

Abstract
The relations between couples’ marital quality and dieting behavior were examined. One-hundred eighty-seven married couples’ dieting behaviors, marital quality, body mass index, weight concerns, depression, and self-esteem were assessed. Results indicate that the relation between healthy dieting behaviors and marital quality is similar for both husbands and wives. However, among wives, marital discord predicted unhealthy dieting behaviors, even after wives’ body mass index, weight concerns, self-esteem, and depression were controlled for. Furthermore, wives’ self-esteem interacted with marital quality when predicting unhealthy dieting. These findings suggest gender differences in the relations between marital quality and dieting behaviors and are consistent with previous research suggesting that men and women have differential response patterns to marital disharmony, with women tending to internalize negative affect experienced in their marriage.
Social support is an important contributor to psychological and physical health. In particular, supportive, close relationships are believed to be conducive to positive health outcomes (House, Landis, & Umberson, 1988). Relationships with significant others have been found to be associated with better health, with consistently married individuals tending to have better health and live longer than unmarried individuals (Brown & Harris, 1978; Burman & Margolin, 1992; Costello, 1982; Tucker, Friedman, Wingard, & Schwartz, 1996). The quality of marital relationships has also been shown to be an important determinant of well-being among both men and women, with negative marital interactions potentially being associated with poor physical and psychological health outcomes (Horowitz, McLaughlin, & White, 1998).
Recent evidence suggests that although marriage can be a positive influence on health, it may be differentially influential in specific health domains (Hope, Rodgers, & Power, 1999). In other words, harmonious marital relations may be conducive to health promotion, whereas conflict-ridden marital relations may be anxiety producing and detrimental to elements of couples’ psychological and physical health (Minuchin, 1985, 1988). However, empirical research exploring the relations between marital quality and couples’ specific health outcomes is limited. In the present study we evaluate the association between health and qualities of married couples’ relationships in one particularly salient health domain: dieting behaviors.
Although a number of studies have evaluated parents’ role in their children’s development of health behaviors (see Tinsley, 1992; Tinsley, Markey, Ericksen, Kwasman, & Ortiz, in press), and eating and dieting behaviors in particular (Davison, Markey, & Birch, 2000; Pike & Rodin, 1991), no empirical investigations of the association between marital constructs and couples’ weight control strategies are available. However, research indicating a link between an individual’s perceived social support and health suggests the need to explore the relations between married partners’ dieting behaviors and marital quality (House et al., 1988). Understanding the links between marital quality and dieting behaviors among married couples is especially important in light of the epidemic rates of unhealthy weight regulation strategies adopted by many women today and the increased prevalence of obesity among both men and women in the United States (Hill & Peters, 1998).
Trends in Dieting Behaviors
A majority of the U.S. adult population engages in dieting behaviors (i.e., food restriction) on a daily basis. In particular, 70–90% of women report being on a diet at any given time (Serdula et al., 1993). This trend is especially problematic due to the health-compromising weight-loss strategies used by many individuals who are trying to lose weight (e.g., purging, fasting, and the use of diuretics; Brownell & Rodin, 1994; Goodrick, Poston, & Foreyt, 1996). It has even been suggested that approximately half of all chronic dieters engage in dieting behaviors at one point in their life that border on clinical eating disorders (Graber, Brooks-Gunn, Paikoff, & Warren, 1994). Further, among dieting individuals, a startling proportion are of normal weight or are underweight by medical standards and do not need to lose weight (Neumark-Sztainer, Sherwood, French, & Jeffery, 1999). Consequently, although the regulation of food intake for weight management (i.e., dieting) is not inherently unhealthy, many individuals risk compromising their health when they diet.
Explanations for the prevalence of dieting include societies’ emphasis on thinness as an integral part of physical attractiveness (Gordon & Tobias, 1984) and rising secular trends in overweight and obesity that may encourage dieting behaviors (Flegal, Carroll, Kuczmarski, & Johnson, 1998). Additionally, several intrapersonal constructs have been substantiated as predictors of dieting behaviors. Among these are an individual’s body size and degree of concern reported about their weight. Researchers have demonstrated a positive relation between body size and dieting behaviors with heavier individuals of all ages (from children to adults) tending to diet more often (Birch & Fisher, 1998; Davison et al., 2000).1 Further, concerns about weight, regardless of objective weight status, have been substantiated as reliable predictors of dieting behaviors, at least among females (Killen et al., 1994).2
Personality characteristics also appear to be related to eating and dieting behaviors (Rotenberg & Flood, 1999). Personality dimensions associated with risk for unhealthy eating behaviors include depressive symptoms, low self-esteem, and feelings of personal ineffectiveness (Gendall, Joyce, Sullivan, & Bulik, 1998; Leon, Fulkerson, Perry, & Cudeck, 1993). Further, the effective treatment of clinical eating disorders with antidepressants suggests, at the very least, comorbidity between depression and the maintenance of unhealthy eating behaviors (Advokat & Kutlesic, 1995).
Thus, although intrapersonal predictors (e.g., body mass index [BMI], weight concerns, personality constructs) of dieting behaviors have been identified, a small body of literature additionally suggests the importance of examining the influence of individuals’ social environments on dieting behaviors. It has been posited that in order to understand Western cultures’ current obsession with weight regulation, the impact of proximal, intimate (e.g., familial) relationships need to be explored (Minuchin, Rosman, & Baker, 1978).
