

Abstract
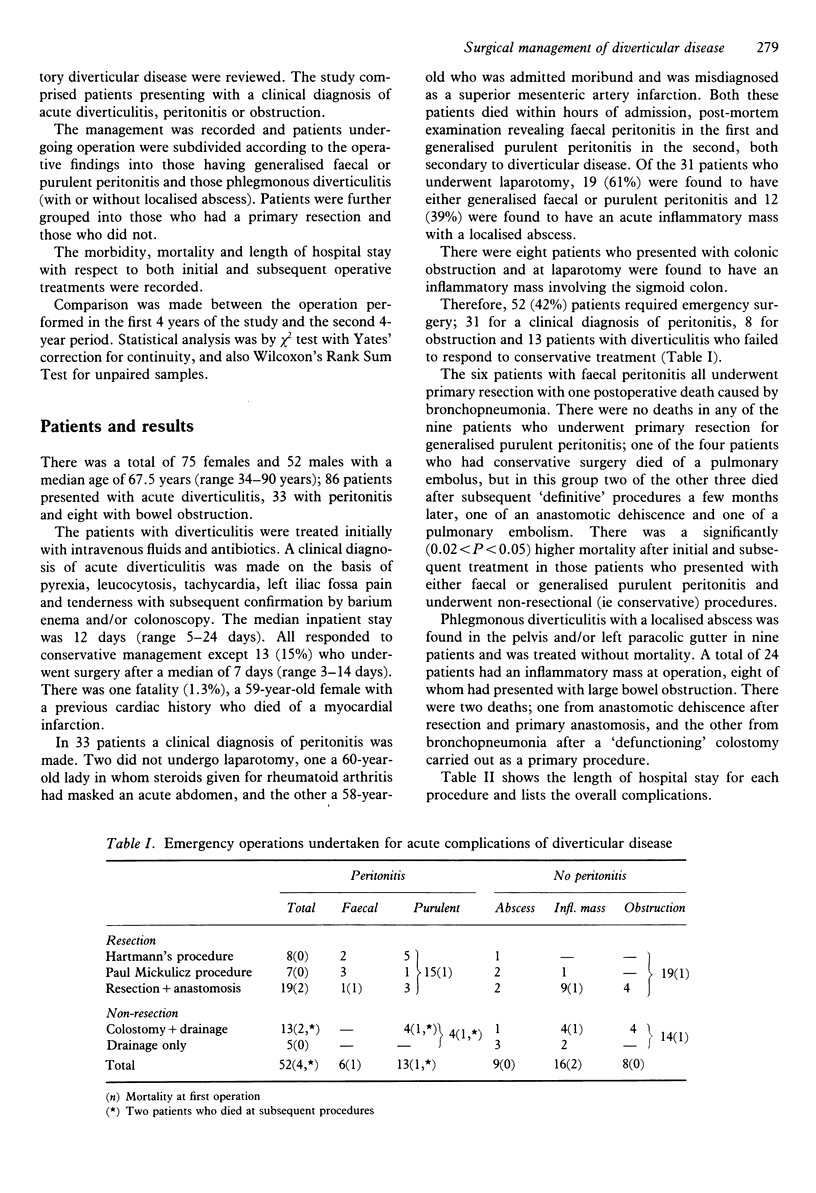
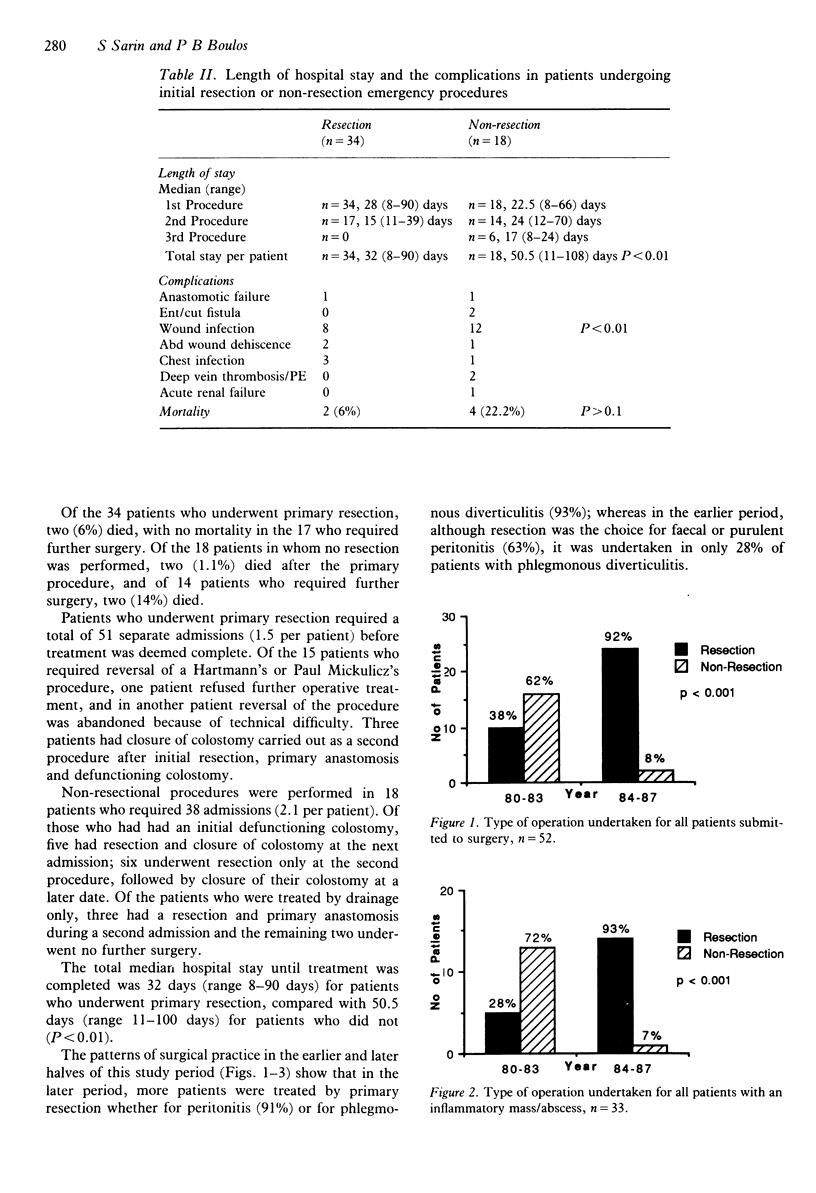
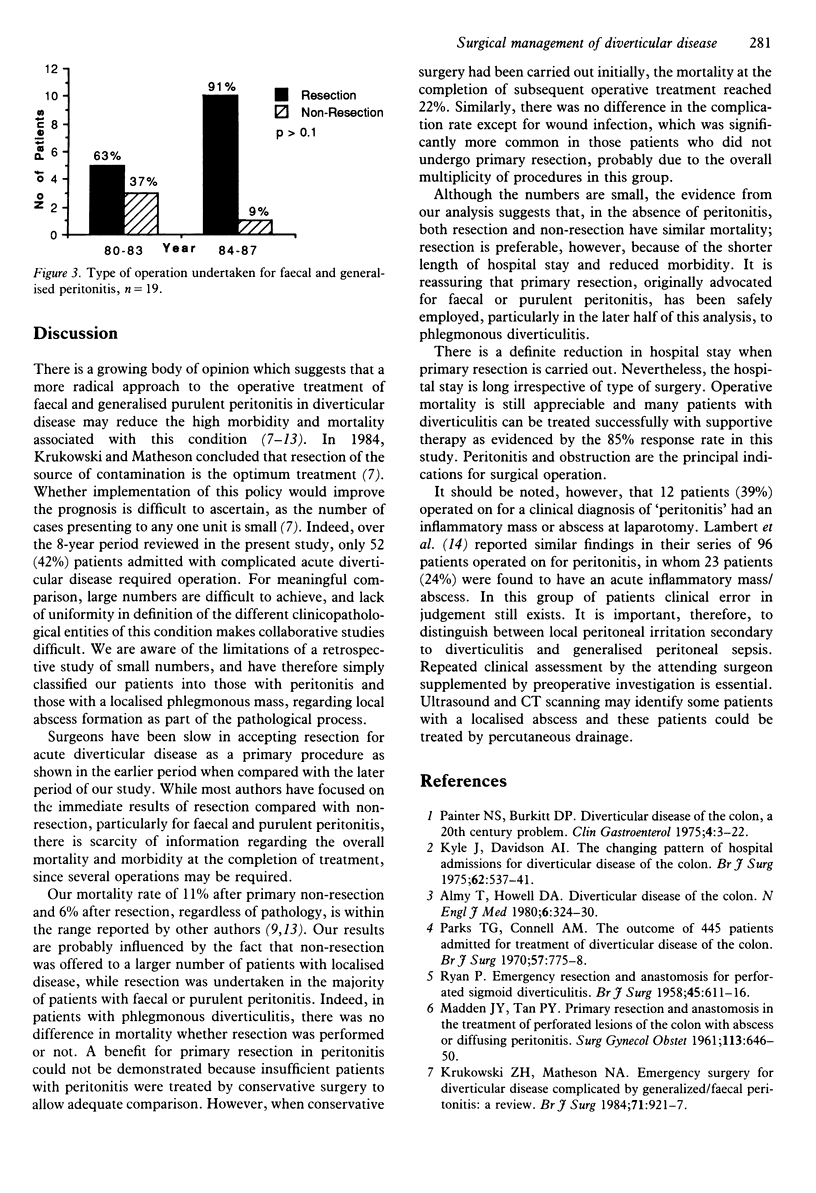
During the period 1980 to 1987, 127 patients were admitted with acute complications of diverticular disease; clinically diagnosed as acute diverticulitis in 86, peritonitis in 33 and colonic obstruction in eight. In those patients diagnosed as acute diverticulitis, conservative treatment was effective in 73 (85%), the other 13 requiring surgery. Of 31 patients, with a clinical diagnosis of peritonitis who underwent operation, 19 (61%) had free purulent or faecal fluid at laparotomy and the remainder had a localised phlegmonous mass. Sigmoid resection was performed in 34 patients and nonexcisional surgery in 18. In the earlier period of the study, there was a preference for the former procedure in patients with peritonitis rather than those with phlegmonous diverticulitis (63% vs 28%), and in the later period of the study, resection was the preferred treatment in both groups (91% vs 93%). The increase in resectional surgery significantly reduced mortality, at completion of treatment, in patients with peritonitis (P less than 0.05) but not in those with phlegmonous diverticulitis. There was an additional benefit of resection in the lower number of procedures per patient (1.5 vs 2.1), a lower median total hospital stay (32 days vs 50.5, P less than 0.01) and a lower wound infection rate (16% vs 32%, P less than 0.01) at the end of treatment. The optimum surgical approach at laparotomy for acutely complicated diverticular disease would therefore appear to be a resectional procedure. Of the patients operated on for 'peritonitis', 39% were found to have a localised diverticular mass/phlegmon.(ABSTRACT TRUNCATED AT 250 WORDS)
