

Abstract
The purpose of the current study was to examine the effects of a multicomponent intervention that included discrimination training, real-time visual feedback, and self-monitoring on postural behavior at a computer workstation in a simulated office environment. Using a nonconcurrent multiple baseline design across 8 participants, the study assessed the effects of the intervention across three postural variables. Following an information phase, the intervention started for the lowest stable postural variable. The intervention led to substantial improvements in safety behavior for most targeted postural variables. A reversal to the information phase for 2 participants did not lead to decreases in safety. Postures self-monitored with high accuracy improved to a greater degree than postures self-monitored with low accuracy.
Keywords: behavioral safety, computer workstations, ergonomics, feedback, occupational safety
Behavioral safety is an approach to injury reduction that focuses on observable phenomena as they occur in real time, particularly on critical safety behaviors and safety conditions. By focusing on observable events and conditions, behaviors can be managed through, for example, regular performance feedback, goal setting, and rewards (Reber, Wallin, & Chhokar, 1984). Olson and Austin (2001) pointed out that there appears to be a relative dearth of experimental evaluations of behavioral safety applications aimed at lone workers. Behavioral safety processes usually rely heavily on peer-observation and peer-influence techniques (Agnew & Snyder, 2002; McSween, 2003; Van Houten, Van Houten, & Malenfant, 2007). However, when a person works alone for a significant portion of the day, it is not possible to program regular peer safety observations.
A possible solution to the lone-worker dilemma is to have the same person function as an observer and the observed through self-monitoring (Hickman & Geller, 2003a, 2003b; McCann & Sulzer-Azaroff, 1996; Olson & Austin, 2001). For example, McCann and Sulzer-Azaroff used self-monitoring in a treatment package aimed at improving safe sitting posture (back straight, shoulders relaxed, neck aligned with back, feet flat on floor, and forearms parallel to the floor) and hand–wrist position for lone workers using keyboards. Results indicated that training involving safety information combined with self-monitoring was enough to generate improvements in body posture. Training and self-monitoring led to modest improvements in hand–wrist performance, and adding rewards, feedback, and goal setting to the intervention led to more improvements.
Even though self-monitoring has been used frequently as an intervention technique, prior research on self-monitoring as a safety intervention for lone workers has involved relatively few self-monitoring opportunities for participants during the study period. Participants have estimated their safety by reporting one global measure of behavior that occurred over extended periods of time. Olson and Austin (2001) required participants to self-monitor twice daily, participants in Hickman and Geller's (2003a, 2003b) studies self-monitored safety once at the end of the workday, and McCann and Sulzer-Azaroff (1996) required participants to self-monitor posture once following sessions that lasted less than 60 min. Furthermore, prior studies have not used real-time feedback as a data source for self-monitoring, but rather relied on verbal self-reports of behavior after the fact.
Self-monitoring may be an effective intervention for posture improvements, but one subpopulation of lone workers for whom self-monitoring has not been evaluated extensively consists of people who work at computer workstations, also referred to as video display terminal (VDT) operators. One reason that VDT operators merit particular attention is that they are especially at risk for musculoskeletal disorders (MSDs; Kroemer & Grandjean, 1997), which are soft-tissue injuries or disorders of the muscles, nerves, tendons, joints, cartilage, or spinal discs. In fact, nearly one third of all nonfatal injuries resulting in days away from work are MSDs (Occupational Safety and Health Administration [OSHA], 2004b). It has been estimated that the direct cost of MSDs to American private industries may range from $15 to $18 billion a year (OSHA, 2004b), as well as up to three to four times that amount in indirect costs. Recent research has established a link between MSDs and repetitive motion or improper posture at computer workstations (Gerr, Marcus, & Monteilh, 2004; Matias, Salvendy, & Kuczek, 1998), suggesting that interventions designed to improve posture could lead to prevention of MSDs. Therefore, the current study addressed the extent to which a treatment package consisting of real-time visual feedback combined with repeated self-monitoring opportunities was effective at improving posture of participants working at computer workstations, which is important given the low number of studies that have examined the effectiveness of real-time feedback and self-monitoring among VDT workers and the cost of MSDs to society.
Method
Participants and Screening of Participants
A total of 21 individuals participated in screening procedures for participation in the current study. Three participants served as pilot participants, and their data are not presented herein. Two participants did not meet the typing criterion, and 1 participant did not want to be involved in a study in which a video camera was constantly aimed at the participant. Five participants excused themselves from the study after they expressed a desire to terminate their participation because of time constraints, and 2 participants did not have low and stable levels of safe posture during the information phase. The remaining 8 participants were exposed to the intervention and completed the study.