Relationships and Dieting Behaviors
Although no prior empirical studies have explicitly investigated the associations between marital quality and dieting, other literature provides information about interpersonal relationships and dieting behaviors. For example, men and women in romantic relationships appear to influence their partners’ concerns about their weight. In particular, men appear to influence their romantic partners’ weight concerns by placing a great deal of importance on women’s body size and shape when instigating romantic relationships (Smith, Waldorf, & Trembath, 1990). Research further suggests that men are less likely than women to adjust their own eating behaviors or feelings about their bodies in accordance with their female partners’ preferences (Tanteleff-Dunn & Thompson, 1995). Interpersonal relationships have been discussed as promoting disordered eating patterns among female adolescents, with discordant relationships influencing the onset and maintenance of disordered eating (Humphrey, 1989).
Systems theorists (i.e., Minuchin et al., 1978) have demonstrated the importance of investigating individuals’ disordered eating behaviors in the context of familial relationships. In particular, young women with eating disturbances tend to report experiencing less satisfying family relationships (Garfinkel et al., 1983; Humphrey, 1986). Young women suffering from clinical eating disorders report perceiving their families as rigid and disengaged (Humphrey, 1987; Waller, Slade, & Calam, 1990). Additionally, researchers have found that eating disorders emerge when an individual fails to individuate from enmeshed and overprotective family influences (Kog & Vandereycken, 1985) or experiences disorganized, inexpressive, and conflictual family environments (Humphrey, 1986, 1989; Wonderlich, 1992). Overall, research addressing interpersonal influences associated with unhealthy eating behaviors most commonly examine dysfunctional eating in terms of female adolescents’ relationships with parents, oftentimes with a focus on clinical eating outcomes. In the present study, we intend to build on this research addressing the link between interpersonal relationships and eating-related behaviors by focusing on the relation between husbands’ and wives’ marital quality and their dieting behaviors.
Aims of the Present Study
In light of research suggesting the positive relation between marital quality and health, in the present study we seek to determine interpersonal predictors of dieting practices among married couples. To ascertain the extent to which various dimensions of marital relationships uniquely contribute to dieting behaviors, a number of related constructs will be considered as well. These additional constructs consist of the previously identified predictors of dieting behaviors reviewed above and include BMI, weight concerns, depression, and self-esteem.
The objectives of this study are threefold. First, previously identified intrapersonal influences on dieting behaviors (BMI, weight concerns, depression, and self-esteem) and various qualities of the marital relationship (love, harmony, understanding, and overall marital quality) will be used to predict healthy and unhealthy dieting behaviors among married couples. Second, in light of previous research detailing the role of the marital relationship in partners’ health outcomes, in this study we seek to examine the unique explanatory power of marital quality in predicting both healthy and unhealthy dieting practices. Finally, potential interactions between intrapersonal influences on dieting behaviors and marital qualities will be investigated.
Because research suggests a relation between social support (i.e., marriage) and positive health outcomes, it is hypothesized that husbands and wives who report higher levels of marital quality will report less frequent use of unhealthy dieting strategies. Further, marital quality is expected to explain unique variance in predicting husbands’ and wives’ dieting practices. Analyses investigating possible interactions between BMI, weight concerns, depression, self-esteem, and marital quality in predicting dieting behaviors are exploratory.
Method
Participants
Participants were 187 married couples recruited from the Eastern United States as part of a larger longitudinal study.3 The women’s mean age was 35 years (range = 24–47) and the men’s mean age was 37 years (range = 26–66). All participants in this study were Euro-Americans. Two thirds of the participants reported a level of education greater than a high school diploma, and approximately equal proportions of families reported annual incomes below $35,000, between $35,000 and $50,000, and above $50,000.
Measures
Intrapersonal Variables
Weight status
Men’s and women’s weight status was operationalized using BMI scores (weight [kg]/ heighs [m]). On the basis of the recommendations of Lohman, Roche, and Martorell (1988), three height and weight measurements were collected for each participant by trained research assistants, and each individual’s average weight and height were used to calculate their BMI.
Weight concerns
Weight concerns were assessed using an amended version of the Weight Concern Scale (Killen et al., 1994). The Weight Concern Scale was designed to assess current fear of weight gain, importance of weight, perceived fatness, and worry about weight and body shape. In the original Weight Concern Scale, Question 3 read “When was the last time you went on a diet?” This question was changed for use in the present study to “Have you ever gone on a diet?” with response options 1 (never), 2 (I have gone on a diet once before) and 3 (/ have gone on a diet more than once before). This change was made based on the results of pilot data assessing the frequency of dieting among middle-aged women and allows for a more valid assessment of adults’ dieting behaviors among individuals who do not diet. In the present study, Cronbach’s alphas of this measure for women and men were 0.82 and 0.75, respectively.
Depression
The Center for Epidemiological Studies Depression Scale (CES-D) is a 20-item self-report questionnaire designed to measure depressive symptoms among adults in nonclinical populations, with a focus on depressed mood (Radloff, 1977). Cronbach’s alphas in this study were .89 for women and .87 for men.
Self-esteem
The Self-Esteem Scale (SES) is a 10-item scale designed to assess the degree to which individuals feel they are persons of worth and possess positive qualities (Rosenberg, 1979). Cronbach’s reliabilities for men and women in this sample were 0.88 and .079, respectively.
Interpersonal Variables (Marital Quality)
Love and harmony
Marital love and harmony was assessed via the Marital Interactions Questionnaire (Braiker & Kelley, 1979). The Love scale consists of 10 items and reflects the sense of belonging, love, and attachment an individual perceives in their marriage and includes items such as “How committed do you feel toward your partner?” The Cronbach’s alphas for the Love scale in the present study were 0.94 for women and 0.90 for men. The Harmony scale is composed of 5 items measuring behavioral conflict and communication of negative affect within a marriage and contains items such as “How often do you and your partner argue with one another?” The reliabilities for the Harmony scale for women and men in this study were 0.80 and 0.79, respectively.
