

Abstract
Scoliosis is a spinal deformity consisting of lateral curvature and rotation of the vertebrae. The causes of scoliosis vary and are classified broadly as congenital, neuromuscular, syndrome-related, idiopathic and spinal curvature due to secondary reasons. The majority of scoliosis cases encountered by the general practitioner will be idiopathic. The natural history relates to the etiology and age at presentation, and usually dictates the treatment. However, it is the patient’s history, physical examination and radiographs that are critical in the initial evaluation of scoliosis, and in determining which patients need additional considerations. Scoliosis with a primary diagnosis (nonidiopathic) must be recognized by the physician to identify the causes, which may require intervention. Patients with congenital scoliosis must be evaluated for cardiac and renal abnormalities. School screening for scoliosis is controversial and is falling out of favour. The treatment for idiopathic scoliosis is based on age, curve magnitude and risk of progression, and includes observation, orthotic management and surgical correction with fusion. A child should be referred to a specialist if the curve is greater than 10° in a patient younger than 10 years of age, is greater than 20° in a patient 10 years of age or older, has atypical features or is associated with back pain or neurological abnormalities.
Keywords: Back pain in scoliosis, Idiopathic scoliosis, Nonidiopathic scoliosis, Scoliosis screening
Abstract
La scoliose est une malformation rachidienne constituée d’une courbure latérale et d’une rotation des vertèbres. Les causes de la scoliose sont variables et se divisent généralement en grandes classes : origine congénitale, origine neuromusculaire, reliée à un syndrome, origine idiopathique et courbure rachidienne imputable à des raisons secondaires. La majorité des scolioses qu’observe l’omnipraticien sont d’origine idiopathique. L’évolution naturelle est reliée à l’étiologie et à l’âge au moment de la consultation et, d’ordinaire, elle dicte le traitement. Cependant, l’histoire, l’examen physique et les radiographies du patient sont essentiels pour l’évaluation initiale de la scoliose et pour déterminer quels patients ont besoin d’une évaluation plus poussée. Le médecin doit établir qu’une scoliose se rapporte à un diagnostic primaire (non idiopathique) afin de déceler les causes qui exigent peutêtre une intervention. Il faut évaluer les patients atteints d’une scoliose congénitale afin d’établir s’ils ont des anomalies cardiaques et rénales. Le dépistage de la scoliose en milieu scolaire est controversé et de moins en moins prôné. Le traitement de la scoliose idiopathique dépend de l’âge, de l’importance de la courbure et du risque d’évolution, et il inclut l’observation, le port d’une orthèse et une correction chirurgicale avec fusion. Il faut aiguiller l’enfant de moins de dix ans vers un spécialiste lorsque la courbure est supérieure à 10° et aiguiller celui de dix ans ou plus lorsque la courbure est supérieure à 20°, de même que lorsque les caractéristiques de la scoliose sont atypiques ou que la scoliose s’associe à des douleurs dorsales ou à des anomalies neurologiques.
Scoliosis is defined as a deviation of the normal vertical line of the spine, consisting of a lateral curvature with rotation of the vertebrae within the curve. Typically, for scoliosis to be considered, there should be at least 10° of spinal angulation on the posterior-anterior radiograph associated with vertebral rotation (1). The causes of scoliosis vary and are classified broadly as congenital, neuromuscular, syndrome-related, idiopathic and spinal curvature due to secondary reasons. Congenital scoliosis is due to a vertebral abnormality causing the mechanical deviation of the normal spinal alignment. Scoliosis can be due to neurological conditions (eg, cerebral palsy or paralysis), muscular abnormalities (eg, Duchenne muscular dystrophy) or other syndromes (eg, Marfan syndrome and neurofibromatosis). Occasionally, significant lateral deviation of the spine can occur with little or no rotation of the spine and without bony abnormalities. In these cases, the ‘scoliosis’ can be the result of pain, spinal cord abnormalities, tumours (both intraspinal and extraspinal) and infection. The majority of scoliosis cases encountered by the general practitioner will be without an obvious cause (idiopathic), and will be the main focus of the present review. The natural history relates to the etiology and age at presentation, and usually dictates the treatment. However, it is the patient’s history, physical examination and radiographs that are critical in the initial evaluation of scoliosis and in determining which patients need additional evaluation and consideration.