During the screening and consent session, participants (a) had to answer if they were suffering from or had ever suffered from an MSD, (b) signed an informed consent form, and (c) had to demonstrate typing proficiency of 30 words per minute or more. Participation was dependent on an absence of a history of MSD and typing proficiency. In addition, the experimenter asked the participants to complete a postural comfort survey during the screening session and during the intervention phase. The first author used a digital video camera to capture still photographs of each participant while he or she was seated at the computer workstation during the screening and consent session. The camera was in full view of the participants, and they were told that they were being videotaped. Participants had to demonstrate both safe and at-risk postures for periods ranging from 15 s to 30 s during the photographing session and received immediate feedback on whether they were in a safe or at-risk posture. Participants received verbal and physical guidance to demonstrate a safe posture, if necessary.
Apparatus
All experimental sessions were recorded digitally using a JVC JV569 MiniDV digital video camera and a Panasonic DMR-ES10 DVD burner recorded all experimental sessions in their entirety. A Dell Inspiron 8600 laptop computer simultaneously ran a Microsoft Word word processor program and a webcam program throughout all experimental sessions. WebcamDV for personal computers (OrangeWare Corporation, 2005) converted video feed into a Webcam browser, and the Willing Webcam (Detisov, 2005) browser managed feedback windows and captured digital pictures of participants. Pop-up windows containing feedback and self-scoring forms were displayed through an Internet Explorer Web browser. A PHP database that ran on an Apache webserver collected self-scoring data.
Task, Setting, and Workstation Setup
We observed each participant for approximately 20 min per session for up to two sessions per day (with at least a 1-hr break between sessions) as he or she transcribed a text while seated at a computer workstation. During the transcription task, each participant was alone in a room located in the university, and a digital video camera was pointed diagonally at his or her upper body. Participants sat in an office chair with armrests at a desk with an adjustable keyboard tray. We adjusted the computer workstation to fit each individual participant before the start of each session based on OSHA recommendations (2004a) and set chair height so that the participant's feet rested comfortably on the floor or footrest, with the upper body high enough to work comfortably at the workstation and with the thighs resting on the front edge of the chair's seat. The monitor was directly in front of the participant; the center of the monitor was located 15 to 20 degrees below horizontal eye level, and the distance from the participant's eye to the monitor was at least 50 to 100 cm so that the participant did not have to lean back or forward to read. The keyboard was in the center in front of the participant and was flush with the participant's seated elbow height. The keyboard tray sloped away from the participant (i.e., tilted downward). A foam pad was in place in front of the keyboard to elevate the wrists to a neutral position, if needed. A mouse was placed on the same level as the keyboard, and the mouse tray sloped away from the participant to keep the hands and wrists in neutral positions.
Response Measurement and Interobserver Agreement
Safe and at-risk postures (the dependent variables) were based on ergonomic guidelines and recommendations issued by OSHA (2004a). Safe postures were defined for each position as follows. Head–neck position was defined as the head upright (in line with the torso and not bent down or back) or the head facing slightly forward of the plane of the upper body. Back supported was defined as the lower (lumbar) back supported by the chair's back support, and the angle of the back and the thigh was between 100 to 110 degrees while seated. Arms were defined as the inside angle of the elbow between 90 to 120 degrees (not scored when participants were using the computer's mouse). Hand–wrist position was defined as flat wrists (not bent up or down) when typing (not scored when participants were using the computer's mouse). Leg position was defined as the knees bent and forming an angle between 90 to 120 degrees. At-risk postures were all postures that did not meet these definitions of safe postures.
During each session, video files of the session in its entirety were fed to a computer and an external DVD burner for digital storage and later scoring. We used a momentary time-sampling procedure, in which each sample consisted of a snapshot (electronic picture in jpg format) captured at 10-s intervals during each session. Each session yielded 120 samples, and each sample had a time stamp that indicated the day, hour, minute, and second that the picture was taken. Research assistants scored each snapshot of posture on observational datasheets, using the operational definitions described above. For each session, an overall safety score was calculated for each dependent variable. The safety score was calculated by dividing the number of samples scored as safe (numerator) by the total number of samples.
