

Abstract
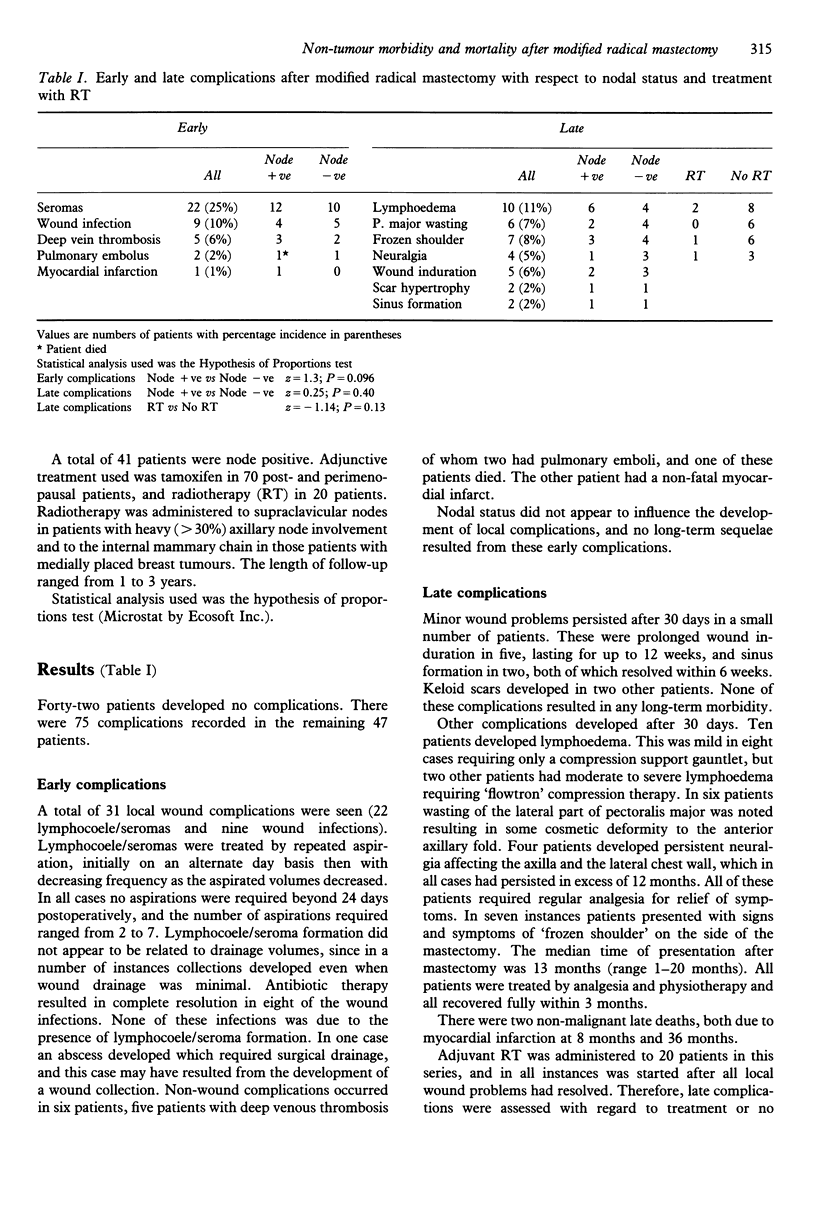
From 1985 to 1987 148 patients underwent mastectomy for breast cancer, of whom 91 underwent modified radical mastectomy. Of these patients (median age 60 years (range 31-86 years)), 89 have been assessed for early (< 30 days) and late (> 30 days) non-tumour morbidity and mortality. A total of 41 patients had nodal metastases. Adjunctive therapy used was tamoxifen in 70 patients and radiotherapy in 20. Overall, 47 patients (53%) developed a total of 75 complications, and there was one 30-day mortality. Of the patients, 26 developed one complication, 14 had two complications and 7 three complications. Early complications were lymphocoele/seroma (n = 22), wound infection (n = 9) and cardiopulmonary problems (five deep vein thrombosis, two pulmonary embolus (1 death), one myocardial infarct). Late complications were lymphoedema (n = 10), pectoralis major wasting (n = 6), frozen shoulder (n = 7), intercostobrachial neuralgia (n = 4), and a small number of self-limiting wound problems (n = 9). There were two late deaths (myocardial infarcts). Early complications were not related to nodal status, and late complications were related to neither nodal status nor radiotherapy. Significant morbidity is attached to radical surgery for breast cancer. Most complications are minor and self-limiting, but there are a small number of late complications which may affect quality of life.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bryant M., Baum M. Postoperative seroma following mastectomy and axillary dissection. Br J Surg. 1987 Dec;74(12):1187–1187. doi: 10.1002/bjs.1800741239. [DOI] [PubMed] [Google Scholar]
- Chiverton S. G., Perry P. M. Morbidity after surgery for breast cancer. Br J Surg. 1987 Dec;74(12):1166–1166. doi: 10.1002/bjs.1800741222. [DOI] [PubMed] [Google Scholar]
- Fisher B., Bauer M., Margolese R., Poisson R., Pilch Y., Redmond C., Fisher E., Wolmark N., Deutsch M., Montague E. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med. 1985 Mar 14;312(11):665–673. doi: 10.1056/NEJM198503143121101. [DOI] [PubMed] [Google Scholar]
- Muscolino G., Leo E., Sacchini V., Bedini A. V., Luini A. Resectable breast cancer: axillary dissection sparing pectoralis muscles and nerves. Eur J Surg Oncol. 1988 Oct;14(5):429–433. [PubMed] [Google Scholar]
- Sarrazin D., Dewar J. A., Arriagada R., Benhamou S., Benhamou E., Lasser P., Fontaine F., Travagli J. P., Spielmann M., Le Chevalier T. Conservative management of breast cancer. Br J Surg. 1986 Aug;73(8):604–606. doi: 10.1002/bjs.1800730804. [DOI] [PubMed] [Google Scholar]
- Temple W. J., Ketcham A. S. Preservation of the intercostobrachial nerve during axillary dissection for breast cancer. Am J Surg. 1985 Nov;150(5):585–588. doi: 10.1016/0002-9610(85)90442-8. [DOI] [PubMed] [Google Scholar]