

Abstract
Objective
This study examined the relationship between weight status and self-concept in a sample of preschool-aged girls and whether parental concern about child overweight or restriction of access to food are associated with negative self-evaluations among girls.
Method
Participants were 197 5-year-old girls and their parents. Girls’ weight status (weight for height percentile) was calculated based on height and weight measurements. Girls’ self-concept was assessed using an individually administered questionnaire. Parents’ concern about their child’s weight status and restriction of their child’s access to food were assessed using a self-report questionnaire.
Results
Girls with higher weight status reported lower body esteem and lower perceived cognitive ability than did girls with lower weight status. Independent of girl’s weight status, higher paternal concern about child overweight was associated with lower perceived physical ability among girls; higher maternal concern about child overweight was associated with lower perceived physical and cognitive ability among girls. Finally, higher maternal restriction of girls’ access to foods was associated with lower perceived physical and cognitive ability among girls with higher weight status but not among girls with lower weight status.
Conclusions
At least as early as age 5 years, lower self-concept is noted among girls with higher weight status. In addition, parents’ concern about their child’s weight status and restriction of access to food are associated with negative self-evaluations among girls. Public health programs that raise parental awareness of childhood overweight without also providing constructive and blame-free alternatives for addressing child weight problems may be detrimental to children’s mental health.
Children in the United States are becoming more overweight. In the past 2 decades, a twofold increase in the prevalence of overweight has been reported among children aged 6 to 17 years.1 Today, ~14% of school-aged children are overweight and another 11% are at risk of overweight.1. Increased rates of overweight are also noted among preschool-aged children, particularly 4- to 5-year-old girls.2 (Overweight was defined conservatively, ie, ≥95th weight for height percentile (WHP). A less conservative definition of overweight, ie, ≥85th WHP, Himes and Dietz, 1994, will be adopted in this article.) Consequently, overweight is regarded as the most prevalent nutritional disease among children and adolescents in the United States.3 Childhood overweight has been associated with numerous negative health and psychological outcomes including noninsulin-dependent diabetes,4 hypertension,5 sleep apnea,6 depression,7 and disturbed body image.8,9 Childhood overweight has also been associated with negative self-evaluations among school-aged children and adolescents,10,11 possibly because overweight children are negatively evaluated by their peers.12–15 The relationship between childhood overweight and self-evaluations has rarely been considered among preschool-aged children. In addition, there is little information regarding how parental reaction to childhood overweight during the preschool years is associated with the young child’s developing sense of self. This study examines the relationship between weight status and self-concept in preschool-aged girls and explores whether parents’ concern about their daughter’s weight status or restriction of her access to food is associated with negative self-evaluations.
Self-concept can be defined as a schema of oneself. (Terms such as self-identity, self-image, and self-identity are used interchangeably with self-concept in the literature.) This schema incorporates descriptors used to define the self (eg, I am tall, I am smart) and the overall evaluative tone associated with such descriptors, generally referred to as self-esteem or general self-concept (eg, I think that I am a good person). Self-concept is multidimensional.16 In addition to a general sense of self, individuals develop self-representations in domains such as physical-appearance self (including body esteem), athletic self, social self, and academic self. A substantial body of research suggests that overweight children experience low self-concept across a number of domains of self-concept. Among school-aged children and adolescents, concurrent associations have been found between childhood overweight and low global self-concept,10,11,17–21 athletic self-concept,17,22 and physical appearance self-concept.9,18,19,22 Using a sample of preschool-aged children, Klesges et al23 found that athletic self-concept negatively and prospectively correlated with body fat 1 and 2 years later.
A notable body of research, however, has failed to identify a relationship between childhood overweight and self-concept.23–25 Consequently, it is difficult to draw any conclusions about the relationship between childhood overweight and self-concept. There are a number of reasons for the inconsistency in research findings including varying definitions of overweight, the use of both unidimensional (assessing only general self-concept) and multidimensional (assessing all domains of self-concept) measures of self-concept, and differing samples. In addition, previous research has assessed only the direct relationship between weight status and self-concept,26 that is, the main effect of weight status on self-concept. The search for main effects, in contrast to interaction effects, assumes that all overweight children will be similarly affected by their weight status.