Understanding
Each participant’s perception of understanding of their spouse was assessed with the Perspective Taking Scale (Understanding of Spouse) of the Marital Experiences Questionnaire (Stets, 1993, 1995). This 4-item scale was designed to assess an individual’s sense of understanding their spouse and includes items such as “I understand my spouse” and “I understand my spouse’s feelings quite well.” The reliabilities of this scale for women and men in this study were 0.77 and 0.69, respectively. Additionally, each participant’s belief that their spouse understands them was assessed by replacing the pronoun “I” with “he/she” in each of the original four items (e.g., “I understand my spouse” was changed to “He/ she understands me”). The reliabilities for this Understanding From Spouse Scale were 0.83 for women and 0.73 for men.
Overall marital quality
Principal-components analysis of the four marital scales (Love, Harmony, Understanding of Spouse, and Understanding From Spouse) used in this study revealed a single factor as indicated by a first to second eigenvalue ratio of 2.54 to 0.73. As suggested by methodologists (e.g., Cohen & Cohen, 1983), because it appears that these scales define a common factor, they were combined to create a measure of overall marital quality. This new index was computed by standardizing each of the four marital scales separately for men and women and averaging these scores within each participant. The resulting measure of overall marital quality had moderate to high internal reliability, with Cronbach’s alphas of 0.86 for women and 0.74 for men.
Healthy and Unhealthy Dieting Behaviors
Participants’ dieting behaviors were assessed using the Weight Control Behaviors Scale (WCBS). The WCBS is a 24-item checklist of various weight loss behaviors that contains two subscales: Healthy Dieting Behaviors and Unhealthy Dieting Behaviors (French, Perry, Leon, & Fulkerson, 1995). Participants were specifically asked to indicate whether they “never, sometimes, or always use [different strategies listed] as an adult to try to lose weight.” The Healthy Dieting Behaviors subscale in this measure assesses behaviors including “eat more fruit and vegetables” and “eliminate snacking.” Approximately 92% of the women and 75% of the men in this sample reported using some type of healthy dieting behavior. Cronbach’s alphas for this subscale were 0.92 for women and 0.95 for men. Items on the unhealthy dieting behaviors subscale include items indicating participants’ use of strategies such as “diet pills” and “vomiting.” Approximately 62% of the women and 49% of the men in this sample reported using some type of unhealthy dieting behavior. Cronbach’s alphas for the Unhealthy Dieting Behaviors subscale were .71 for women and .56 for men.
Procedure
All participants were recruited as part of a larger study of familial health. Husbands and wives completed the questionnaires used in this study during their scheduled visits to the laboratory. Upon completion of all questionnaires, a trained research assistant measured the husbands’ and wives’ height and weight. Written consent was obtained prior to participation in this study, and participants were financially compensated for their efforts upon completion of all components of the study.
Results
Table 1 displays the descriptive statistics for both the intrapersonal and marital constructs considered in the analyses. On the basis of criteria outlined by the World Health Organization (1998), the rate of overweight among women in this sample was slightly higher than population-level trends, whereas the rate of obesity was slightly lower. For men, both rates of overweight and obesity were somewhat higher than population trends.4 Additionally, dependent t tests revealed that wives had lower BMIs, t(186) = 4.92, p < .01, reported more marital harmony, t(186) = 2.96, p < .01, more weight concerns, t(186) = 6.90, p < .01, and more healthy dieting behaviors, t(186) = 6.29, p < .01, and unhealthy dieting behaviors, t(186) = 4.39, p < .01, than husbands. Correlational analyses presented in Table 1 demonstrated that husbands’ and wives’ BMIs were positively related, and there was considerable agreement between husbands and wives across all marital variables. Table 2 displays the relations among all intrapersonal and marital constructs for both husbands and wives.
Table 1.
Descriptive Statistics for Intrapersonal and Marital Constructs
| Wife
|
Husband
|
||||
|---|---|---|---|---|---|
| Scale | M | SD | M | SD | r |
| Healthy Diet | 11.87 | 5.53 | 7.98 | 6.41 | .01 |
| Unhealthy Diet | 1.66 | 1.92 | 0.89 | 1.28 | −.14 |
| Body Mass Index | 25.85 | 5.56 | 28.08 | 4.48 | .25* |
| Weight Concerns | 1.59 | 0.75 | 1.07 | 0.68 | −.04 |
| Depression | 9.56 | 7.50 | 9.65 | 7.34 | .06 |
| Self-Esteem | 33.12 | 4.51 | 33.67 | 4.41 | .11 |
| Overall Marital Quality | 0.00 | 0.88 | 0.00 | 0.69 | .51* |
| Harmony | 21.06 | 6.90 | 19.33 | 6.70 | .31* |
| Love | 75.26 | 13.48 | 75.48 | 10.48 | .25* |
| Understanding of Spouse | 14.17 | 2.49 | 13.83 | 2.38 | .40* |
| Understanding From Spouse | 13.39 | 2.96 | 13.42 | 2.46 | .41* |
Note, n = 187 for both wives and husbands. Values in bold indicate a significant difference between husbands’ and wives’ scores.
p < .05.
Table 2.
Correlations Between Intrapersonal and Marital Constructs for Husbands and Wives
| Scale | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Body Mass Index | — | .36* | .09 | −.15* | −.16* | −.14* | −.10 | −.09 | −.21* |
| 2. Weight Concerns | .37* | — | .21* | −.28* | −.13 | −.13 | −.10 | −.08 | −.12 |
| 3. Depression | .11 | −.06 | — | −.52* | −.34* | −.33* | −.15* | −.31* | −.35* |
| 4. Self-Esteem | .05 | .09 | −.42* | — | .26* | .23* | .11 | .22* | .29* |
| 5. Marital Quality | −.10 | .10 | −.29* | .30* | — | .81* | .78* | .86* | .87* |
| 6. Harmony | −.14 | .00 | −.18* | .19* | .70* | — | .51* | .62* | .58* |
| 7. Love | −.08 | .07 | −.22* | .27* | .69* | .48* | — | .52* | .57* |
| 8. Understanding of Spouse | −.05 | .09 | −.23* | .19* | .77* | .29* | .25* | — | .76* |
| 9. Understanding From Spouse | −.03 | .15* | −.22* | .24* | .81* | .31* | .35* | .80* | — |
Note. Wives’ correlations are presented above the diagonal; husbands’ correlations are presented below the diagonal, df = 185.
p < .05.