Two observers independently rated all snapshots from 33% of all sessions for interboserver agreement purposes. Agreements were instances in which both observers agreed that a posture was safe or at risk, and disagreements were instances in which one observer scored a posture as safe, whereas the second observed scored the same posture as at risk. We calculated interobserver agreement by dividing the number of agreements by the total number of agreements and disagreements and then converted that ratio to a percentage. Productivity, measured as words typed per minute, was calculated by dividing the number of words typed per session by 20. Mean agreement was 94% overall for all postural behaviors across all participants.
We assessed self-monitoring accuracy by comparing each participant's scoring of his or her own posture with the research assistant's scoring of the digital picture that immediately preceded a given self-monitoring response. For example, if a participant scored a given posture at 10 hr, 25 min, 33 s, the research assistant's scoring of the picture that was shot immediately before that (10 hr, 25 min, 30 s) was used as a comparison. Participants self-monitored accurately if their judgments of safe posture were identical to scoring by research assistants. A measure of a participant's overall self-monitoring accuracy was calculated by dividing the total number of agreements by the total number of self-monitoring responses. Due to technological difficulties, it was not possible to gather self-monitoring accuracy data for all intervention sessions.
Experimental Design
The current study used a nonconcurrent multiple baseline design across participants. We selected this design because few participants exhibited low levels of safety on more than one dependent variable, which precluded the use of a multiple baseline design across behaviors. Furthermore, using a concurrent multiple baseline design was not possible because sessions could not be synchronized across participants due to logistical constraints (e.g., participant and experimental room availability).
Every participant experienced the two phases of the experiment: information and information coupled with live visual feedback and self-monitoring. We exposed participants to the intervention for the postural behaviors that had low and stable levels of safety performance during the information phases. The delivery of the intervention was staggered temporally across participants. We exposed 2 participants to the treatment package for arm position only and exposed 1 of them to a one-session withdrawal to test for maintenance of treatment effects. We exposed 3 participants to the intervention for head–neck position, and 1 of the 3 also received feedback and self-monitoring for arm position. We exposed the last 3 participants to the intervention for back position only, and we also exposed 1 of the 3 to a withdrawal of the intervention.
Information
The first author read an introductory script to each participant before his or her first session of the information phase. The script informed participants that the camera in the experimental room was being used to collect data on their posture and contained instructions for participants for the information phase.
During the first 5 min of each session of the information phase, participants read and initialed a handout that contained definitions of safe posture. Initialing served to indicate that the participants had read the definition. Participants were allowed to start the transcription task only after spending 5 min reading the definitions of safe posture. The function of having participants read the information was to insure that each participant was familiar with the definitions of safe posture during baseline. Therefore, any changes in safe posture that occurred during the intervention phase (safety information, visual feedback, and self-monitoring) could be attributed to the intervention and not to increases in participant knowledge about safe posture. The first author told participants to work at their own pace for 20 min and to take short breaks if they felt fatigued.
Safety Information, Visual Feedback, and Self-Monitoring
Participants continued to receive safety information at the start of each session as described above. Before the first session of the intervention phase, the first author showed participants two to four slides of themselves in a safe posture for the target postural variable and two to four slides of at-risk posture. Slides appeared on the computer on which the participants transcribed text. Participants were then asked to discriminate between slides of safe and at-risk posture based on the operational definitions of safe posture contained on the information sheet. If a participant could not discriminate between slides of safe and at-risk posture, the first author gave him or her verbal corrective feedback on discriminations until the participant was able to discriminate slides of safe and at-risk posture accurately. No limit was set on the amount of verbal feedback given during the discrimination training, and participants had to make three consecutive correct discriminations of safe slides and three consecutive correct discriminations of at-risk slides.
The live video feedback during this phase was broadcast in a pop-up window that appeared at regular intervals on the right side of the computer screen; an example of this display appears in Figure 1. Every time the feedback window appeared, participants were required to score certain dimensions of their own posture as safe or at risk by clicking in designated spaces contained in another window. Participants were instructed to make judgments about their posture based on the image they saw of themselves the first time they looked at the feedback window. The act of self-scoring closed the feedback window. The feedback window reappeared 50 s after the participant self-scored, and participants had to self-score again. Self-scoring was required on this schedule for the duration of the entire session.
Figure 1.