An overweight child is embedded in a social context. This context provides clues to the child about the acceptability of his or her weight status. Certain factors within this environment may protect the child from self-depreciating thoughts or may place the child at risk of such thoughts. With the physical and emotional well-being of their child in mind, parents of an overweight child may react to their child’s weight status by expressing concern and by altering the feeding environment. A concerned parent may directly or indirectly criticize their child in an effort to encourage behavioral change. In addition, concerned parents may exert strict control over the types and quantities of food their child has access to in an attempt to foster healthful eating and to contest weight gain. Parental concern and control in the feeding domain may send children the message that their weight status is undesirable and that they are not capable of controlling their eating habits. These messages, when combined with being overweight, may negatively impact a child’s evolving sense of self.
The present study assesses the relationship between weight status and self-concept using a sample of 5-year-old girls. We have chosen to focus on 5-year-old girls because there has been a dramatic increase in the prevalence of overweight among 4- to 5-year-old girls2 and research has rarely considered the relationship between weight status and self-concept in preschool-aged children. Preschool girls are of particular interest because body dissatisfaction and concern about weight are more often noted among girls than among boys.27–29 Three particular questions will be addressed. First, do 5-year-old girls with higher weight status experience lower self-concept across the various domains of self-concept? Second, is parental concern about their daughter’s weight status, or parental restriction of access to food, associated with lower self-concept among girls, independent of their weight status? Third, is higher weight status in combination with parental concern or restriction associated with lower self-concept among girls? That is, is there an interaction between weight status and parent concern or restriction in predicting girls’ self-concept?
METHODS
Participants
Participants were 197 5-year-old girls (mean: 5.4 ± .3 years; range: 4.6–6.4 years) and their parents. Families were recruited for participation in a study of the “health and development of young girls.” Eligibility criteria for girls’ participation included living with both biological parents, the absence of severe food allergies or chronic medical problems affecting food intake, and the absence of dietary restrictions involving animal products. The sample included a mixture of families from rural and nonrural areas from central Pennsylvania. All families participating were non-Hispanic white. Based on power calculations, this sample was deemed appropriate (ie, large enough) to test the hypotheses herein.
Procedures
Each girl was individually interviewed by a trained interviewer on 2 separate occasions approximately 1 week apart. Before data collection began, all interviewers received extensive training on interview skills, the importance of neutrality when interviewing (particularly with young children), and the necessity of standardization across all interview procedures. In addition, all interview sessions were monitored by a trained psychologist during the beginning of data collection and periodically throughout the remaining months of data collection to ensure the quality of data collected.
Parents also visited the laboratory (within approximately 1 month of their daughter’s visit) and completed a series of questionnaires. In addition to the information gained from the questionnaires, trained staff members collected 3 height and weight measurements each for girls, mothers, and fathers. The present study was reviewed and approved by the institutional review board of Pennsylvania State University. Mothers and fathers provided written consent for their participation and mothers provided written consent for their daughters.
Measures
Weight Status
Based on the recommendations of Lohman et al,30 3 height and weight measurements were collected for each girl by a trained research assistant and average weight and height were used to calculate the ratio of weight for height. Weight for height scores were converted into percentile rankings (WHP) based on National Center for Health Statistics reference values.
Self-Concept
The Pictorial Scale of Perceived Competence and Social Acceptance for Young Children (PCSA) was used to assess girls’ self-concept.31 The PCSA was devised to be developmentally appropriate for children aged 4 to 7 years. The 24-item scale assesses 4 dimensions of self-concept (6 items per scale) or perceived competence, including physical ability (eg, “This girl is good at running”), cognitive ability (eg, “This girl is good at puzzles”), peer acceptance (eg, “This girl can make friends easily”), and maternal acceptance (eg, “This girl’s mother smiles at her a lot”). Scores for each of the 4 subscales were averaged to give perceived competence scores ranging from 1 (not competent) to 4 (really competent) for each subscale.