PATIENT HISTORY
Much of the history and physical examination is focused on identifying nonidiopathic and often more ominous causes of scoliosis (Table 1). Young age at onset (younger than 10 years of age), rapid curve progression and the presence of neurological symptoms are the most useful findings in identifying nonidiopathic scoliosis (1). Fortunately, most frontline physicians will only encounter idiopathic scoliosis during their careers. Perhaps the most important task for the physician, however, is to identify underlying causes that may require intervention.
TABLE 1.
Patient history components
| Age at onset |
| Evidence of maturation |
| Presence of back pain |
| Neurological symptoms, including gait abnormalities, weakness or sensory |
| changes |
| Feelings about overall appearance and back shape |
| Family history |
Usually, patients present spinal deformity or, more likely, chest wall and back asymmetry. Whether identified by the patient, their parents, or through school or physician screening programs, posterior chest wall prominence is the most outward manifestation of spinal curvature. With more significant scoliosis, adolescent girls sometimes notice a difference in their breast sizes. Other body characteristics may include shoulder asymmetry and overall posture imbalance in the coronal plane.
While not typically the presenting symptom, back pain is not unusual (2). Approximately one-quarter of patients with adolescent idiopathic scoliosis (AIS) present with back pain (2). Patients with idiopathic scoliosis will sometimes have back pain and, specifically, posterior chest wall pain on the side of the rib prominence. Lower back pain is common in the adolescent population with or without scoliosis. Back pain without injury that is severe and unremitting is a cause of concern and should be investigated with, at minimum, a complete examination and radiographs because there may be a more specific diagnosis (2,3). Acute back pain associated with fever, for example, should be evaluated for spinal infections. Back pain isolated to one area, which is worse at night and significantly improved with nonsteroidal anti-inflammatory drugs, may be indicative of a spinal tumour such as an osteoid osteoma.
With any spinal condition, the health care provider must be on the watch for neurological problems. A complete neurological history should include inquiries of weakness, sensory changes, problems of balance, gait and coordination, as well as bowel and bladder difficulties such as incontinence. Significant disturbances in these may suggest intraspinal pathology such as syringomyelia (central spinal cord dilation), tethered cord or tumour (4,5).
The risk of curve progression in idiopathic scoliosis and hence its treatment and prognosis is based on remaining spinal growth (6). The most reliable method of monitoring growth is simple height measurements. Therefore, the primary physician often possesses this information from their annual examinations. Furthermore, it is important to look at other markers of growth and maturity, including signs of puberty, onset of menarche and breast development.
There is a genetic component to this condition with siblings (seven times more frequently) and children (three times) of patients with scoliosis having a higher incidence (7). Adults with idiopathic scoliosis should know that their children should be carefully screened.
Finally, it is important to understand the patient’s general thoughts about their appearance. Because, as will be discussed, AIS is primarily a cosmetic deformity, treatment is based on the desire to change the shape of the back or to prevent the deformity from worsening. The self-perception of a patient and whether they are happy with their appearance is important in the decision-making process.
PHYSICAL EXAMINATION
The scoliosis patient’s physical examination should begin with the overall appearance, the skin and the neuromuscular system before the evaluation of the back’s shape (Table 2). A height measurement is important to monitor skeletal growth and the risk of scoliotic curve progression. In addition, patients who are tall with long fingers and an increased arm span to height ratio should be assessed for other signs of Marfan syndrome (such as cardiac abnormalities). Patients with joint and skin hyperlaxity along with scoliosis may need to have further work up for a connective tissue condition such as Ehlers-Danlos syndrome. High-arched or cavus feet may be associated with a neurological disorder such as Charcot-Marie-Tooth disease or a spinal cord abnormality such as a tumour. Skin inspection that notes café-au-lait spots or axillary freckles suggests neurofibromatosis, while a hairy patch or skin dimpling in the back may identify a spinal dysraphism such as myelomeningocele. Assessment of pubertal development (Tanner staging) should be included with the general appearance.