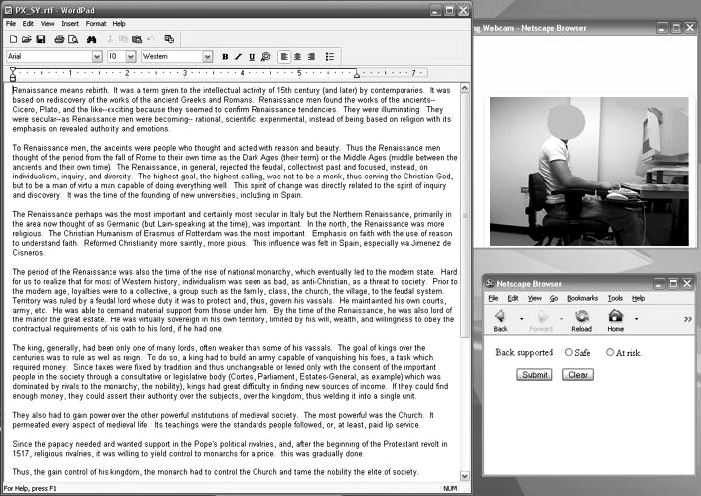
Screenshot of user interface during intervention sessions.
Results
Most participants demonstrated safe posture for the majority of postural variables during the information phases. Therefore, we display results only for postures that we exposed to the intervention.
Figure 2 depicts results for the 3 participants exposed to the intervention for head–neck position. Mean safe head–neck position was low for all 3 participants during the information phase (Ms = 4%, 22%, and 9% for Participants 1, 2, and 3, respectively) and increased during the self-monitoring intervention (Ms = 98%, 96%, and 78% for Participants 1, 2, and 3, respectively). During Session 19, Participant 3 did not receive feedback due to a software malfunction, but the self-monitoring response browser window was still available during that session.
Figure 2.
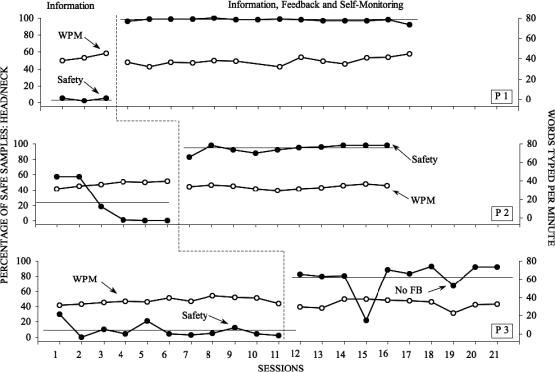
Safety performance and productivity across sessions for participants exposed to the intervention for head–neck posture.
Figure 3 depicts results for the 3 participants exposed to the intervention for back position. Mean safe back position was low for all 3 participants during the information phase (Ms = 18%, 2%, and 36% for Participants 4, 5, and 6, respectively). Mean safe back position increased for Participant 4 during the self-monitoring intervention (M = 94%) and remained high during a reversal to information (M = 96%) and during a follow-up session conducted 3 weeks following the last reversal phase (M = 98%). Mean safe back position increased initially but then decreased for Participants 5 and 6 during the self-monitoring intervention (Ms = 45% and 52% for Participants 5 and 6, respectively).
Figure 3.

Safety performance and productivity across sessions for participants exposed to the intervention for back posture.
Figures 4 and 5 are sample pictures of 1 participant who was exposed to the intervention for back posture (red lines have been added as a visual aid). Figure 4 was captured during the information phase and depicts at-risk posture, whereas Figure 5 depicts safe posture during an intervention session.
Figure 4.

Sample of at-risk back posture of a participant exposed to the intervention for back posture.
Figure 5.

Sample of safe back posture of a participant exposed to the intervention for back posture.
Figure 6 depicts results for 2 of the participants exposed to the intervention for arm position. Mean safe arm position was low for both participants during the information phase (Ms = 0% and 16% for Participants 7 and 8, respectively) and increased during the self-monitoring intervention (Ms = 97% and 97% for Participants 7 and 8, respectively). The final session for Participant 8 involved a reversal to the information phase, which yielded a safety percentage of 100%. We also exposed Participant 3 to the intervention for arms, but because she was exposed to the intervention for head–neck before arms, her data are not included on Figure 6. Mean safe performance for arms for Participant 3 was 70% during information and 39% during the self-monitoring intervention.
Figure 6.
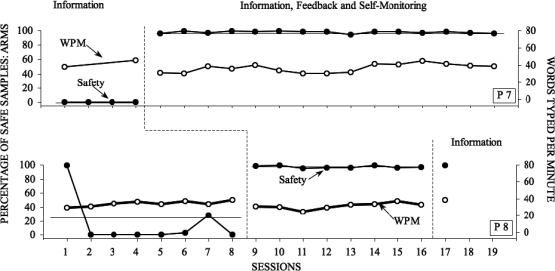
Safety performance and productivity across sessions for participants exposed to the intervention for arm posture.
