

Abstract
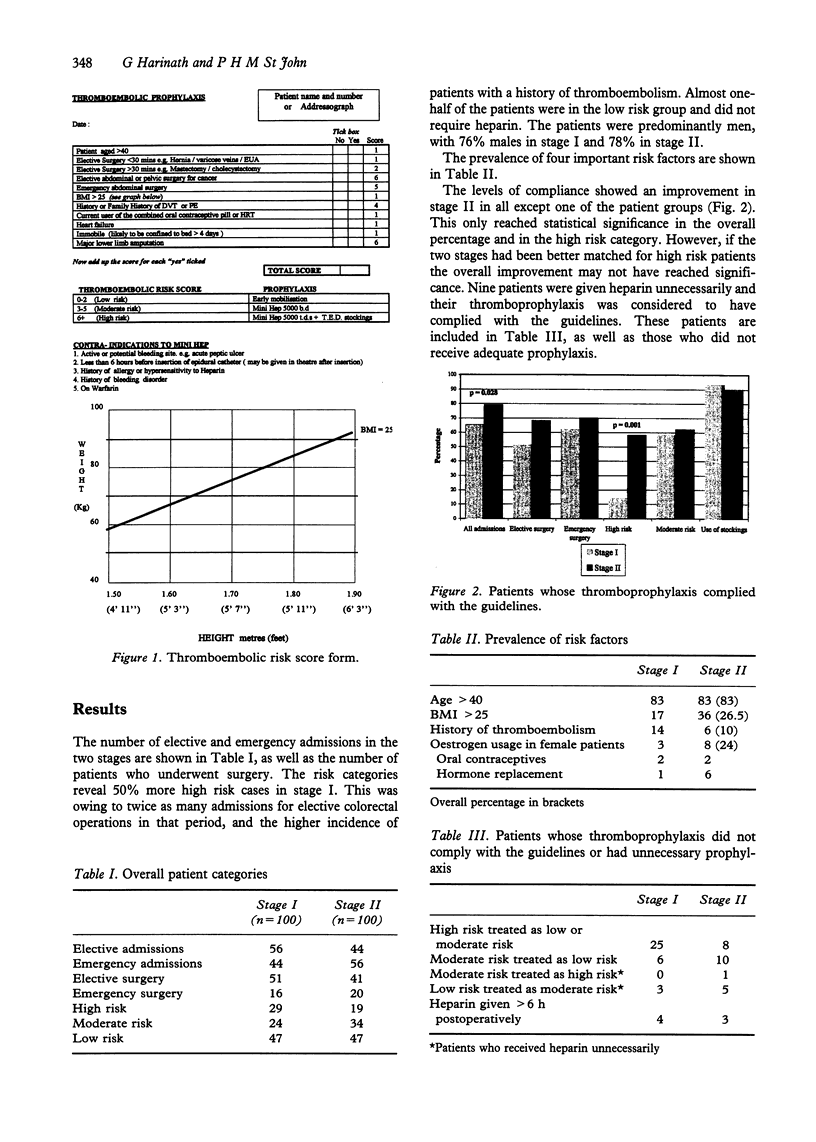
Two hundred admissions to a general surgical ward were audited prospectively before and after the introduction of a thromboembolic risk score. This was based on the Thromboembolic Risk Factors (THRIFT) Consensus Group guidelines for thrombo-prophylaxis. The results showed an overall improvement in compliance from 65% to 79%. High risk patients formed 24% of the patients studied. In this group, compliance improved significantly from 14% to 58%. The overall prevalence of important thromboembolic risk factors was calculated. Of the patients, 26.5% had a Body Mass Index (BMI) of > 25, and 10% gave a past or family history of thromboembolism. Of female patients, 24% were taking oestrogens. We conclude that quantitative assessment of all patients for thromboembolic risk can improve the implementation of thromboprophylaxis, particularly in high risk patients.