TABLE 2.
Physical examination components
| Height measurement |
| Gait check |
| Foot shape |
| Skin inspection |
| Assessment of pubertal development |
| Neurological examination, including motor, sensory and reflex tests (including abdominal) |
| Symmetry of shoulders and iliac crest |
| Forward bending test |
A complete neurological examination should evaluate balance, reflexes and motor testing in all muscle groups, and sensory testing of the lower extremities, back and chest. Rapid assessment of strength and balance can be made by observing gait, toe-walking, heel-walking, heel-to-toe walking along a straight line and hopping on one foot. Weakness of the lower extremities may be caused by a spinal mass or a central nervous system problem. Sensory changes to light touch along the back and spine may be a subtle sign of an underlying spinal syrinx causing the scoliosis. Upper and lower extremity deep tendon reflexes should be included, as well as the Babinski test. Abdominal reflexes obtained by stroking the four quadrants around the umbilicus in a supine patient (umbilicus moving toward the stroked side is normal) should be completed. Abnormal examination may indicate an intraspinal disorder such as syringomyelia.
When examining the back of a patient with suspected scoliosis, the evaluator should inspect the shoulders and hips for asymmetry. Significant leg length discrepancies, quickly judged by feeling the top of the iliac crests or the level of the dimples made by the posterior-superior iliac spines, can cause an oblique spinal take-off from the pelvis, which results in spinal curvature. The classic screening test for scoliosis, the forward bending test, is finally performed by having the patient bend forward at the waist with knees straight and palms together (Figure 1) (1,8). The examiner should look for any asymmetry in the contours of the back resulting from the rotational deformity of the spine (9). In classic thoracic scoliosis with the apex of the curve to the right, the patient’s right side is prominent. While this is most easily seen in the thoracic spine, it is important to look in the lumbar region for prominence as well. The inability to perform this test due to pain in the back or hamstring tightness can suggest other pathology, including mechanical back pain, disc herniation, spondylolysis or infection.
Figure 1.

Photograph of a patient with idiopathic scoliosis upright (A) and forward bending test (B). Note the rotational asymmetry of the back
IMAGING EVALUATION
Once scoliosis is suspected, a standing posterior-anterior radiograph should be obtained. These films are taken on a three-foot cassette if possible. Further plain radiograph imaging is beyond a screening examination and should be determined by the orthopaedic surgeon. Besides examining the curve itself, careful attention should be paid to the vertebral bodies on the radiographs. There should be two pedicles at every level and there should be rotation of the spine, with the apex of the curve having the most rotation. Remember, true scoliosis is not only a deformity in the coronal plane but is also a rotational deformity. A scoliotic curve without rotation should be investigated for other causes, including bony tumours (osteoid osteoma), intraspinal pathology (syringomyelia and masses) and nerve root irritation.
If back pain is present, a lateral radiograph of the spine including the lumbosacral region should be obtained to look for vertebral abnormalities associated with diagnoses such as spondylolysis (an idiopathic fracture of the posterior elements of the vertebral body), spondylolisthesis (a slipping forward of one vertebral body on the adjacent one), infection or bony destruction. Further imaging for patients with scoliosis and back pain may include a bone scan or a magnetic resonance imaging (MRI) test. These imaging modalities are beyond screening examinations and are usually obtained by the treating surgeons.
An MRI is not needed for most patients with AIS; although this is somewhat controversial. Some treating centres automatically request an MRI for any patient with scoliosis. However, an MRI is most likely to be useful for patients younger than 10 years of age at presentation (juvenile and infantile scoliosis) (10,11), those with left thoracic curves (11) and those with an abnormality on neurological examination.
