activity recommendations49 was more effective in reducing depressive symptoms and inducing remission compared to a lower total dose of exercise in young adults with major depression.29 The frequency of exercise sessions (3 vs 5 times/week) was not associated with depression response.29 Positive social support gained from exercising in group settings may mediate the relationship between visit dose and improvement in depressive symptoms. Frequent attendance is associated with social support and the more one attends, the more therapeutic benefit may be received.50 Interestingly, a recent study showed comparable improvements in depression with both home and group-based exercise.26
Conclusion
While depressed older adults were as likely to enroll in a health plan–sponsored physical activity program as nondepressed members, once enrolled, they had a significantly higher risk of attendance lapses over 2 years. Based on Silver Sneakers program attendance records, only 3% of all Silver Sneakers participants actually met the public health exercise dose recommendation of 5 times per week. Greater participation in the physical activity program was associated with lower depression risk, but significantly so only in participants without a history of depression.
Acknowledgments
The authors would like to acknowledge the support of Dr. Elizabeth Lin and staff at the Center for Health Studies of Group Health Cooperative of Puget Sound.
Funding/Support. This study was funded in part by the University of Washington Health Promotion and Research Center (CDC, U48-DP-000050) and 1KL2RR025015-01 from the National Center for Research Resources (NCRR), a component of the NIH and NIH Roadmap for Medical Research; its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. Information on NCRR is available at http://www.ncrr.nih.gov/. Information on Re-engineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.
Footnotes
No financial disclosures were reported by the authors of this paper.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Martinson BC, O'Connor PJ, Pronk NP. Physical inactivity and short-term all-cause mortality in adults with chronic disease. Arch Intern Med. 2001;161(9):1173–80. doi: 10.1001/archinte.161.9.1173. [DOI] [PubMed] [Google Scholar]
- 2.Kushi LH, Fee RM, Folsom AR, Mink PJ, Anderson KE, Sellers TA. Physical activity and mortality in postmenopausal women. JAMA. 1997;277(16):1287–92. [PubMed] [Google Scholar]
- 3.Pratt M, Macera C, Wang G. Higher direct medical costs associated with physical inactivity. Phys Sportsmed. 2000;28(10):63–70. doi: 10.3810/psm.2000.10.1237. [DOI] [PubMed] [Google Scholar]
- 4.Carlsson S, Andersson T, Wolk A, Ahlbom A. Low physical activity and mortality in women: baseline lifestyle and health as alternative explanations. Scand J Public Health. 2006;34(5):480–7. doi: 10.1080/14034940600551293. [DOI] [PubMed] [Google Scholar]
- 5.USDHHS, CDC. Prevention Behavioral Risk Factor Surveillance System. Available at www.cdc.gov/nccdphp/dnpa/physical/stats/index.htm.
- 6.King AC, Rejeski WJ, Buchner DM. Physical activity interventions targeting older adults: a critical review and recommendations. Am J Prev Med. 1998;15(4):316–33. doi: 10.1016/s0749-3797(98)00085-3. [DOI] [PubMed] [Google Scholar]
- 7.Prohaska T, Belansky E, Belza B, et al. Physical activity, public health, and aging: critical issues and research priorities. J Gerontol B Psychol Sci Soc Sci. 2006;61(5):S267–73. doi: 10.1093/geronb/61.5.s267. [DOI] [PubMed] [Google Scholar]
- 8.Satariano WA, McAuley E. Promoting physical activity among older adults: from ecology to the individual. Am J Prev Med. 2003;25(3S2):184–92. doi: 10.1016/s0749-3797(03)00183-1. [DOI] [PubMed] [Google Scholar]
- 9.DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101–7. doi: 10.1001/archinte.160.14.2101. [DOI] [PubMed] [Google Scholar]
- 10.Lin EH, Katon W, Von Korff M, et al. Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care. 2004;27(9):2154–60. doi: 10.2337/diacare.27.9.2154. [DOI] [PubMed] [Google Scholar]
- 11.Dishman RK, Berthoud HR, Booth FW, et al. Neurobiology of exercise. Obesity (Silver Spring) 2006;14(3):345–56. doi: 10.1038/oby.2006.46. [DOI] [PubMed] [Google Scholar]
- 12.Brown WJ, Ford JH, Burton NW, Marshall AL, Dobson AJ. Prospective study of physical activity and depressive symptoms in middle-aged women. Am J Prev Med. 2005;29(4):265–72. doi: 10.1016/j.amepre.2005.06.009. [DOI] [PubMed] [Google Scholar]