Full text
PDF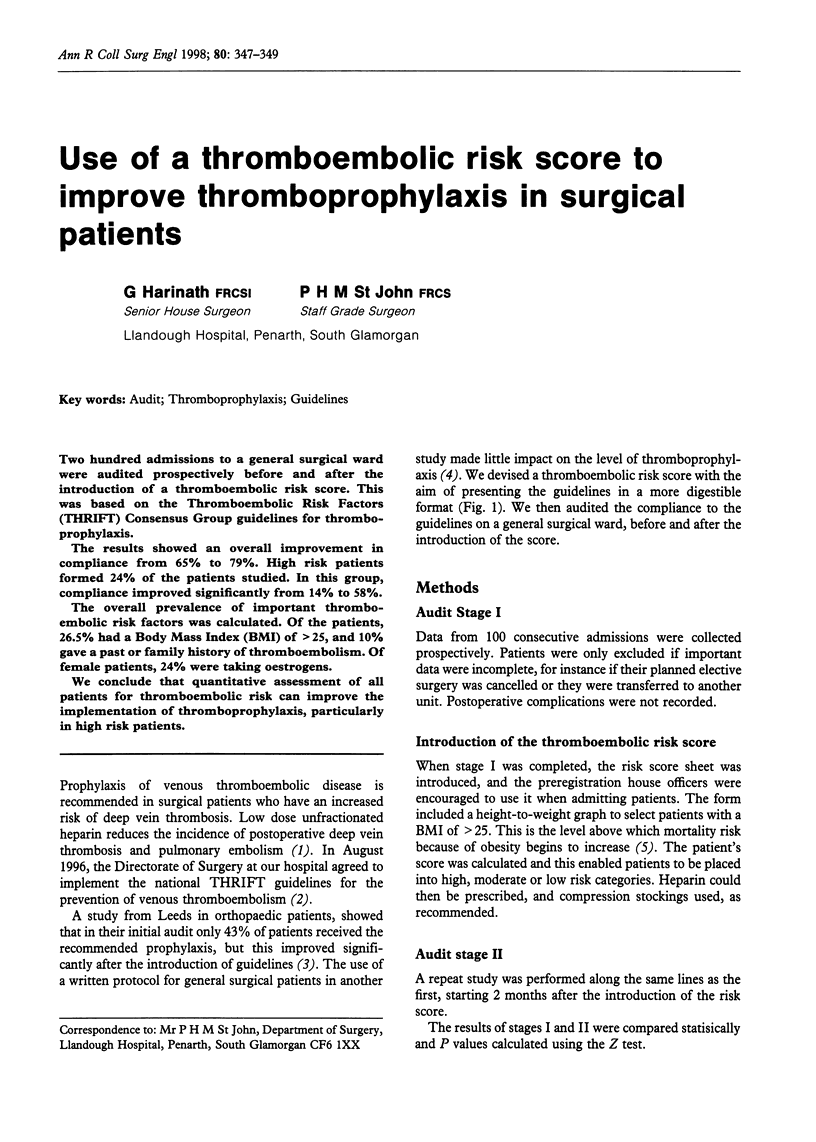

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Collins R., Scrimgeour A., Yusuf S., Peto R. Reduction in fatal pulmonary embolism and venous thrombosis by perioperative administration of subcutaneous heparin. Overview of results of randomized trials in general, orthopedic, and urologic surgery. N Engl J Med. 1988 May 5;318(18):1162–1173. doi: 10.1056/NEJM198805053181805. [DOI] [PubMed] [Google Scholar]
- Daly E., Vessey M. P., Hawkins M. M., Carson J. L., Gough P., Marsh S. Risk of venous thromboembolism in users of hormone replacement therapy. Lancet. 1996 Oct 12;348(9033):977–980. doi: 10.1016/S0140-6736(96)07113-9. [DOI] [PubMed] [Google Scholar]
- George B. D., Cook T. A., Franklin I. J., Nethercliff J., Galland R. B. Protocol violation in deep vein thrombosis prophylaxis. Ann R Coll Surg Engl. 1998 Jan;80(1):55–57. [PMC free article] [PubMed] [Google Scholar]
- Rees D. C., Cox M., Clegg J. B. World distribution of factor V Leiden. Lancet. 1995 Oct 28;346(8983):1133–1134. doi: 10.1016/s0140-6736(95)91803-5. [DOI] [PubMed] [Google Scholar]
- Schuster K. L., Jentschura D. Activated protein C resistance: the commonest hereditary hypercoagulation disorder. Br J Surg. 1997 Dec;84(12):1633–1635. doi: 10.1002/bjs.1800841202. [DOI] [PubMed] [Google Scholar]
- Vessey M., Mant D., Smith A., Yeates D. Oral contraceptives and venous thromboembolism: findings in a large prospective study. Br Med J (Clin Res Ed) 1986 Feb 22;292(6519):526–526. doi: 10.1136/bmj.292.6519.526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams H. R., Macdonald D. A. Audit of thromboembolic prophylaxis in hip and knee surgery. Ann R Coll Surg Engl. 1997 Jan;79(1):55–57. [PMC free article] [PubMed] [Google Scholar]