TYPES OF SCOLIOSIS
Congenital scoliosis is due to skeletal abnormalities of the spine that are present at birth. These anomalies, which can include multiple levels, are the result of and broadly classified as a failure of formation or a failure of segmentation (or both) during vertebral development (Figure 2). Because these spinal deformities are present in utero, they are often first identified on fetal ultrasound (12). Organ systems that develop at the same gestational time (fifth to sixth week) may also demonstrate abnormalities in up to 60% of cases (13,14). Thus, it is important to identify associated anomalies with a thorough evaluation of the neurological, cardiovascular and genitourinary system, including a good neurological and cardiac physical examination, an abdominal ultrasound and an echocardiogram. Treatment is based on the age of the patient, progression of the curve, and the location and type of anomaly. The options for surgical treatment include in situ fusion and resection with correction of the deformity.
Figure 2.
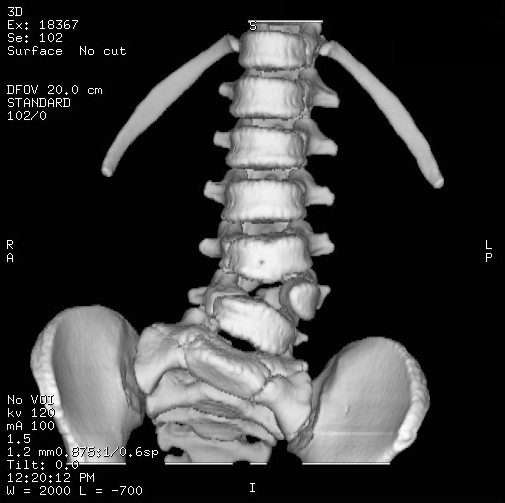
Congenital scoliosis – computed tomography depicting a hemivertebrae
Scoliosis can be associated with neurological conditions, muscular abnormalities and global syndromes. This long list of diagnoses would typically have other signs, symptoms and physical manifestations as well as scoliosis. Usually, these varying diagnoses are treated at tertiary care facilities with special expertise in the management of patients with complex multisystem problems. The caregiver who treats these patients should be familiar with the nonspinal manifestations of these conditions. Some examples can be seen in Table 3.
TABLE 3.
A partial list of syndromes and neuromuscular conditions associated with scoliosis
| Cerebral palsy |
| Charcot-Marie-Tooth disease |
| Poliomyelitis |
| Spinal muscular atrophy |
| Arthrogryposis |
| Duchenne muscular dystrophy |
| Congenital hypotonia |
| Neurofibromatosis |
| Paralysis |
| Marfan syndrome |
| Ehlers-Danlos syndrome |
| Myelomeningocele |
| Osteogenesis imperfecta |
| Achondroplasia |
As noted above, a curve can be found in the coronal plane on radiographs with minimal or no rotation of the vertebral bodies (Figure 3). Often, there is pain associated, which contributes to the deformity. This is not a true scoliosis, and other causes of the deformity should be investigated.
Figure 3.

Spinal curvature without rotation – other diagnoses apart from idiopathic scoliosis must be considered
Idiopathic scoliosis is, in some ways, a diagnosis of exclusion. However, idiopathic scoliosis is by far the most common type of spinal deformity with a prevalence of one to three per 100 (curves of greater than 10°) in an equal proportion of boys and girls (15–18). Meanwhile, the prevalence of curves greater than 30° is one to three per 1000 with a 1:8 ratio of boys to girls (18–20). Patients are divided into age at which the scoliosis presents – infantile idiopathic scoliosis in patients zero to three years of age (0.5% of idiopathic scoliosis), juvenile idiopathic scoliosis in patients four to 10 years of age (10.5% of idiopathic scoliosis), and AIS in patients older than 10 years of age (89% of idiopathic scoliosis) (21).
Infantile curves may be associated with neuroaxial abnormalities, plagiocephaly, hip dysplasia, congenital heart disease and mental retardation, and usually (90%) resolve spontaneously (7,22). Juvenile scoliosis, on the other hand, is often progressive and, due to the remaining growth, has the potential for severe trunk deformity and eventual cardiac or pulmonary compromise. If left untreated, curves that reach 30° are almost always progressive (23).