The PCSA is not a clinical instrument; there are no norms to define what is considered a healthy self-concept and what is considered problematic. Rather the PSCA is designed to assess self-concept in children, relative to the sample. The PCSA was chosen over other measures of self-concept for a number of reasons. First, the PCSA is a multidimensional measure of self-concept; that is, the PCSA creates separate scores for each domain of self. As a result, it is possible to assess whether weight status is differentially associated with each domain of self. Second, the PCSA was developed specifically for children aged 4 to 7 years.31 Third, Harter and Pike31 effectively illustrated that the PCSA shows good convergent validity, discriminant validity, and predictive validity in preschool and first and second grade children. In addition, Harter and Pike reported internal consistency coefficients, for kindergarten-aged children, ranging from .50 to .85 across the 4 subscales. In the present study, internal consistency coefficients ranged from .56 to .73.
Body Esteem
Although the PCSA for young children measures physical ability, it does not assess body esteem or physical appearance self-concept. This dimension of self-concept is central to the present study because potentially adverse psychological consequences of being overweight are most likely to be reflected through perceived physical appearance, in addition to other dimensions of the self. Therefore, in addition to the PCSA, the Body Esteem scale was included in the present study.9 The Body Esteem scale is a 24-item scale that assesses overall, nonspecific body esteem (eg, “I like what I look like in pictures,” “I’m proud of my body,” and “I wish I were thinner”) and is suitable for use with young children. The Body Esteem scale does not necessarily measure whether children are aware that they are overweight, rather it assesses their general opinion about their body and physical appearance. To increase variability in responses, the response set was adjusted slightly from a 2-item response set (yes/no) to a 3-item response set (yes/no/sometimes). Responses for all the items were summed to create a total body esteem score.
The Body Esteem scale is not a clinical instrument; therefore, there are no norms defining healthy and problematic body esteem. The reliability and validity of the Body Esteem scale has been previously assessed. In a sample of 7- to 12-year-old children, Mendelson and White9 reported that the Body Esteem scale had a split-half reliability of r = .85 (odd-even split) and displayed concurrent validity with the Physical Attributes subscale of the Piers-Harris Self-Concept scale (r = .67). In the present study, Cronbach’s α for the Body Esteem scale was .73.
Parent Child Feeding Practices
The Child Feeding Questionnaire was developed within the laboratory and is a parent self-report measure that taps parental feeding strategies and ideas about child feeding.32 Two subscales from the Child Feeding Questionnaire were deemed appropriate for the present study as indices of parent reaction to child overweight: 1) concern about child overweight and 2) restriction of child access to and intake of food.
Concern about child overweight was assessed using the questions: 1) How concerned are you about your child eating too much when you are not around her?; 2) How concerned are you about your child having to diet to maintain a desirable weight?; and 3) How concerned are you about your child becoming overweight? Parents responded to these questions using a scale of 1 to 5, unconcerned to concerned. Responses for the 3 items were averaged separately for mother and fathers to create a total concern score for each parent. Cronbach’s α was .74 for maternal concern and .77 for paternal concern.
Restriction of child access to food was assessed using the items: 1) I have to be sure that my child does not eat too many sweets/high fat foods/of her favorite foods (the question is asked for each type of food); 2) I intentionally keep some foods out of my child’s reach; 3) I offer sweets/favorite foods as a reward for good behavior; and 4) If I did not guide or regulate my child’s eating she would eat too many junk foods/of her favorite foods. Parents responded to these items using a scale of 1 to 5 (agree to disagree). As with the concern scale, responses for each of the restriction items were averaged to create a total restriction score for each parent. Cronbach’s α was .78 for maternal restriction and .66 for paternal restriction.
Parental Control
The General Parental Control Scale (GPCS), developed by Baumrind,33 was used to assess mothers’ and fathers’ beliefs regarding general control in parenting (ie, not specific to the feeding domain). This measure consists of 13 items and uses a 4-response option Likert scale, from disagree strongly to agree strongly. Example items include; “A child who defies authority is not very likeable” and “It is all right with me if my child argues with me about my decisions.” A total control score was created for each parent by calculating the average across all items. Using a sample of parents of preschool-aged girls and boys, Baumrind33 found that self-reported control by parents was correlated with observed parenting behavior. In the present study Chronbach’s was .72 for mothers and .72 for fathers. The GPCS was used in the present study to determine whether mothers’ and fathers’ reports of restriction and concern reflected general practices of control in parenting.