Predicting Healthy and Unhealthy Dieting Behaviors
Next, analyses were done to examine how each intrapersonal and marital variable was related to healthy and unhealthy dieting for both husbands and wives. Table 3 displays the Pearson product-moment coefficients for husbands’ and wives’ healthy and unhealthy dieting behaviors with each intrapersonal and marital construct. BMI and weight concerns tended to be related to more healthy dieting behaviors for both wives and husbands. However, similar patterns did not emerge between husbands and wives for unhealthy dieting behaviors. For husbands, none of the marital or intrapersonal constructs significantly predicted unhealthy dieting. However, among wives, unhealthy dieting was related to high BMI, weight concerns, depression, and low self-esteem. Additionally, as was hypothesized, wives’ unhealthy dieting was related to poor overall marital quality, a lack of marital harmony, love, little understanding of their spouse, and the perception of little understanding from their spouse.
Table 3.
Correlations Between Healthy and Unhealthy Dieting and Intrapersonal and Marital Constructs
| Healthy dieting
|
Unhealthy dieting
|
|||||||
|---|---|---|---|---|---|---|---|---|
| Scale | Wife | Husband | q | ZPF | Wife | Husband | q | ZPF |
| Body Mass Index | .26* | .15* | .12 | 1.10 | .21* | .13 | .08 | 0.75 |
| Weight Concerns | .56* | .20* | .43 | 4.23* | .43* | .13 | .33 | 3.19* |
| Depression | .11 | .07 | .04 | 0.39 | .30* | .06 | .25 | 2.40* |
| Self-Esteem | −.11 | .08 | −.19 | − 1.78 | −.30* | .12 | −.43 | −4.01* |
| Overall Marital Quality | −.13 | .11 | −.24 | −2.36* | −.28* | .11 | −.40 | −3.71* |
| Harmony | −.12 | −.04 | −.08 | −1.49 | −.18* | .03 | −.22 | −2.02* |
| Love | −.08 | .13 | −.21 | −2.08* | −.20* | .13 | −.33 | −3.23* |
| Understanding of Spouse | −.14 | .09 | −.23 | −2.33* | −.36* | .10 | −.48 | −4.45* |
| Understanding From Spouse | −.11 | .06 | −.17 | −1.56 | −.20* | .06 | −.26 | −2.45* |
Note. Values given under Wife and Husband are correlation coefficients. Cohen’s q is used as an effect size index of wives’ r – husbands’ r. The Z-transformed Pearson-Filon statistic (ZPF) is given to determine the significant difference between these correlations, n = 187 for both wives and husbands.
p < .05.
Next, the data were used to examine whether the measured intrapersonal and marital variables predicted healthy and unhealthy dieting differently for husbands and wives. Cohen’s q (Cohen, 1988) was calculated to assess the effect size of the differences between the correlations for husbands and wives. It should be noted that because participants in this study were married, the correlations of husbands and wives are related, but nonoverlapping. Because of this dependency, the Z-transformed Pearson-Filon statistic (ZPF) was used to determine the significance of these differences (Raghunathan, Rosenthal, & Rubin, 1996, page 179, Equation 3). As can be seen in Table 3, four of the correlations for healthy dieting were significantly different for husbands and wives, with small differences for overall marital quality, love, and understanding of spouse, and moderate differences for weight concerns. However, for unhealthy dieting all of the correlations, except BMI, were significantly different for husbands and wives, with small differences for depression, harmony, and understanding from spouse, and moderate differences for weight concerns, self-esteem, overall marital quality, love, and understanding of spouse.5
Unique Contributions of Intrapersonal Constructs and Overall Marital Quality
Because all marital variables tended to be related to dieting behaviors similarly, and because of the high relationship discussed previously between the marital scales (see the Method section), to simplify further analysis we will use only the marital variable of overall marital quality. The amount of unique variance in healthy and unhealthy dieting behaviors explained by the predictor variables of BMI, weight concerns, depression, self-esteem, and overall marital quality were next examined. For both husbands and wives, simultaneous regression analyses were conducted separately for healthy and unhealthy dieting behaviors. All predictor variables were centered for husbands and wives. The resulting beta weights provide insight into the relative contribution of each predictor variable. As predicted, weight concerns consistently added unique variance when predicting husbands’ and wives’ healthy dieting behaviors, as well as wives’ unhealthy dieting behaviors (see Table 4 and Table 5). Overall marital quality also contributed to the prediction of unhealthy dieting in wives above the variance explained by all other variables.
Table 4.
Simultaneous Regression Analyses Predicting Healthy Dieting Behaviors
| Healthy Dieting | B | SE B | β |
|---|---|---|---|
| Husbands | |||
| Body Mass Index | 0.12 | 0.11 | .08 |
| Weight Concerns | 1.43 | 0.74 | .16* |
| Depression | 0.12 | 0.07 | .13 |
| Self-Esteem | 0.12 | 0.11 | .08 |
| Overall Marital Quality | 1.06 | 0.71 | .12 |
| Wives | |||
| Body Mass Index | 0.06 | 0.07 | .06 |
| Weight Concerns | 4.10 | 0.50 | .55* |
| Depression | 0.00 | 0.05 | .00 |
| Self-Esteem | 0.09 | 0.09 | .08 |
| Overall Marital Quality | −0.43 | 0.41 | −.07 |
Note. n = 187 for both husbands and wives. Husbands’ R2 = .07 (p < .05); wives’ R2 = .32 (p < .05).
p < .05.