Productivity decreased by a mean of 11% following the introduction of the intervention. Overall, mean self-monitoring accuracy was 74% across all participants during the course of the study. Participants self-monitored five of nine targeted postures with over 70% accuracy (Participant 1: head–neck, Participant 2: head–neck, Participant 3: head–neck, Participant 4: back, Participant 7: arms, and Participant 8: arms), and all of those five postures improved considerably during intervention. Three postural variables were self-monitored with 40% to 54% accuracy and failed to respond consistently to the intervention (Participant 3: arms, Participant 5: back, and Participant 6: back).
Discussion
The current study is the first organizational behavior management lone-worker study that focuses on real-time visual feedback as a source of self-monitoring data and repeated self-monitoring opportunities delivered through a computer, thus representing the application of a new technology to the problem of MSDs resulting from computer work. Overall, the intervention, consisting of real-time visual feedback and self-monitoring, was effective in improving safety performance for almost all targeted behaviors. Results were most consistent for head–neck and arm outcomes and less consistent for back posture. Participants who were exposed to a withdrawal phase did not revert to preintervention safety levels following the removal of the intervention.
The current study replicates the findings of McCann and Sulzer-Azaroff (1996), in that participants for whom we used a self-monitoring intervention for safe arm and head–neck posture showed high levels of increases in safe posture following intervention. However, the participants in the current study did not show sustained increases in levels of safe back posture. It is not clear if adding components to treatment (e.g., rewards) as in the McCann and Sulzer-Azaroff study would have further improved levels of safe back posture.
Overall the current study appears to have resulted in larger percentage-point changes than earlier safety studies that used self-monitoring (Hickman & Geller, 2003a, 2003b; Olson & Austin, 2001), with the possible exception of McCann and Sulzer-Azaroff (1996). Earlier studies have required participants to self-monitor behavior after the fact, which is in effect a one-time verbal report of events that take place over temporally extended periods. Whether the comparatively large and consistent improvements for head–neck and arm postures observed in the current study can be accounted for by the fact that self-monitoring occurred frequently and at the same time as participants were engaging in the behavior to be self-monitored, as opposed to a one-time verbal report after the fact, remains to be resolved by future studies. Participants in this study were also provided with external stimuli in the form of visual feedback to facilitate the discriminative aspect of self-monitoring, as opposed to participants in the McCann and Sulzer-Azaroff (1996) study who were shown only still pictures of models depicting safe and at-risk postures during discrimination training.
The intervention in the present study may have been effective because it functioned to enable participants to discriminate between kinesthetic stimuli associated with safe and at-risk posture, and those kinesthetic stimuli then came to exert control over postural behavior (Agnew & Snyder, 2002). The potential motivational variables that functioned to make safe kinesthetic stimuli more reinforcing than at-risk kinesthetic stimuli may include increased comfort associated with safe posture or rule statements (e.g., “If I am safe, I will be complying with what the experimenter is expecting from me” or “I will be a good participant if I am in a safe posture”). Because most participants' posture improved immediately following the onset of the intervention, it is likely that rule statements contributed to the improvements in posture observed in this study. It is also possible that once participants had acquired reliable discriminations of their own posture, feedback and self-monitoring episodes may have functioned to prompt participants to adjust their posture.
One limitation of the current study is the nonconcurrent multiple baseline design, which is in effect a series of AB replications. Use of alternative designs (e.g., multiple baseline across behaviors) would have strengthened the demonstration of functional control. However, one control that the nonconcurrent multiple baseline design does provide is that some type of maturation as a result of prolonged exposure to the conditions of the experiment can be eliminated as a potential confounding effect. The fact that posture improved when, and only when, the intervention was introduced for 7 of the 8 participants suggests that a degree of experimental control was achieved.
A second limitation of the study is that postural behavior failed to reverse following the removal of the intervention for 2 participants, which suggests that some confounding factor may have contributed to the observed improvements in posture for these 2 participants. An alternative explanation may be that participants acquired accurate discriminations of kinesthetic stimuli during the intervention, and that other environmental variables (e.g., rule statements) maintained safe postural behavior in the absence of the intervention. Future research might address this issue by altering the characteristics in the experimental environment that communicate the aim of the study (e.g., using a hidden camera).