- 13.Camacho TC, Roberts RE, Lazarus NB, Kaplan GA, Cohen RD. Physical activity and depression: evidence from the Alameda County Study. Am J Epidemiol. 1991;134(2):220–31. doi: 10.1093/oxfordjournals.aje.a116074. [DOI] [PubMed] [Google Scholar]
- 14.Harris AH, Cronkite R, Moos R. Physical activity, exercise coping, and depression in a 10-year cohort study of depressed patients. J Affect Disord. 2006;93(1–3):79–85. doi: 10.1016/j.jad.2006.02.013. [DOI] [PubMed] [Google Scholar]
- 15.Lampinen P, Heikkinen RL, Kauppinen M, Heikkinen E. Activity as a predictor of mental well-being among older adults. Aging Ment Health. 2006;10(5):454–66. doi: 10.1080/13607860600640962. [DOI] [PubMed] [Google Scholar]
- 16.Lampinen P, Heikkinen RL, Ruoppila I. Changes in intensity of physical exercise as predictors of depressive symptoms among older adults: an eight-year follow-up. Prev Med. 2000;30(5):371–80. doi: 10.1006/pmed.2000.0641. [DOI] [PubMed] [Google Scholar]
- 17.Wise LA, Adams-Campbell LL, Palmer JR, Rosenberg L. Leisure time physical activity in relation to depressive symptoms in the Black Women's Health Study. Ann Behav Med. 2006;32(1):68–76. doi: 10.1207/s15324796abm3201_8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women. The Women's Health Initiative (WHI) Arch Intern Med. 2004;164(3):289–98. doi: 10.1001/archinte.164.3.289. [DOI] [PubMed] [Google Scholar]
- 19.Paffenbarger RS, Jr, Lee IM, Leung R. Physical activity and personal characteristics associated with depression and suicide in American college men. Acta Psychiatr Scand Suppl. 1994;377:16–22. doi: 10.1111/j.1600-0447.1994.tb05796.x. [DOI] [PubMed] [Google Scholar]
- 20.Strawbridge WJ, Deleger S, Roberts RE, Kaplan GA. Physical activity reduces the risk of subsequent depression for older adults. Am J Epidemiol. 2002;156(4):328–34. doi: 10.1093/aje/kwf047. [DOI] [PubMed] [Google Scholar]
- 21.Emery CF, Gatz M. Psychological and cognitive effects of an exercise program for community-residing older adults. Gerontologist. 1990;30(2):184–8. doi: 10.1093/geront/30.2.184. [DOI] [PubMed] [Google Scholar]
- 22.King AC, Taylor CB, Haskell WL. Effects of differing intensities and formats of 12 months of exercise training on psychological outcomes in older adults. Health Psychol. 1993;12(4):292–300. doi: 10.1037//0278-6133.12.4.292. [DOI] [PubMed] [Google Scholar]
- 23.Penninx BW, Rejeski WJ, Pandya J, et al. Exercise and depressive symptoms: a comparison of aerobic and resistance exercise effects on emotional and physical function in older persons with high and low depressive symptomatology. J Gerontol B Psychol Sci Soc Sci. 2002;57(2):124–32. doi: 10.1093/geronb/57.2.p124. [DOI] [PubMed] [Google Scholar]
- 24.Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159(19):2349–56. doi: 10.1001/archinte.159.19.2349. [DOI] [PubMed] [Google Scholar]
- 25.Singh NA, Stavrinos TM, Scarbek Y, Galambos G, Liber C, Fiatarone Singh MA. A randomized controlled trial of high versus low intensity weight training versus general practitioner care for clinical depression in older adults. J Gerontol A Biol Sci Med Sci. 2005;60(6):768–76. doi: 10.1093/gerona/60.6.768. [DOI] [PubMed] [Google Scholar]
- 26.Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. 2007;69(7):587–96. doi: 10.1097/PSY.0b013e318148c19a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Brenes GA, Williamson JD, Messier SP, et al. Treatment of minor depression in older adults: a pilot study comparing sertraline and exercise. Aging Ment Health. 2007;11(1):61–8. doi: 10.1080/13607860600736372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mather AS, Rodriguez C, Guthrie MF, McHarg AM, Reid IC, McMurdo ME. Effects of exercise on depressive symptoms in older adults with poorly responsive depressive disorder: randomised controlled trial. Br J Psychiatry. 2002;180:411–5. doi: 10.1192/bjp.180.5.411. [DOI] [PubMed] [Google Scholar]
- 29.Dunn AL, Trivedi MH, Kampert JB, Clark CG, Chambliss HO. Exercise treatment for depression: efficacy and dose response. Am J Prev Med. 2005;28(1):1–8. doi: 10.1016/j.amepre.2004.09.003. [DOI] [PubMed] [Google Scholar]
- 30.Donesky-Cuenco D, Janson S, Neuhaus J, Neilands TB, Carrieri-Kohlman V. Adherence to a home-walking prescription in patients with chronic obstructive pulmonary disease. Heart Lung. 2007;36(5):348–63. doi: 10.1016/j.hrtlng.2006.11.004. [DOI] [PubMed] [Google Scholar]