Table 5.
Simultaneous Regression Analyses Predicting Unhealthy Dieting Behaviors
| Unhealthy Dieting | B | SE B | β |
|---|---|---|---|
| Husbands | |||
| Body Mass Index | 0.03 | 0.02 | .09 |
| Weight Concerns | 0.15 | 0.15 | .07 |
| Depression | 0.03 | 0.01 | .15 |
| Self-Esteem | 0.03 | 0.02 | .13 |
| Overall Marital Quality | 0.20 | 0.14 | .11 |
| Wives | |||
| Body Mass Index | 0.02 | −0.02 | .03 |
| Weight Concerns | 0.89 | 0.18 | .34* |
| Depression | 0.03 | 0.02 | .12 |
| Self-Esteem | −0.04 | 0.03 | −.08 |
| Overall Marital Quality | −0.37 | 0.15 | −.17* |
Note. n = 187 for both husbands and wives. Husbands’ R2 = .06 (p < .05); wives’ R2 = .26 (p < .05).
p < .05.
Interactions Between Marital Quality and Intrapersonal Variables
In the previous analyses, poor marital quality was demonstrated to have a negative and unique impact on unhealthy dieting in wives. Additional regression analyses were next conducted in order to determine whether any intrapersonal variables (BMI, weight concerns, depression, and self-esteem) interacted with marital quality when predicting unhealthy dieting among husbands and wives. Of the eight analyses conducted, only self-esteem produced a significant interaction with overall marital quality in predicting wives’ unhealthy dieting, F(1, 183) = 5.24, p < .05. Figure 1 presents a graphic representation of this interaction by calculating simple regression equations corresponding to individuals scoring at the mean, one standard deviation above the mean, and one standard deviation below the mean of self-esteem (Aiken & West, 1991). As the figure indicates, there was a negative relationship between marital quality and unhealthy dieting when wives had low self-esteem and essentially no relationship between marital quality and unhealthy dieting when wives had high self-esteem.
Figure 1.
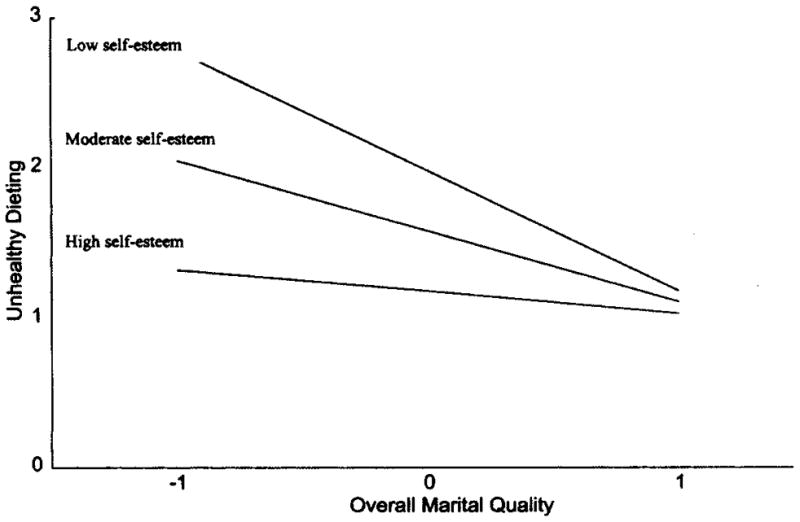
A graphic representation of the regression equation Unhealthy Diet = 1.58 – 0.47 (Marriage) –0.09 (Self-Esteem) + 0.08 (Marriage × Self-Esteem), for wives scoring at the mean, one standard deviation above the mean, and one standard deviation below the mean on self-esteem.
Discussion
In light of previous research (Burman & Margolin, 1992; Tucker et al., 1996) suggesting the integral role marriage has on couples’ health, the objectives of the present study were to identify interpersonal predictors of healthy and unhealthy dieting behaviors among married couples while considering previously recognized predictors of dieting behaviors. Although constructs such as BMI, weight concerns, depression, and self-esteem have previously been discussed in relation to unhealthy eating behaviors (Birch & Fisher, 1998; Rotenberg & Flood, 1999), less attention has been focused on the potential influences of interpersonal constructs, such as marital quality, on dieting strategies. The findings presented in this article suggest the importance of considering associations among intrapersonal variables, marital quality, and dieting behaviors.
The present analyses are in agreement with prior findings suggesting that women tend to be more concerned with their weight than men, as women in this study tended to have higher weight concerns than their husbands, dieted much more than their husbands, and were more likely to utilize both healthy and unhealthy dieting strategies than their husbands (Pliner, Chaiken, & Flett, 1990). Further, these findings suggest relations between husbands’ and wives’ body size and concordance between husbands’ and wives’ perceptions of their marital relationship.
The patterns of relations found between healthy dieting behaviors and marital dimensions were similar for both husbands and wives in this study, with the marital relationship having seemingly little association with healthy dieting behaviors. The previously substantiated predictors of dieting behaviors, weight concerns and BMI, predicted healthy dieting behaviors among both husbands and wives in this study. However, for unhealthy dieting strategies, different associations appear to exist for husbands and wives. That is, although wives’ reports of marital quality were related to their unhealthy dieting behaviors, none of the measures of marital quality predicted husbands’ unhealthy dieting. Further, among women, overall marital quality was significantly associated with unhealthy dieting even after the variance explained by BMI, weight concerns, depression, and self-esteem was removed.