Statistical Analyses
Analyses were conducted using SAS Software, Version 6.12 (Cary, NC). Multiple regression analysis was used to assess the following questions. First, do girls with higher weight status experience lower self-concept? Second, do girls of parents who express higher levels of concern about child overweight or restrict their access to food experience lower self-concept (independent of their weight status)? Third, does the relationship between parental concern or restriction and girls’ self-concept vary for girls with higher and lower weight status? For each dimension of self-concept (ie, cognitive ability, physical ability, physical appearance or body esteem, maternal acceptance, and peer acceptance), multiple regression analysis was used to assess: 1) the main effect of girls’ weight status, 2) the main effect of parent concern or parent restriction, and 3) the interaction between girls’ weight status and parent concern/restriction. A significance level of P < .05 was used for all analyses.
Variables were entered into the analysis in a hierarchical fashion. Girls’ weight status was entered first into the model to assess the basic relationship between weight status and self-concept, irrespective of parent reaction to child overweight. Parent concern/restriction was entered second into the model to assess the relationship between parent concern/restriction and child self-concept, independent of girls’ weight status. The interaction between weight status and parent concern/restriction was entered last into the model, once the main effects had been taken into consideration. Analyses were conducted separately for parent concern and parent restriction and for mothers and fathers.
In a follow-up series of analyses, correlations between parental control (using scores from the GPCS) and parental restriction and concern were calculated to determine whether restriction and concern reflect broader parenting practices and beliefs. In cases in which the GPCS was significantly correlated with parental concern or restriction, all significant relationships previously identified were reanalyzed controlling for general parental control to determine whether the effects of concern and restriction were independent of general parental control.
RESULTS
Two thirds of parents reported a level of education higher than a high school diploma. All fathers and two thirds of mothers were employed and approximately equal proportions of families reported incomes below $35 000, between $35 000 and $50 000, and above $50 000. WHP rankings for girls ranged from 6.43 to 99.8. Based on criteria outlined by Himes and Dietz,34 48 girls were overweight (WHP ≥ 85), 20 of these 48 girls were obese (WHP ≥ 95), and 149 girls were nonoverweight (WHP < 85); that is, 25% of girls were overweight and 10% were obese. These rates are similar to population-based rates of overweight and obesity among young non-Hispanic white girls.1,2
To initially display trends for girls’ weight status, mean self-concept and parental concern and restriction scores are reported in Table 1 for the entire sample and separately for overweight (≥85th WHP) and nonoverweight (<85th WHP) girls. As shown in Table 1, overweight girls reported significantly lower body esteem and perceived cognitive ability than nonoverweight girls. In addition, parents of overweight girls reported significantly higher levels of concern about their daughter’s weight than did parents of nonoverweight girls. Results from regression analyses assessing relationships among girls’ self-concept, girls’ weight status (used as a continuous rather than categorical variable), and parental concern and restriction are reported in Table 2. Results are presented separately for each domain of self-concept.
TABLE 1.
Mean Self-Concept, Parent Concern, and Parent Restriction for the Entire Sample and for Overweight and Nonoverweight Girls
| Nonoverweight Girls (n = 149) WHP, <85 | Overweight Girls (n = 48) WHP ≥ 85 | Entire Sample | |
|---|---|---|---|
| Weight for height percentile | 51.81 (21.45)** | 93.33 (4.85)** | 61.92 (25.93) |
| Body esteem | 57.03 (7.05)* | 54.68 (6.51)* | 56.45 (6.98) |
| Physical ability | 3.47 (0.43) | 3.36 (.57) | 3.45 (.47) |
| Cognitive ability | 3.61 (.38)** | 3.33 (.63)** | 3.54 (.47) |
| Peer acceptance | 3.04 (.62) | 2.98 (.66) | 3.03 (.63) |
| Maternal acceptance | 3.08 (.60) | 3.11 (.61) | 3.09 (.60) |
| Maternal concern | 2.06 (1.10)** | 2.97 (1.09)** | 2.28 (1.16) |
| Paternal concern | 2.09 (1.11)** | 2.84 (1.11)** | 2.28 (1.15) |
| Maternal restriction | 2.89 (.85) | 3.07 (.95) | 2.93 (.85) |
| Paternal restriction | 3.08 (.69) | 3.22 (.72) | 3.11 (.69) |
Analyses compared overweight and nonoverweight girls. The scale range for the body esteem scale is 24 to 72. The scale range for all other measures is 1 to 4.