A third limitation of the study is that introduction of the intervention package was associated with a mean decrease in productivity of 11%, which would probably not be acceptable in any workplace. This decrease in productivity was perhaps to be expected, because work was interrupted approximately every 55 s. Reducing the frequency of self-monitoring while simultaneously achieving improvements in posture is an important area of future research.
Future research should also be aimed at investigating the relative contributions of the components of this package intervention. The treatment package in the current study involved discrimination training, feedback, self-monitoring of posture, and the appearance of feedback and self-monitoring browser windows. The effects of these components can be analyzed individually or in different combinations to determine which of the intervention components are necessary to achieve change in safe posture.
Future applications of the intervention also should involve VDT workers in actual office settings. A relatively inexpensive Web camera could be used to collect data and serve as a source for feedback in office settings, and workers could be trained to visually discriminate between safe and at-risk posture with low costs to organizations. The biggest challenge in extending this technology to the workplace will most likely involve workers' lack of motivation to attend to visual feedback and to engage in self-monitoring repeatedly over extended periods of time, a task that is an inherent distracter from work. If motivational variables are addressed in future studies in applied settings, the consistent and long-lasting improvements observed in the current study can perhaps be replicated outside the laboratory and progress could be made in battling the prevalence of MSDs among computer workers.
References
- Agnew J.L, Snyder G. Removing obstacles to safety: A behavior-based approach. Tucker, GA: Performance Management Publications; 2002. [Google Scholar]
- Detisov O. Eden Prairie, MN: RegSoft; 2005. Willing webcam (Version 2.6) [Computer software]. [Google Scholar]
- Gerr F, Marcus M, Monteilh C. Epidemiology of musculoskeletal disorders among computer users: Lesson learned from the role of posture and keyboard use. Journal of Electromyography and Kinesiology. 2004;14:25–31. doi: 10.1016/j.jelekin.2003.09.014. [DOI] [PubMed] [Google Scholar]
- Hickman J.S, Geller E.S. A safety self-management intervention for mining operations. Journal of Safety Research. 2003a;34:299–308. doi: 10.1016/s0022-4375(03)00032-x. [DOI] [PubMed] [Google Scholar]
- Hickman J.S, Geller E.S. Self-management to increase safe driving among short-haul truck drivers. Journal of Organizational Behavior Management. 2003b;23((4)):1–20. [Google Scholar]
- Kroemer K.H.E, Grandjean E. Fitting the task to the human: A textbook of occupational ergonomics (5th ed.) Bristol, PA: Taylor & Francis; 1997. [Google Scholar]
- Matias A.C, Salvendy G, Kuczek T. Predictive models of carpal tunnel syndrome causation among VDT operators. Ergonomics. 1998;41:213–226. doi: 10.1080/001401398187260. [DOI] [PubMed] [Google Scholar]
- McCann K.B, Sulzer-Azaroff B. Cumulative trauma disorders: Behavioral injury prevention at work. Journal of Applied Behavioral Science. 1996;32((3)):277–291. [Google Scholar]
- McSween T.E. The values-based safety process: Improving your safety culture with a behavioral approach (2nd ed.) New York: Van Nostrand Reinhold; 2003. [Google Scholar]
- Occupational Safety and Health Administration. Computer workstations eTool-checklist. 2004a Retrieved December 8, 2004, from http://www.osha.gov/SLTC/etools/computerworkstations/checklist.html.
- Occupational Safety and Health Administration. Ergonomics programs: Preventing musculoskeletal disorders. 2004b Retrieved December 8, 2004, from http://www.osha.gov/pls/oshaweb/owadisp.show_documentp_tableUNIFIED_AGENDAp_id4167.
- Olson R, Austin J. Behavior-based safety and working alone: The effects of a self-monitoring package on safe performance of bus operators. Journal of Organizational Behavior Management. 2001;21((3)):5–43. [Google Scholar]
- OrangeWare Corporation. Anaheim Hills, CA: Author; 2005. WebcamDV (Version 2.1). [Computer software]. [Google Scholar]
- Reber R.A, Wallin J.A, Chhokar J.S. Reducing industrial accidents: A behavioral experiment. Industrial Relations. 1984;23:119–125. [Google Scholar]
- Van Houten R, Van Houten J, Malenfant J.E.L. Impact of a comprehensive safety program on bicycle helmet use among middle-school children. Journal of Applied Behavior Analysis. 2007;40:239–247. doi: 10.1901/jaba.2007.62-06. [DOI] [PMC free article] [PubMed] [Google Scholar]