Although we can only speculate about the direction of influence in this study, these findings corroborate previous research that suggests men and women have different response patterns to marital disharmony, with women tending to internalize negative affect experienced in their marriage (Katz & Gottman, 1996). It is possible that a woman’s perception of a lack of love and understanding by her marital partner results in a sense of despair or worthlessness that is exhibited in unhealthy and perhaps even self-punishing dieting behaviors. Although the specific processes relating marital dimensions to dieting behaviors are not decipherable due to the nature of the data available in this study, it seems clear that men’s dieting behaviors are not a result of dissatisfaction with their marriage or of sublimation of negative interpersonal relations with their wives. It is possible, and would be consistent with previous research (Hope, Rodgers, & Power, 1999), that men who did experience disharmonious marriages relied on different coping strategies of a more externalizing nature.
Furthermore, these results indicate an interaction between wives’ self-esteem and their report of marital quality in influencing their unhealthy dieting behaviors. This finding may have occurred because women with high self-esteem are protected from poor marital relations and may deal with negative marital interactions in a more positive manner. Or perhaps positive marital relations protect women with low self-esteem from engaging in unhealthy dieting behaviors. Regardless, these analyses demonstrate the importance of considering marital quality when trying to understand women’s unhealthy dieting practices.
Limitations
Although the present study is to our knowledge the first attempt to investigate the effects of the marital relationship on dieting behaviors, several limitations need to be kept in mind. The first limitation concerns the homogenous, Euro-American sample. Future research endeavors are needed to determine whether these findings are generalizable to all ethnic groups. This study should also be replicated using behavioral, and not just self-report, measures of the marital relationship. Additional research including data from both observational assessments and self-report measures could substantially strengthen our understanding of the relations between marital quality and dieting behaviors. Finally, these results need to be interpreted with caution, as cause cannot be determined on the basis of the correlational nature of the design used. Whereas these analyses have focused on unhealthy dieting behaviors as the outcome of interest, unhealthy dieting behaviors could also be conceptualized as predictors of marital discord. Additional longitudinal research should help to discern the direction of effects between marital quality and dieting behaviors among married couples.
Implications for Application and Public Policy
The present study presents the first attempt to empirically examine the associations between marital quality and dieting. Contrary to traditional conceptualizations of the relation between social support and health that suggest social support is primarily positively related to health outcomes, these findings suggest that the quality of an individual’s interpersonal relationships may determine the extent to which relationships are associated with positive and negative health outcomes. Furthermore, interpersonal relationships, such as a marriage, that are disharmonious may negatively affect individuals’ health as indicated by the relation in this study between wives’ reports of poor marital quality and unhealthy dieting practices.
Although the present study suggests the important association between marital quality and dieting behaviors among women, the negative impact of poor marital relations on dieting behaviors may have consequences for individuals outside of the marital dyad. Of primary importance are couples’ children, who are likely influenced both directly and indirectly by their parents’ marital relationship and related dieting behaviors. Research suggests that happily married couples may not only experience better health, but may be more capable of exhibiting greater investment, sensitivity, and warmth in family interactions than unhappily married coupies (Cowan, Cowan, Sulz, & Heming, 1994; Fincham, 1998; McHale, 1995). Further, relations between parents’ and children’s eating and dieting behaviors have been substantiated (Birch & Fisher, 1998; Davison et al., 2000). Presumably, children are likely to benefit when couples take care to maintain both positive marital relations and health (e.g., dieting) behaviors.
From a public health perspective these findings are informative because of the recognized number of individuals engaging in unhealthy eating behaviors in the United States and increasing efforts aimed at improving nutritional patterns among individuals who are currently overweight and individuals engaging in disordered eating. Clearly, unhealthy nutritional patterns are a result of multifaceted intrapersonal and interpersonal factors. Although therapists have exhibited an increasing recognition of the necessity of including family therapy in treatment programs aimed at ameliorating children’s pathologies (see Minuchin et al., 1978), similar strategies are rarely adopted when attempting to improve the health status of married couples. It is plausible that unhealthy eating habits among married women are in part indicative of marital disharmony, and couples who undergo marital counseling may cultivate both their marital relationship and their health.
Acknowledgments
This research was funded by National Institute of Health Grant RO1 HD 32973 awarded to Leann L. Birch. An earlier version of this article was presented at the 108th Annual Convention of the American Psychological Association, Washington, DC, August 2000. We thank the participating families and many research assistants who made this study possible. Furthermore, we are thankful to Barbara J. Tinsley and Daniel J. Ozer for their helpful comments.
Footnotes
Charlotte N. Markey and Patrick M. Markey, Department of Psychology, University of California, Riverside; Leann L. Birch, Department of Human Development and Family Studies, Pennsylvania State University.
Body size is typically assessed using Body Mass Index = (weight in kg)/(height in m2).
Although little empirical research has examined predictors of men’s weight regulation strategies, there is recent evidence suggesting that patterns of relations among BMI, weight concerns, and dieting among men are similar to patterns corroborated among women (Davison et al., 2000).
All couples participating in this study had 5-year-old daughters (that were their biological children) participating in this study as well. Thus, although detailed information concerning couples’ marital history is unavailable, it is probable that most participating couples had been married for at least 5 years.
On the basis of criteria established by the World Health Organization (1998), men and women were classified as overweight if their BMI ≥ 25 and as obese if their BMI ≥ 30.
It should be noted that when the relations between the marital constructs and unhealthy dieting are corrected for attenuation, the difference in the patterns of relations seen for husbands and wives becomes even more magnified for all the marital variables except marital harmony.