P < .05.
P < .01.
TABLE 2.
Results of Analyses Assessing the Main Effects of Weight Status, Parental Concern, and Parental Restriction and the Interaction Between Weight Status and Parental Concern/Restriction in Predicting Girls’ Self-Concept
| Outcome Variable | Predictor Variables | β | |
|---|---|---|---|
| Girls’ body esteem | Weight status | WHP | −.13* |
| Parental concern† | Maternal concern | −.03 | |
| Paternal concern | −.17* | ||
| Parental restriction† | Maternal restriction | −.04 | |
| Paternal restriction | −.09 | ||
| Interactions‡ | WHP × maternal concern | .10 | |
| WHP × paternal concern | .10 | ||
| WHP × maternal restriction | .01 | ||
| WHP × paternal restriction | .04 | ||
| Girls’ perceived physical ability | Weight status | WHP | −.07 |
| Parental concern† | Maternal concern | −.20** | |
| Paternal concern | −.02 | ||
| Parental restriction† | Maternal restriction | −.05 | |
| Paternal restriction | −.12 | ||
| Interactions‡ | WHP × maternal concern | −.01 | |
| WHP × paternal concern | −.05 | ||
| WHP × maternal restriction | −.15**§ | ||
| WHP × paternal restriction | −.12 | ||
| Girls’ perceived cognitive ability | Weight status | WHP | −.22** |
| Parental concern† | Maternal concern | −.21** | |
| Paternal concern | −.03 | ||
| Parental restriction† | Maternal restriction | −.08 | |
| Paternal restriction | −.18 | ||
| Interactions‡ | WHP × maternal concern | −.07 | |
| WHP × pernal concern | −.12 | ||
| WHP × maternal restriction‡ | −.15**|| | ||
| WHP × paternal restriction | −.05 |
Results are only reported for dependent variables for which significant relationships were identified.
P < .05.
P < .01.
In analyses assessing the main effects of parental concern or parental restriction, weight status was also entered into the model to assess the effect of concern/restriction, independent of weight status.
In all interaction analyses, weight status and concern/restriction were also entered into the model.
The WHP × maternal restriction interaction for physical ability resulted in the following regression equation: perceived physical ability = 3.59 − .001 (WHP) − .017 (restriction) − .003 (interaction).
The WHP × maternal restriction interaction for cognitive ability resulted in the following regression equation: perceived cognitive ability = 3.89 − .004 (WHP) − .033 (restriction) − .003 (interaction).
Body Esteem
Results from regression analyses showed a negative relationship between girls’ weight status and girls’ body esteem (see Table 2). That is, girls with higher weight status reported lower body esteem than girls with lower weight status. In addition, a negative relationship was found between fathers’ concern about their daughter’s weight status and girls’ body esteem (see Table 2). Higher concern among fathers was associated with lower body esteem among their daughters, independent of girls’ weight status.
Perceived Physical Ability
No relationship was identified between girls’ weight status and perceived physical ability. A negative relationship, however, was identified between mothers’ concern about their daughter’s weight status and girls’ perceived physical ability (see Table 2). Higher concern among mothers was associated with lower perceived physical ability among their daughters, independent of girls’ weight status.
A negative interaction was found between maternal restriction and girls’ weight status in predicting girls’ perceived physical ability (see Table 2 and Fig 1A). Little difference was noted in perceived physical ability for girls with higher and lower weight status when maternal restriction was low (ie, 1). When maternal restriction was high (ie, 4), however, girls with higher weight status reported substantially lower perceived physical ability in comparison to girls with lower weight status.
Fig 1.