- 31.Wilbur J, Chandler P, Miller AM. Measuring adherence to a women's walking program. West J Nurs Res. 2001;23(1):8–24. doi: 10.1177/01939450122044934. discussion 24–32. [DOI] [PubMed] [Google Scholar]
- 32.USDHHS. Physical activity and health: a report of the Surgeon General. Atlanta: USDHHS, CCDC, National Center for Chronic Disease Prevention and Health Promotion; 1996. [Google Scholar]
- 33.Nelson ME, Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116(9):1094–1105. doi: 10.1161/CIRCULATIONAHA.107.185650. [DOI] [PubMed] [Google Scholar]
- 34.Putnam KG, Buist DS, Fishman P, et al. Chronic disease score as a predictor of hospitalization. Epidemiology. 2002;13(3):340–6. doi: 10.1097/00001648-200205000-00016. [DOI] [PubMed] [Google Scholar]
- 35.Maciejewski ML, Liu CF, Derleth A, McDonell M, Anderson S, Fihn SD. The performance of administrative and self-reported measures for risk adjustment of Veterans Affairs expenditures. Health Serv Res. 2005;40(3):887–904. doi: 10.1111/j.1475-6773.2005.00390.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Fishman PA, Goodman MJ, Hornbrook MC, Meenan RT, Bachman DJ, O'Keeffe Rosetti MC. Risk adjustment using automated ambulatory pharmacy data: the RxRisk model. Med Care. 2003;41(1):84–99. doi: 10.1097/00005650-200301000-00011. [DOI] [PubMed] [Google Scholar]
- 37.Nguyen HQ, Ackermann RT, Berke EM, et al. Impact of a managed-Medicare physical activity benefit on health care utilization and costs in older adults with diabetes. Diabetes Care. 2007;30(1):43–8. doi: 10.2337/dc06-1013. [DOI] [PubMed] [Google Scholar]
- 38.Unutzer J, Patrick DL, Simon G, et al. Depressive symptoms and the cost of health services in HMO patients aged 65 years and older: a 4-year prospective study. JAMA. 1997;277(20):1618–23. doi: 10.1001/jama.1997.03540440052032. [DOI] [PubMed] [Google Scholar]
- 39.Berke EM, Ackermann RT, Lin EH, et al. Distance as a barrier to using a fitness-program benefit for managed Medicare enrollees. J Aging Phys Act. 2006;14(3):313–24. doi: 10.1123/japa.14.3.313. [DOI] [PubMed] [Google Scholar]
- 40.Colditz GA. Economic costs of obesity and inactivity. Med Sci Sports Exerc. 1999;31(11S):S663–7. doi: 10.1097/00005768-199911001-00026. [DOI] [PubMed] [Google Scholar]
- 41.Garrett NA, Brasure M, Schmitz KH, Schultz MM, Huber MR. Physical inactivity: direct cost to a health plan. Am J Prev Med. 2004;27(4):304–9. doi: 10.1016/j.amepre.2004.07.014. [DOI] [PubMed] [Google Scholar]
- 42.Katzmarzyk PT, Gledhill N, Shephard RJ. The economic burden of physical inactivity in Canada. CMAJ. 2000;163(11):1435–40. [PMC free article] [PubMed] [Google Scholar]
- 43.Lyness JM, Caine ED, King DA, Cox C, Yoediono Z. Psychiatric disorders in older primary care patients. J Gen Intern Med. 1999;14(4):249–54. doi: 10.1046/j.1525-1497.1999.00326.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Parker G, Crawford J. Judged effectiveness of differing antidepressant strategies by those with clinical depression. Aust N Z J Psychiatry Jan. 2007;41(1):32–37. doi: 10.1080/00048670601057726. [DOI] [PubMed] [Google Scholar]
- 45.Garrod R, Marshall J, Barley E, Jones PW. Predictors of success and failure in pulmonary rehabilitation. Eur Respir J. 2006;27(4):788–94. doi: 10.1183/09031936.06.00130605. [DOI] [PubMed] [Google Scholar]
- 46.Glazer KM, Emery CF, Frid DJ, Banyasz RE. Psychological predictors of adherence and outcomes among patients in cardiac rehabilitation. J Cardiopulm Rehabil. 2002;22(1):40–6. doi: 10.1097/00008483-200201000-00006. [DOI] [PubMed] [Google Scholar]
- 47.Trivedi MH, Greer TL, Grannemann BD, et al. TREAD: TReatment with Exercise Augmentation for Depression: study rationale and design. Clin Trials. 2006;3(3):291–305. doi: 10.1191/1740774506cn151oa. [DOI] [PubMed] [Google Scholar]
- 48.Dunn AL, Trivedi MH, O'Neal HA. Physical activity dose-response effects on outcomes of depression and anxiety. Med Sci Sports Exerc. 2001;33(6S):S587–97. doi: 10.1097/00005768-200106001-00027. discussion 609–510. [DOI] [PubMed] [Google Scholar]
- 49.Haskell WL, Lee IM, Pate RR, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116(9):1081–93. doi: 10.1161/CIRCULATIONAHA.107.185649. [DOI] [PubMed] [Google Scholar]
- 50.Herman S, Blumenthal JA, Babyak M, et al. Exercise therapy for depression in middle-aged and older adults: predictors of early dropout and treatment failure. Health Psychol. 2002;21(6):553–63. [PubMed] [Google Scholar]