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Almy T. P., Howell D. A. Medical progress. Diverticular disease of the colon. N Engl J Med. 1980 Feb 7;302(6):324–331. doi: 10.1056/NEJM198002073020605. [DOI] [PubMed] [Google Scholar]
- Auguste L., Borrero E., Wise L. Surgical management of perforated colonic diverticulitis. Arch Surg. 1985 Apr;120(4):450–452. doi: 10.1001/archsurg.1985.01390280044010. [DOI] [PubMed] [Google Scholar]
- Botsford T. W., Zollinger R. M., Jr, Hicks R. Mortality of the surgical treatment of diverticulitis. Am J Surg. 1971 Jun;121(6):702–705. doi: 10.1016/0002-9610(71)90050-x. [DOI] [PubMed] [Google Scholar]
- Howe H. J., Casali R. E., Westbrook K. C., Thompson B. W., Read R. C. Acute perforations of the sigmoid colon secondary to diverticulitis. Am J Surg. 1979 Feb;137(2):184–187. doi: 10.1016/0002-9610(79)90141-7. [DOI] [PubMed] [Google Scholar]
- Krukowski Z. H., Matheson N. A. Emergency surgery for diverticular disease complicated by generalized and faecal peritonitis: a review. Br J Surg. 1984 Dec;71(12):921–927. doi: 10.1002/bjs.1800711202. [DOI] [PubMed] [Google Scholar]
- Kyle J., Davidson A. I. The changing pattern of hospital admissions for divertical disease of the colon. Br J Surg. 1975 Jul;62(7):537–541. doi: 10.1002/bjs.1800620709. [DOI] [PubMed] [Google Scholar]
