

Abstract
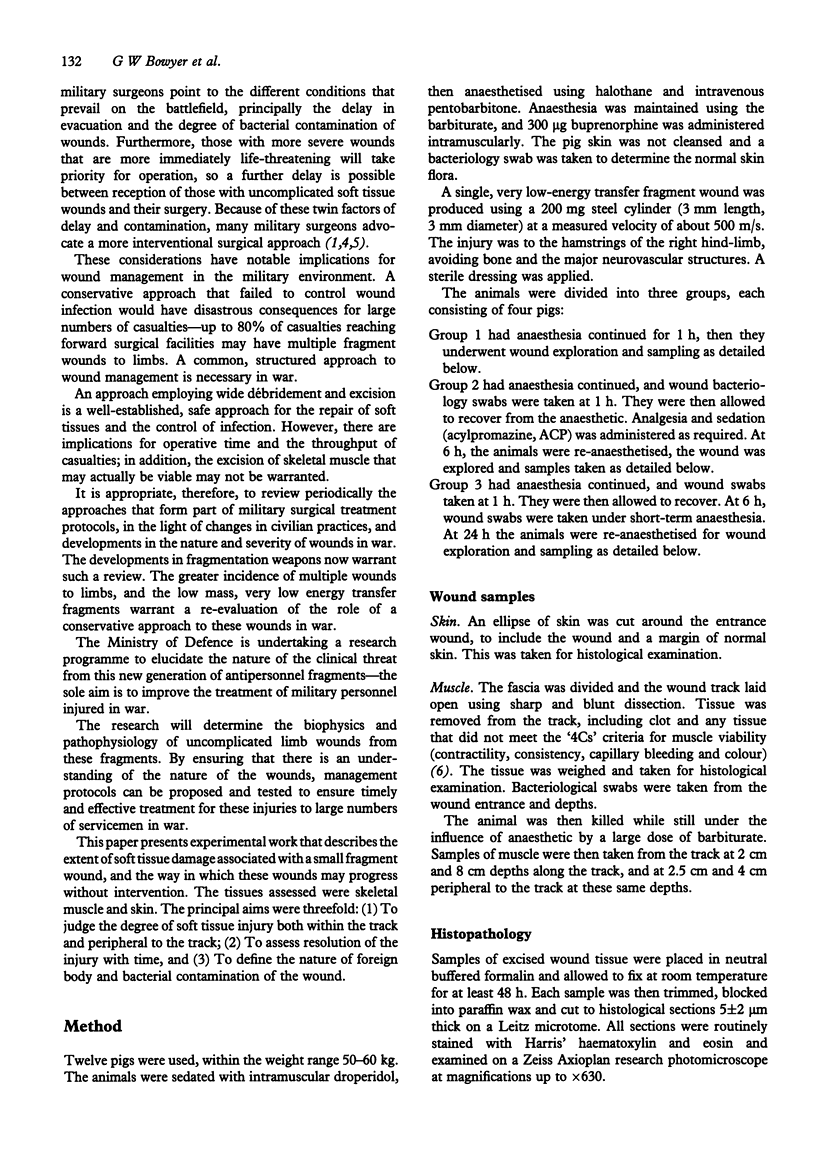
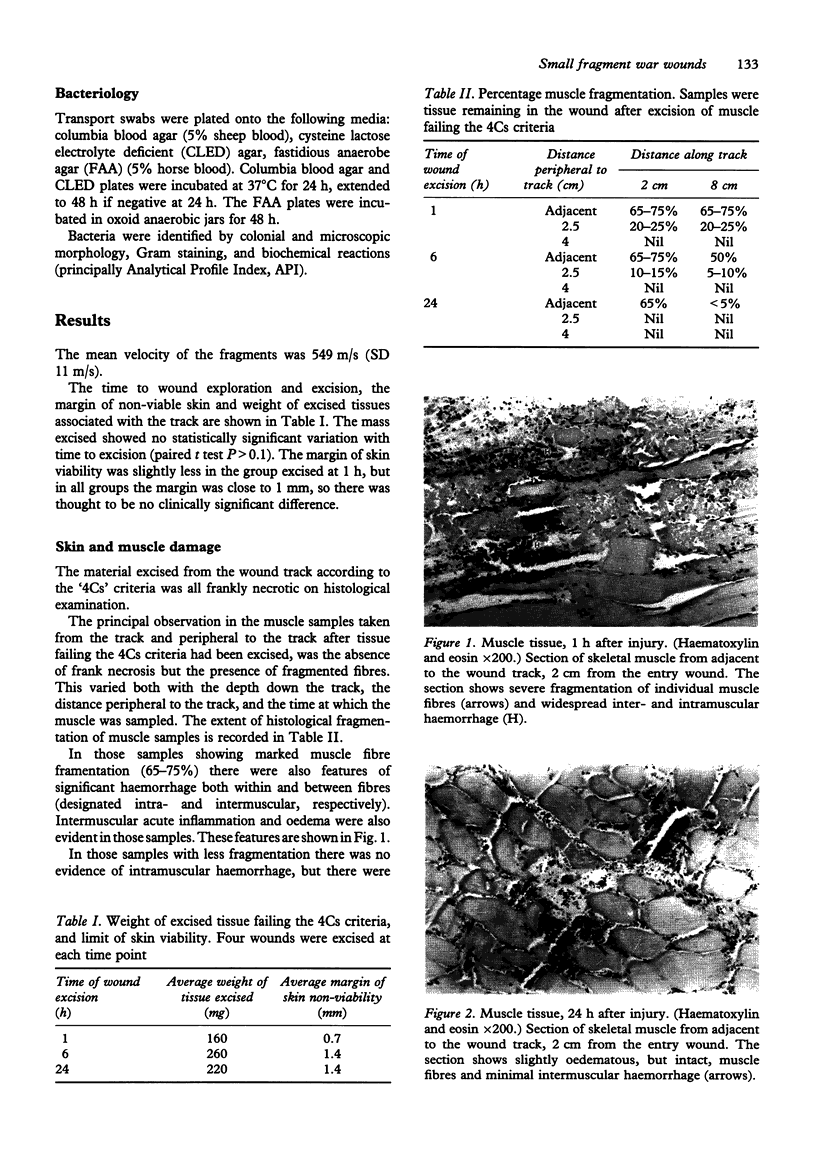
The majority of war wounds are caused by antipersonnel fragments from munitions such as mortars and bomblets. Modern munitions aim to incapacitate soldiers with multiple wounds from very small fragments of low available kinetic energy. Many of these fragments may be stopped by helmets and body armour and this has led to a predominance of multiple wounds to limbs in those casualties requiring surgery. The development of an appropriate management strategy for these multiple wounds requires knowledge of the contamination and extent of soft tissue injury; conservative management may be appropriate. The extent of skin and muscle damage associated with a small fragment wound, the way in which these wounds may progress without intervention and their colonisation by bacteria has been determined in an experimental animal model. Results from 12 animals are presented. There was a very small (approximately 1 mm) margin of nonviable skin around the entrance wound. The amount of devitalised muscle in the wound tract was a few hundred milligrams. Some muscles peripheral to the wound track also showed signs of damage 1 h after wounding, but this improved over 24 h; the proportion of fragmented muscle fibres in the tissue around the track decreased as time went on. There was no clinical sign or bacteriological evidence of