Patients with AIS typically present after 10 years of age which corresponds with rapid adolescent growth (1). The historical classification system is the King-Moe system, while the newer Lenke system is currently used more widely (24,25). Risk factors for progression include female gender, curve magnitude of greater than 50° at maturity, curve type and remaining growth. Curves progress most rapidly when the child is growing rapidly – adolescent growth spurt (26). Clinically, this can be estimated (with varying degrees of accuracy) by age (on average, girls grow until 14 years of age and boys until 16 years of age), the menarche status (typically growth is most rapid in the six months before menarche and ceases, on average, two years after menarche) and peak height velocity. Radiographically, markers for determining remaining growth include the closure of the triradiate cartilage, the ossification of the iliac crest apophysis (Risser sign) and various skeletal markers on the hand or elbow when compared with normal controls. Finally, curves greater than 30° (27) with an apex above T12 are more likely to progress (28).
NATURAL HISTORY AND TREATMENT
Natural history studies of patients with idiopathic scoliosis after skeletal maturity, found that curves less than 30° do not progress, while most curves of greater than 50° continue to progress. The progression is approximately 1° per year (29,30). In patients with severe thoracic curves (greater than 90° to 100°), there is an increased risk of cor pulmonale and right heart failure. However, an increased mortality rate has not been found in long-term studies (31,32) of patients with AIS. Pulmonary function can become limited with severe scoliosis (greater than 90°) (31,33). Back pain is common in the normal population, making studies evaluating back pain in scoliosis difficult. Some studies show a slightly higher rate of back pain in patients with AIS (34). Scoliosis has also been found to be a risk factor for psychosocial issues and health compromising behaviour (35). However, there have been no studies comparing treated and untreated patients with scoliosis to their rates of back pain and their self image.
School-based and physician screening programs are controversial. In a population-based study (36), school screening identified some of the children who went on to receive treatment but referred many more who did not. The Scoliosis Research Society (USA) recommends annual screening of all children between 10 and 14 years of age (37). The American Academy of Pediatrics has recommended screening with the forward bending test at routine health supervision visits at 10, 12, 14 and 16 years of age (38). Meanwhile, the US Preventive Services Task Force (39) and the Canadian Task Force on the Periodic Health Examination (40) concluded that there was insufficient evidence to recommend for or against routine screening of asymptomatic adolescents for idiopathic scoliosis. The US Preventive Services Task Force concluded that the harms of screening adolescents for idiopathic scoliosis may exceed potential benefits (39). Most jurisdictions have abandoned routine screening.
The treatment of scoliosis is based on the type of scoliosis, the magnitude of the curve, the number of years of growth remaining and the patient’s opinion about the shape of their back. The treatment of patients with congenital-, neuromuscular- and syndrome-associated scoliosis, and those with idiopathic scoliosis younger than 10 years of age, presents a number of controversies. These patients should be treated at specialized facilities; their treatment is beyond the scope of the present paper.
The treatment options for AIS include observation, bracing and surgery. While many other factors must be considered, the general goal is to keep curves under 50° at maturity. Typically, observation is recommended for immature patients with curves of less than 25°. Orthotic management is recommended for immature patients with progressing curves between 25° and 50° (41). There are a number of different braces (Milwaukee brace, Boston brace and the Charleston bending brace) available with varying published results. Compliance and wearing time also seems to have a role in the efficacy of bracing (42). Bracing, however, does not permanently improve or correct the curve but tries to prevent it from worsening (43). While orthotic management is the standard of care for progressive scoliosis, the scientific basis is not conclusive (1). A prospective, randomized trial to look at the efficacy of bracing is currently underway.