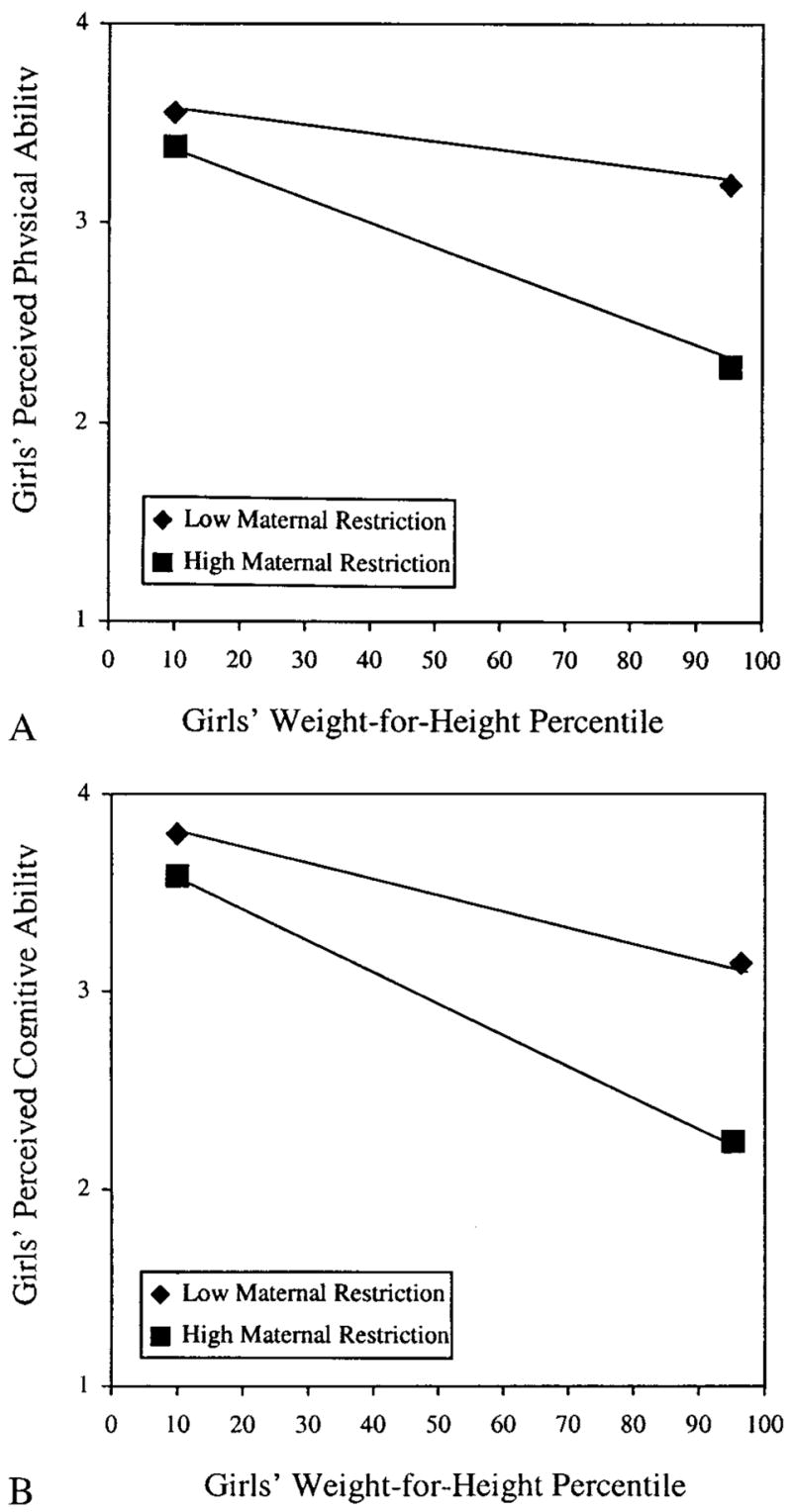
A, Predicting girls’ perceived physical ability based on the interaction between weight for height percentile and maternal restriction of child access to food. B, Predicting girls’ perceived cognitive ability based on the interaction between weight for height percentile and maternal restriction of child access to food.