References
- Advokat C, Kutlesic V. Pharmacotherapy of eating disorders: A commentary. Neuroscience and Biobehavioral Reviews. 1995;19(1):59–66. doi: 10.1016/0149-7634(94)00044-2. [DOI] [PubMed] [Google Scholar]
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Thousand Oaks, CA: Sage; 1991. [Google Scholar]
- Birch LL, Fisher JO. Development of eating behaviors among children and adolescents. Pediatrics. 1998;101:539–549. [PubMed] [Google Scholar]
- Braiker HB, Kelley HH. Conflict in the development of close relationships. In: Burgess R, Houston T, editors. Social exchange in developing relationships. New York: Academic Press; 1979. pp. 135–168. [Google Scholar]
- Brown GW, Harris T. Social origins of depression: A study of psychiatric disorder in women. New York: Free Press; 1978. [Google Scholar]
- Brownell KD, Rodin J. The dieting maelstrom: Is it possible and advisable to lose weight? American Psychologist. 1994;49:781–791. doi: 10.1037//0003-066x.49.9.781. [DOI] [PubMed] [Google Scholar]
- Burman B, Margolin G. Analysis of the association between marital relationships and health problems: An interactional perspective. Psychological Bulletin. 1992;112:39–63. doi: 10.1037/0033-2909.112.1.39. [DOI] [PubMed] [Google Scholar]
- Cohen J. Set correlation and contingency tables. Applied Psychological Measurement. 1988;12:425–434. [Google Scholar]
- Cohen J, Cohen P. Applied multiple regression: Correlation analysis for the behavioral sciences. Hillsdale, NJ: Erlbaum; 1983. [Google Scholar]
- Costello CG. Social factors associated with depression: A retrospective community study. Psychological Medicine. 1982;12:329–339. doi: 10.1017/s0033291700046663. [DOI] [PubMed] [Google Scholar]
- Cowan PA, Cowan C, Sulz M, Heming J. Prebirth to preschool family factors predicting children’s adaptation to kindergarten. In: Parke R, Kellman S, editors. Advances in family research. Vol. 4. Hillsdale, NJ: Erlbaum; 1994. pp. 75–114. [Google Scholar]
- Davison KK, Markey CN, Birch LL. Etiology of body dissatisfaction and weight concerns among 5-year-old girls. Appetite. 2000;35(2):143–151. doi: 10.1006/appe.2000.0349. [DOI] [PubMed] [Google Scholar]
- Fincham FD. Child development and marital relations. Child Development. 1998;69:543–574. [PubMed] [Google Scholar]
- Flegal KM, Carroll MD, Kuczmarski RJ, Johnson CL. Overweight and obesity in the United States: Prevalence and trends, 1960–1994. International Journal of Eating Disorders. 1998;22:39–47. doi: 10.1038/sj.ijo.0800541. [DOI] [PubMed] [Google Scholar]
- French SA, Perry CL, Leon GR, Fulkerson JA. Dieting behaviors and weight change history in female adolescents. Health Psychology. 1995;14:548–555. doi: 10.1037//0278-6133.14.6.548. [DOI] [PubMed] [Google Scholar]
- Garfinkel PE, Garner DM, Rose J, Darby PL, Brandes JS, O’Halen J, Walsh N. A comparison of characteristics in the families of patients with anorexia nervosa and normal controls. Psychological Medicine. 1983;13:821–828. doi: 10.1017/s0033291700051539. [DOI] [PubMed] [Google Scholar]
- Gendall KA, Joyce PR, Sullivan PF, Bulik CB. Personality and dimensions of dietary restraint. International Journal of Eating Disorders. 1998;24:371–379. doi: 10.1002/(sici)1098-108x(199812)24:4<371::aid-eat4>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- Goodrick GK, Poston WSC, Foreyt JP. Methods for voluntary weight loss control: Update. The International Journal of Applied and Basic Nutritional Sciences. 1996;12:672–676. doi: 10.1016/s0899-9007(96)00243-2. [DOI] [PubMed] [Google Scholar]
- Gordon JB, Tobias A. Fat, female and the life course: The developmental years. Marriage & Family Review. 1984;7:65–92. [Google Scholar]
- Graber JA, Brooks-Gunn J, Paikoff RL, Warren MP. Prediction of eating problems: An 8-year study of adolescent girls. Developmental Psychology. 1994;30:823–834. [Google Scholar]
- Hill JO, Peters JC. Environmental contributions to the obesity epidemic. Science. 1998 May;280:1371–1374. doi: 10.1126/science.280.5368.1371. [DOI] [PubMed] [Google Scholar]
- Hope S, Rodgers B, Power C. Marital status transitions and psychological distress: Longitudinal evidence from a national population sample. Psychological Medicine. 1999;29:381–389. doi: 10.1017/s0033291798008149. [DOI] [PubMed] [Google Scholar]
- Horowitz AV, McLaughlin J, White HR. How the negative and positive aspects of partner relationships affect the mental health of young married people. Journal of Health & Social Behavior. 1998;39(2):124–136. [PubMed] [Google Scholar]
- House JS, Landis KR, Umberson D. Social relationships and health. Science. 1988 July;241:540–545. doi: 10.1126/science.3399889. [DOI] [PubMed] [Google Scholar]
- Humphrey LL. Family relations in bulimic-anorexic and nondistressed families. International Journal of Eating Disorders. 1986;5(2):223–232. [Google Scholar]
- Humphrey LL. Comparison of bulimicanorexic and nondistressed families using structural analysis of social behavior. Journal of the American Academy of Child & Adolescent Psychiatry. 1987;26(2):248–255. doi: 10.1097/00004583-198703000-00023. [DOI] [PubMed] [Google Scholar]
- Humphrey LL. Observed family interactions among subtypes of eating disorders using structural analysis of social behavior. Journal of Consulting & Clinical Psychology. 1989;57:206–214. doi: 10.1037//0022-006x.57.2.206. [DOI] [PubMed] [Google Scholar]