Surgical correction of idiopathic scoliosis is considered for curves greater than 45° in immature patients and for curves greater than 50° in mature patients. The trunk deformity and balance is also included in the decision-making process (Figure 4A) (1). As noted, the long-term consequences of an untreated patient with 55° of scoliosis at maturity are not definitive. Thus, the patient usually should be unhappy with the shape of their back to undergo a significant and potentially dangerous surgical correction of scoliotic deformity less than 60°. Surgery is usually performed during adolescence, but newer techniques allow good correction to be accomplished into early adulthood. The goals for surgical treatment are to prevent progression and to improve spinal alignment and balance. The hips and shoulders should be level, and the head over the sacrum while maintaining sagittal alignment. The spine is corrected with a combination of rods, hooks, screws and wires while being fused by bone graft – either from the patient, a cadaver or artificially (Figure 4B). Strategies include fusion with and without instrumentation from the anterior, the posterior or both depending on the curve type, age and surgeon preference. The techniques for the correction and fusion change quickly; long-term results have not been obtained for the newest techniques. However, with older technology, good results have been found in a 20-year follow-up period (44).
Figure 4.

A Typical adolescent idiopathic scoliosis requiring correction and fusion; B Fused spine with hook and screw construct
Given these treatment guidelines, primary care physicians should refer any child with an atypical curve of greater than 10° to a specialist, including patients younger than 10 years of age, those with left thoracic curves, those with neurological abnormalities or those with significant pain. A child older than 10 years of age who has not reached skeletal maturity can be referred at any time, but definitely once the curve reaches 20° to 25°. Because typical scoliosis rarely progresses faster than 1° per month, a referral within three to six months is appropriate. Atypical scoliosis should be seen within one month.
SUMMARY
Scoliosis is a deviation of the spine consisting of lateral curvature and rotation of the vertebrae. While scoliosis is associated with many diagnoses, the vast majority of patients encountered are idiopathic in nature. A thorough history and physical examination and radiographs should be completed to identify nonidiopathic causes of the scoliosis. The treatment for idiopathic scoliosis is based on age, curve magnitude and risk of progression, and includes observation, orthotic management and surgical correction.
REFERENCES
- 1.Morrissy RT, Weinstein SL. Lovell and Winter’s Pediatric Orthopaedics. Philadelphia: Lippincott Williams & Wilkins; 2006. pp. 693–762. [Google Scholar]
- 2.Ramirez N, Johnston CE, Browne RH. The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am. 1997;79:364–8. doi: 10.2106/00004623-199703000-00007. [DOI] [PubMed] [Google Scholar]
- 3.Mehta MH. Pain provoked scoliosis. Observation on the evolution of the deformity. Clin Orthop Relat Res. 1978;135:58–65. [PubMed] [Google Scholar]
- 4.Baker AS, Dove J. Progressive scoliosis as the presenting sign of syringomyelia. Report of a case. J Bone Joint Surg Br. 1983;65:472–3. doi: 10.1302/0301-620X.65B4.6874721. [DOI] [PubMed] [Google Scholar]
- 5.Citron N, Edgar MA, Sheehy J, Thomas DG. Intramedullary spinal cord tumours presenting as scoliosis. J Bone Joint Surg Br. 1984;66:513–7. doi: 10.1302/0301-620X.66B4.6746684. [DOI] [PubMed] [Google Scholar]