- Lambert M. E., Knox R. A., Schofield P. F., Hancock B. D. Management of the septic complications of diverticular disease. Br J Surg. 1986 Jul;73(7):576–579. doi: 10.1002/bjs.1800730721. [DOI] [PubMed] [Google Scholar]
- Liebert C. W., Jr, DeWeese B. M. Primary resection without anastomosis for perforation of acute diverticulitis. Surg Gynecol Obstet. 1981 Jan;152(1):30–32. [PubMed] [Google Scholar]
- MADDEN J. L., TAN P. Y. Primary resection and anastomosis in the treatment of perforated lesions of the colon, with abscess or diffusing peritonitis. Surg Gynecol Obstet. 1961 Nov;113:646–650. [PubMed] [Google Scholar]
- Painter N. S., Burkitt D. P. Diverticular disease of the colon, a 20th century problem. Clin Gastroenterol. 1975 Jan;4(1):3–21. [PubMed] [Google Scholar]
- Parks T. G., Connell A. M. The outcome in 455 patients admitted for treatment of diverticular disease of the colon. Br J Surg. 1970 Oct;57(10):775–778. doi: 10.1002/bjs.1800571021. [DOI] [PubMed] [Google Scholar]
- RYAN P. Emergency resection and anastomosis for perforated sigmoid diverticulitis. Br J Surg. 1958 May;45(194):611–616. doi: 10.1002/bjs.18004519409. [DOI] [PubMed] [Google Scholar]
- Roxburgh R. A., Dawson J. L., Yeo R. Emergency resection in treatment of diverticular disease of colon complicated by peritonitis. Br Med J. 1968 Aug 24;3(5616):465–466. doi: 10.1136/bmj.3.5616.465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Underwood J. W., Marks C. G. The septic complications of sigmoid diverticular disease. Br J Surg. 1984 Mar;71(3):209–211. doi: 10.1002/bjs.1800710314. [DOI] [PubMed] [Google Scholar]