- Katz LF, Gottman JM. Spillover effects of marital conflict: In search of parenting and co-parenting mechanisms. In: McHale JP, Cowan PA, editors. Understanding how family-level dynamics affect children’s development: Studies of two-parent families. San Francisco, CA: Jossey-Bass; 1996. pp. 57–76. [Google Scholar]
- Killen JD, Taylor CB, Hayward C, Wilson DM, Haydel KF, Hammer LD, Simmonds B, Robinson TN, Lift I, Varady A, Kraemer H. Pursuit of thinness and onset of eating disorder symptoms in a community sample of adolescent girls: A three-year prospective analysis. International Journal of Eating Disorders. 1994;16:227–238. doi: 10.1002/1098-108x(199411)16:3<227::aid-eat2260160303>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- Kog E, Vandereycken W. Family characteristics of anorexia nervosa and bulimia. A review of the research literature. Clinical Psychology Review. 1985;5:159–180. [Google Scholar]
- Leon GR, Fulkerson JA, Perry CL, Cudeck R. Personality and behavioral vulnerabilities associated with risk status for eating disorders in adolescent girls. Journal of Abnormal Psychology. 1993;102:438–444. doi: 10.1037//0021-843x.102.3.438. [DOI] [PubMed] [Google Scholar]
- Lohman TG, Roche AF, Martorell M. Anthropometric standardization reference manual. Champaign, IL: Human Kinetics; 1988. [Google Scholar]
- McHale JP. Coparenting and triadic interactions during infancy: The role of marital distress and child gender. Developmental Psychology. 1995;31:985–996. [Google Scholar]
- Minuchin P. Families and individual development: Provocations from the field of family therapy. Child Development. 1985;56:289–302. [PubMed] [Google Scholar]
- Minuchin P. Relationships within the family: A systems perspective on development. In: Hinde RA, Stevenson-Hinde J, editors. Relationships within families: Mutual influences. Oxford, England: Clareden Press; 1988. pp. 7–26. [Google Scholar]
- Minuchin S, Rosman BL, Baker L. Psychosomatic families: Anorexia nervosa in context. Cambridge, MA: Harvard University Press; 1978. [Google Scholar]
- Neumark-Sztainer D, Sherwood NE, French SA, Jeffery RW. Weight control behaviors among adult men and women: Cause for concern? Obesity Research. 1999;7:672–676. doi: 10.1002/j.1550-8528.1999.tb00700.x. [DOI] [PubMed] [Google Scholar]
- Pike KM, Rodin J. Mothers, daughters, and disordered eating. Journal of Abnormal Psychology. 1991;100:198–204. doi: 10.1037//0021-843x.100.2.198. [DOI] [PubMed] [Google Scholar]
- Pliner P, Chaiken S, Flett GL. Gender differences in concern with body weight and physical appearance over the life span. Personality & Social Psychology Bulletin. 1990;16:263–273. [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Raghunathan TE, Rosenthal R, Rubin DB. Comparing correlated but nonoverlapping correlations. Psychological Methods. 1996;1:178–183. [Google Scholar]
- Rosenberg M. Conceiving the self. New York: Basic Books; 1979. [Google Scholar]
- Rotenberg KJ, Flood D. Loneliness, dysphoria, dietary restraint, and eating behavior. International Journal of Eating Disorders. 1999;25:55–64. doi: 10.1002/(sici)1098-108x(199901)25:1<55::aid-eat7>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- Serdula MK, Collins ME, Williamson DF, Anda RF, Pamuk ER, Byers TE. Weight control practices among U.S. adolescents and adults. Annals of Internal Medicine. 1993;119:667–671. doi: 10.7326/0003-4819-119-7_part_2-199310011-00008. [DOI] [PubMed] [Google Scholar]
- Smith JE, Waldorf VA, Trembath DL. Single white male looking for thin, very attractive …. Sex Roles. 1990;23:675–685. [Google Scholar]
- Stets JE. Control in dating relationships. Journal of Marriage and the Family. 1993;55:673–685. [Google Scholar]
- Stets JE. Modeling control in relationships. Journal of Marriage and the Family. 1995;57:489–501. [Google Scholar]
- Tanteleff-Dunn S, Thompson JK. Romantic partners and body image disturbance: Further evidence for the role of perceived–actual disparities. Sex Roles. 1995;33:589–605. [Google Scholar]
- Tinsley BJ. Multiple influences on the acquisition and socialization of children’s health attitudes and behavior: An integrative review. Child Development. 1992;63:1043–1069. doi: 10.1111/j.1467-8624.1992.tb01680.x. [DOI] [PubMed] [Google Scholar]
- Tinsley BJ, Markey CN, Ericksen AJ, Kwasman A, Ortiz RV. Health promotion for parents. In: Bornstein MH, editor. Handbook of parenting. Hillsdale, NJ: Erlbaum; in press. [Google Scholar]
- Tucker JS, Friedman HS, Wingard DL, Schwartz JE. Marital history at midlife as a predictor of longevity: Alternative explanations to the protective effect of marriage. Health Psychology. 1996;15:94–101. doi: 10.1037//0278-6133.15.2.94. [DOI] [PubMed] [Google Scholar]
- Waller G, Slade P, Calam R. Family adaptability and cohesion: Relation to eating attitudes and disorders. International Journal of Eating Disorders. 1990;9:225–228. [Google Scholar]
- Wonderlich S. Relationship of family and personality factors in bulimia. In: Crowther JH, Tennenbaum DL, Hobfoll E, Stephens MAP, editors. The etiology of bulimia nervosa: The individual and familial context. Washington, DC: Hemisphere; 1992. pp. 103–126. [Google Scholar]
- World Health Organization. Obesity: Preventing and managing the global epidemic; Report of a WHO consultation on obesity; Geneva. June 3–5, 1997; Geneva, Switzerland: Author; 1998. [PubMed] [Google Scholar]