

Abstract
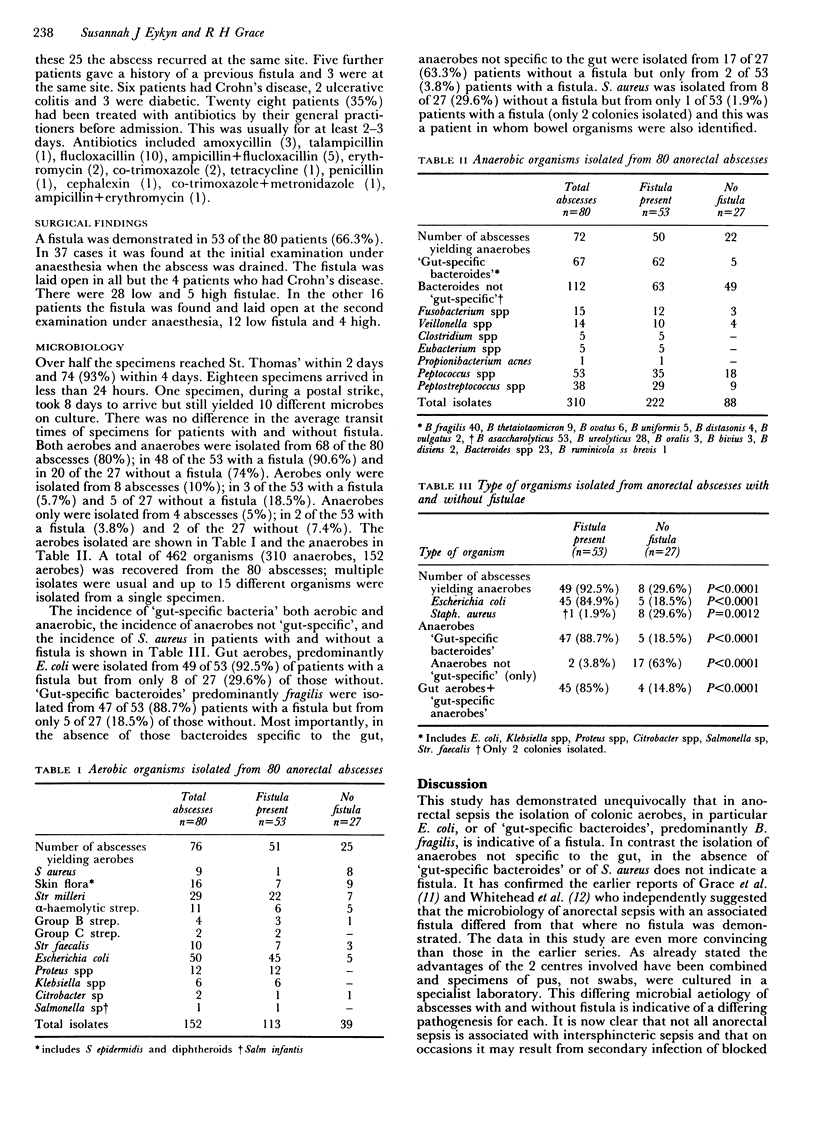
Eighty patients with anorectal sepsis were studied over three years. All abscesses were drained and pus was submitted for culture. If a fistula was found when the abscess was drained it was laid open otherwise a second examination under anaesthetic was performed within 7-10 days. In no case was sterile pus obtained. Gut aerobes, predominantly Escherichia coli, were isolated from 49 of 53 (92.5%) of patients with a fistula and 8 of 27 (29.6%) of those without. 'Gut-specific bacteroides' predominantly Bacteroides fragilis were isolated from 47 of 53 (88.7%) patients with a fistula and 5 of 27 (18.5%) of those without. Anaerobes not specific to the gut, predominantly B. asaccharolyticus, B. ureolyticus, peptococci and peptostreptococci, in the absence of those specific to the gut, were isolated from 2 of 53 patients with a fistula (3.8%) and 17 of 27 (63%) of those without. Staphylococcus aureus was isolated from only 1 of 53 (1.9%) patients with a fistula but from 8 of 27 (29.6%) of those without. It is concluded that only patients with gut-specific organisms should be submitted to a second examination under anaesthetic and that culture of pus in anorectal sepsis is an essential part of its management.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Buchan R., Grace R. H. Anorectal suppuration: the results of treatment and the factors influencing the recurrence rate. Br J Surg. 1973 Jul;60(7):537–540. doi: 10.1002/bjs.1800600711. [DOI] [PubMed] [Google Scholar]
- EISENHAMMER S. A new approach to the anorectal fistulous abscess based on the high intermuscular lesion. Surg Gynecol Obstet. 1958 May;106(5):595–599. [PubMed] [Google Scholar]
- EISENHAMMER S. The anorectal and anovulval fistulous abscess. Surg Gynecol Obstet. 1961 Oct;113:519–520. [PubMed] [Google Scholar]
- EISENHAMMER S. The internal anal sphincter and the anorectal abscess. Surg Gynecol Obstet. 1956 Oct;103(4):501–506. [PubMed] [Google Scholar]
- ELLIS M. Incision and primary suture of abscesses of the anal region. Proc R Soc Med. 1960 Aug;53:652–653. [PMC free article] [PubMed] [Google Scholar]
- Grace R. H., Harper I. A., Thompson R. G. Anorectal sepsis: microbiology in relation to fistula-in-ano. Br J Surg. 1982 Jul;69(7):401–403. doi: 10.1002/bjs.1800690715. [DOI] [PubMed] [Google Scholar]
- PARKS A. G. Pathogenesis and treatment of fistuila-in-ano. Br Med J. 1961 Feb 18;1(5224):463–469. doi: 10.1136/bmj.1.5224.463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Page R. E., Freeman R. Superficial sepsis: the antibiotic of choice for blind treatment. Br J Surg. 1977 Apr;64(4):281–284. doi: 10.1002/bjs.1800640415. [DOI] [PubMed] [Google Scholar]
- WILSON D. H. THE LATE RESULTS OF ANORECTAL ABSCESS TREATED BY INCISION, CURETTAGE, AND PRIMARY SUTURE UNDER ANTIBIOTIC COVER. Br J Surg. 1964 Nov;51:828–831. doi: 10.1002/bjs.1800511107. [DOI] [PubMed] [Google Scholar]
- Whitehead S. M., Leach R. D., Eykyn S. J., Phillips I. The aetiology of perirectal sepsis. Br J Surg. 1982 Mar;69(3):166–168. doi: 10.1002/bjs.1800690319. [DOI] [PubMed] [Google Scholar]