

Abstract
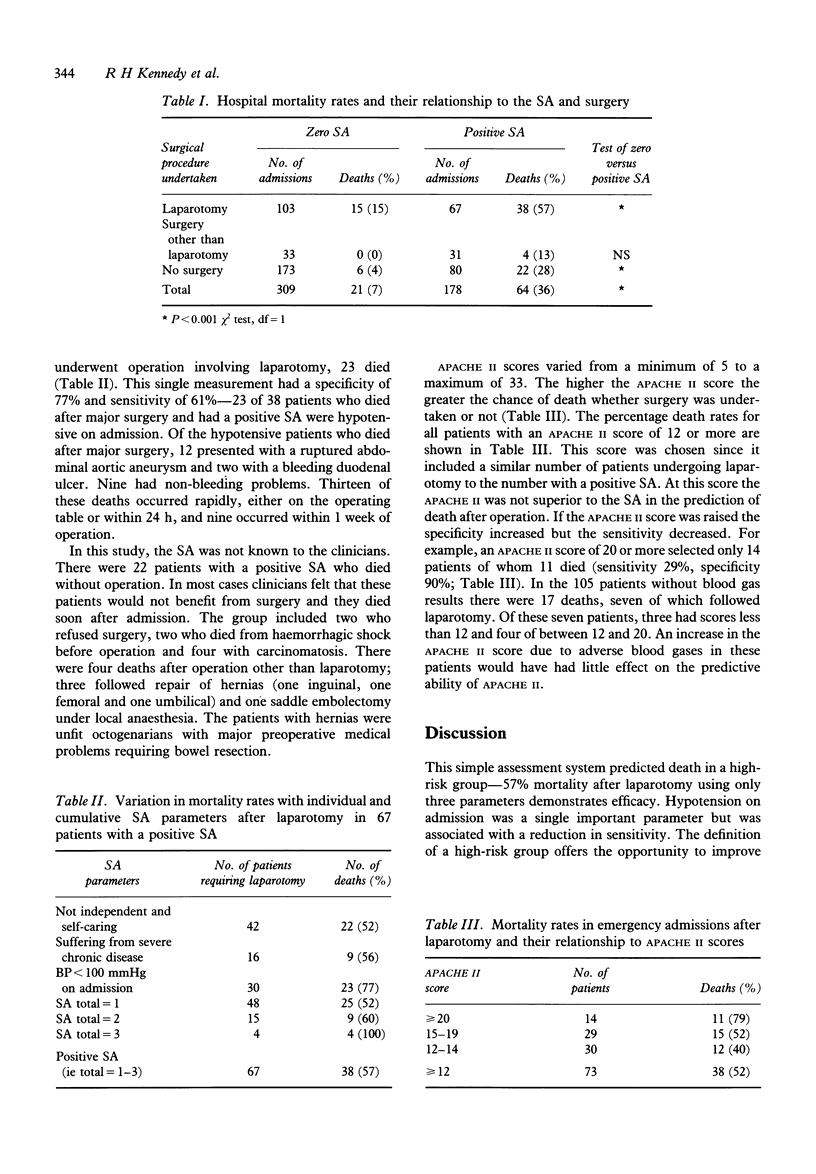
Most scoring systems used to predict mortality are complex. A simple preoperative assessment, the Sickness Assessment (SA), was evaluated as a predictor of mortality in elderly patients admitted as surgical emergencies. The three parameters comprising the SA are: hypotension on admission, the presence of severe chronic disease, whether the patient was independent and self-caring. Prospectively, 487 consecutive patients of over 65 years of age admitted as surgical emergencies were studied. On admission, the SA and the APACHE II score were calculated. Hospital mortality was used as the endpoint. Of 309 patients with zero SA, 21 (7%) died. In 178 with a positive SA, 64 died (36%) (chi 2 = 64.6, P < 0.001). After laparotomy, mortality was 57% (36/67) with a positive SA, but 15% (15/103) with a zero assessment (chi 2 = 33.6, P < 0.001). When the single parameter of hypotension on admission was present, mortality was 77% (23/30). The predictive ability of the APACHE II score was not superior to SA. The SA is a simple preoperative assessment which identifies a high-risk group. It should be used in emergency surgical practice to improve outcome and avoid inappropriate surgery.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bion J. F., Edlin S. A., Ramsay G., McCabe S., Ledingham I. M. Validation of a prognostic score in critically ill patients undergoing transport. Br Med J (Clin Res Ed) 1985 Aug 17;291(6493):432–434. doi: 10.1136/bmj.291.6493.432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boey J., Wong J., Ong G. B. A prospective study of operative risk factors in perforated duodenal ulcers. Ann Surg. 1982 Mar;195(3):265–269. doi: 10.1097/00000658-198203000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Irvin T. T. Mortality and perforated peptic ulcer: a case for risk stratification in elderly patients. Br J Surg. 1989 Mar;76(3):215–218. doi: 10.1002/bjs.1800760304. [DOI] [PubMed] [Google Scholar]
- Knaus W. A., Draper E. A., Wagner D. P., Zimmerman J. E. APACHE II: a severity of disease classification system. Crit Care Med. 1985 Oct;13(10):818–829. [PubMed] [Google Scholar]
- Teres D., Brown R. B., Lemeshow S. Predicting mortality of intensive care unit patients. The importance of coma. Crit Care Med. 1982 Feb;10(2):86–95. doi: 10.1097/00003246-198202000-00004. [DOI] [PubMed] [Google Scholar]