- 6.Little DG, Song KM, Katz D, Herring JA. Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am. 2000;82:685–93. doi: 10.2106/00004623-200005000-00009. [DOI] [PubMed] [Google Scholar]
- 7.Wynn-Davies R. Familial (idiopathic) scoliosis. A family survey. J Bone Joint Surg Br. 1968;50:24–30. [PubMed] [Google Scholar]
- 8.Adams W. London: Churchill Livingston; 1865. Lectures on Pathology and Treatment of Lateral and Other Forms of Curvature of the Spine. [Google Scholar]
- 9.Grossman TW, Mazur JM, Cummings RJ. An evaluation of the Adams forward bend test and the scoliometer in a scoliosis school screening setting. J Pediatric Orthop. 1995;15:535–8. doi: 10.1097/01241398-199507000-00025. [DOI] [PubMed] [Google Scholar]
- 10.Gupta P, Lenke LG, Bridwell KH. Incidence of neural axis abnormalities in infantile and juvenile patients with spinal deformity. Is a magnetic resonance image screening necessary? Spine. 1998;23:206–10. doi: 10.1097/00007632-199801150-00011. [DOI] [PubMed] [Google Scholar]
- 11.Schwend RM, Hennrikus W, Hall JE, Emans JB. Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am. 1995;77:46–53. [PubMed] [Google Scholar]
- 12.Barnewolt CE, Estroff JA. Sonography of the fetal central nervous system. Neuroimaging Clin N Am. 2004;14:255–71. doi: 10.1016/j.nic.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 13.Basu PS, Elsebaie H, Noordeen MH. Congenital spinal deformity: A comprehensive assessment at presentation. Spine. 2002;27:2255–9. doi: 10.1097/00007632-200210150-00014. [DOI] [PubMed] [Google Scholar]
- 14.Beals RK, Robbins JR, Rolfe B. Anomalies associated with vertebral malformations. Spine. 1993;18:1329–32. doi: 10.1097/00007632-199308000-00012. [DOI] [PubMed] [Google Scholar]
- 15.Kane WJ, Moe JH. A scoliosis-prevalence survey in Minnesota. Clin Orthop Relat Res. 1970;69:216–8. [PubMed] [Google Scholar]
- 16.Stirling AJ, Howel D, Millner PA, Sadiq S, Sharples D, Dickson RA. Late-onset idiopathic scoliosis in children six to fourteen years old: A cross-sectional prevalence study. J Bone Joint Surg Am. 1996;78:1330–6. doi: 10.2106/00004623-199609000-00006. [DOI] [PubMed] [Google Scholar]
- 17.Rogala EJ, Drummond DS, Gurr J. Scoliosis: Incidence and natural history. A prospective epidemiological study. J Bone Joint Surg Am. 1978;60:173–6. [PubMed] [Google Scholar]
- 18.Montgomery F, Willner S. The natural history of idiopathic scoliosis: Incidence of treatment in 15 cohorts of children born between 1963 and 1977. Spine. 1997;22:772–4. doi: 10.1097/00007632-199704010-00012. [DOI] [PubMed] [Google Scholar]
- 19.Kane WJ. Scoliosis prevalence: A call for a statement of terms. Clin Orthop Relat Res. 1977;126:43–6. [PubMed] [Google Scholar]
- 20.Bunnell WP. The natural history of idiopathic scoliosis before skeletal maturity. Spine. 1986;11:773–6. doi: 10.1097/00007632-198610000-00003. [DOI] [PubMed] [Google Scholar]
- 21.Risenborough EJ, Wynne-Davies R. A genetic survey of idiopathic scoliosis in Boston, Massachusetts. J Bone Joint Surg Am. 1973;55:974–82. [PubMed] [Google Scholar]
- 22.Lloyd-Roberts GC, Pilcher MF. Structural idiopathic scoliosis in infancy. J Bone Joint Surg Br. 1965;47:520–3. [PubMed] [Google Scholar]
- 23.Tolo VT, Gillespie R. The characteristics of juvenile scoliosis and results of its treatment. J Bone Joint Surg Br. 1978;60-B:181–8. doi: 10.1302/0301-620X.60B2.659460. [DOI] [PubMed] [Google Scholar]
- 24.King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am 2001. 1983;65-A:1302–13. [PubMed] [Google Scholar]
- 25.Lenke LG, Betz RR, Harms J. Adolescent idiopathic scoliosis: A new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am. 83-A:1169–81. [PubMed] [Google Scholar]
- 26.Loncar-Dusek M, Pecina M, Prebeg Z. A longitudinal study of growth velocity and development of secondary gender characteristics versus onset of idiopathic scoliosis. Clin Orthop Relat Res. 1991;270:278–82. [PubMed] [Google Scholar]