the track becoming infected up to 24 h after wounding. This preliminary work suggests that, in the absence of infection, the amount of muscle damage caused by small fragment wounds begins to resolve in the first 24 h after injury, even without surgical intervention.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ARTZ C. P., SAKO Y., SCULLY R. E. An evaluation of the surgeon's criteria for determining the viability of muscle during débridement. AMA Arch Surg. 1956 Dec;73(6):1031–1035. doi: 10.1001/archsurg.1956.01280060131029. [DOI] [PubMed] [Google Scholar]
- Marcus N. A., Blair W. F., Shuck J. M., Omer G. E., Jr Low-velocity gunshot wounds to extremities. J Trauma. 1980 Dec;20(12):1061–1064. doi: 10.1097/00005373-198012000-00010. [DOI] [PubMed] [Google Scholar]
- Ryan J. M., Cooper G. J., Haywood I. R., Milner S. M. Field surgery on a future conventional battlefield: strategy and wound management. Ann R Coll Surg Engl. 1991 Jan;73(1):13–20. [PMC free article] [PubMed] [Google Scholar]
- Ryan J. M., Cooper G. J., Maynard R. L. Wound ballistics: contemporary and future research. J R Army Med Corps. 1988 Oct;134(3):119–125. doi: 10.1136/jramc-134-03-02. [DOI] [PubMed] [Google Scholar]
- Spalding T. J., Stewart M. P., Tulloch D. N., Stephens K. M. Penetrating missile injuries in the Gulf war 1991. Br J Surg. 1991 Sep;78(9):1102–1104. doi: 10.1002/bjs.1800780921. [DOI] [PubMed] [Google Scholar]