- 27.Peterson LE, Nachemson AL. Prediction of progression of the curve in girls who have adolescent idiopathic scoliosis of moderate severity. Logistic regression analysis based on data from the Brace Study of the Scoliosis Research Society. J Bone Joint Surg Am. 1995;77:823–7. doi: 10.2106/00004623-199506000-00002. [DOI] [PubMed] [Google Scholar]
- 28.Nachemson A, Lonstein JE, Weinstein SL. Park Ridge: Natural History Committee of Scoliosis Research Society; 1982. Report of the prevalence and natural history committee. [Google Scholar]
- 29.Weinstein SL, Ponseti IV. Curve progression in idiopathic scoliosis. J Bone Joint Surg Am. 1983;65:447–55. [PubMed] [Google Scholar]
- 30.Weinstein SL. Idiopathic scoliosis. Natural history. Spine. 1986;11:780–3. doi: 10.1097/00007632-198610000-00006. [DOI] [PubMed] [Google Scholar]
- 31.Weinstein SL, Zavala DC, Ponseti IV. Idiopathic scoliosis: Long term follow-up and prognosis in untreated patients. J Bone Joint Surg Am. 1981;63:702–12. [PubMed] [Google Scholar]
- 32.Pehrsson K, Larsson S, Oden A, Nachemson A. Long-term follow-up of patients with untreated scoliosis. A study of mortality, causes of death, and symptoms. Spine. 1992;17:1091–6. doi: 10.1097/00007632-199209000-00014. [DOI] [PubMed] [Google Scholar]
- 33.Pehrsson K, Bake B, Larsson S, Nachemson A. Lung function in adult idiopathic scoliosis: A 20 year follow up. Thorax. 1991;46:474–8. doi: 10.1136/thx.46.7.474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mayo NE, Goldberg MS, Poitras B, Scott S, Hanley J. The Ste-Justine Adolescent Idiopathic Scoliosis Cohort Study. Part III: Back pain. Spine. 1994;19:1573–81. doi: 10.1097/00007632-199407001-00005. [DOI] [PubMed] [Google Scholar]
- 35.Payne WK, III, Ogilvie JW, Resnick MD, Kane RL, Transfeldt EE, Blum RW. Does scoliosis have a psychological impact and does gender make a difference? Spine. 1997;22:1380–4. doi: 10.1097/00007632-199706150-00017. [DOI] [PubMed] [Google Scholar]
- 36.Yawn BP, Yawn RA, Hodge D, et al. A population based study of school scoliosis screening. JAMA. 1999;282:1427–32. doi: 10.1001/jama.282.15.1427. [DOI] [PubMed] [Google Scholar]
- 37.Scoliosis Research Society. Park Ridge: Scoliosis Research Society; 1986. A handbook for patients. [Google Scholar]
- 38.American Academy of Pediatrics. Elk Grove Village: American Academy of Pediatrics; 1988. Guidelines for health supervision II. [Google Scholar]
- 39.US Preventive Services Task Force. Guide to Clinical Preventive Services. 2nd edn. Washington DC: Office of Disease Prevention and Health Promotion; 1996. [Google Scholar]
- 40.Canadian Task Force on Periodic Health Examination. Canadian guide to clinical preventive care. Ottawa: Canada Communication Group; 1994. pp. 346–54. [Google Scholar]
- 41.Nachemson AL, Peterson LE. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. J Bone Joint Surg Am. 1995;77:815–22. doi: 10.2106/00004623-199506000-00001. [DOI] [PubMed] [Google Scholar]
- 42.Rowe DE, Bernstein SM, Riddick MF, Adler F, Emans JB, Gardner-Bonneau D. A meta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. J Bone Joint Surg Am. 1997;79:664–74. doi: 10.2106/00004623-199705000-00005. [DOI] [PubMed] [Google Scholar]
- 43.Willers U, Normelli H, Aaro S, Svensson O, Hedlund R. Long-term results of Boston brace treatment on vertebral rotation in idiopathic scoliosis. Spine. 1993;18:432–5. [PubMed] [Google Scholar]
- 44.Dickson JH, Mirkovic S, et al. Results of operative treatment of idiopathic scoliosis in adults. J Bone Joint Surg Am. 1995;77:513–23. doi: 10.2106/00004623-199504000-00003. [DOI] [PubMed] [Google Scholar]