Perceived Cognitive Ability
A negative relationship was identified between girls’ weight status and perceived cognitive ability (see Table 2). Girls with higher weight status reported lower perceived cognitive ability than girls with lower weight status. In addition, a negative relationship was noted between mothers’ concern about their daughter’s weight status and girls’ perceived cognitive ability (see Table 2). Higher concern among mothers was associated with lower perceived cognitive ability among their daughters, independent of girls weight status.
The relationship between girls’ weight status and perceived cognitive ability was modified by a negative interaction between girls’ WHP and maternal restriction (see Table 2 and Fig 1B). Little difference was noted in perceived cognitive ability for girls with higher and lower weight status when maternal restriction was low. However, when maternal restriction was high, girls with higher weight status reported substantially lower perceived physical ability in comparison to girls with lower degrees of weight status.
Perceived Peer Acceptance and Maternal Acceptance
No relationship was identified between girls’ perceived maternal or peer acceptance and girls’ weight status, parental concern, or parental restriction.
Follow-Up Analyses
Relationships identified between parental concern and restriction and girls’ self-concept could simply reflect the association between concern/restriction and general practices of parental control. A follow-up series of analyses were run to address this possibility. A significant correlation was found between mothers’ scores on the GPCS and mothers’ concern about their daughter’s weight status (r = .15; P = .03). No relationship was found between mothers’ scores on the GPCS and maternal restriction. A significant correlation was found between fathers’ scores on the GPCS and paternal concern about their daughter’s weight status (r = .18; P = .01) and paternal restriction (r = .15; P = .03). Consequently, all significant relationships identified above were reassessed controlling for parents’ GPCS scores to determine whether the effects identified were independent of general parental control. Neither the significance level nor the strength of the associations (ie, the β-weight) changed after controlling for general parental control.
DISCUSSION
The present study examined relationships among 5-year-old girls’ weight status, parents’ reaction to their daughter’s weight status, and girls’ self-concept. Girls with higher weight status reported lower body esteem and lower perceived cognitive ability than girls with lower weight status. In addition, parents’ concern about their daughter’s weight status and restriction of their daughter’s access to food were associated with lower self-perceptions among girls. Independent of girls’ actual weight status, higher concern among fathers about their daughter’s weight status was associated with lower body esteem among girls and higher maternal concern was associated with lower perceived physical ability and cognitive ability among girls. Finally, higher weight status among girls, in combination with higher levels of maternal restriction of access to food, was associated with lower perceived cognitive ability and physical ability among girls. Results from the present study support previous research identifying lower psychological well-being among overweight school-aged children and adolescents, in comparison to their nonoverweight peers, and extend these findings to preschool-aged girls. Parents’ concern about their child’s weight status and restriction of their child’s access to food are also associated with negative psychological outcomes linked to childhood overweight.
Body Esteem
Girls with higher weight status reported lower body esteem. This result supports research with older children and suggests that the stigmatizing impact of overweight may be experienced as early as the preschool years. Previous research has shown that girls as young as 5 years old express a fear of gaining weight.35 It seems, therefore, that young girls may be well aware of what is considered physically attractive (ie, a thin body shape) and may judge their own bodies accordingly. This early awareness may be caused by the pervasive image of the thin ideal portrayed in the media, the extensive amount of time preschool-aged children spend watching television,36 and teasing experienced by overweight children.19,21,37
Higher concern among fathers about their daughter’s weight status was also associated with lower body esteem among girls. Previous research has shown that children aged 9 years and older are accurate evaluators of their parents’ perception of their body shape.19 Findings from the present study suggest that girls as young as 5 years of age may be aware of how their fathers perceive their body shape and that these perceptions may influence daughters’ self evaluations. Previous research has rarely considered the role of fathers in girls’ evolving sense of self or the development of weight concerns, although research indicates that fathers play a central role in girls’ development in related areas, including gender role development38–40 and food acceptance patterns.41 Unfortunately, the exact means by which parents express concern was not assessed in the present study. Future research could build on the findings of the present study by assessing ways in which parents express concern about their child’s weight status and the impact that each method has on children’s self-concept.
Perceived Cognitive Ability
In addition to lower body esteem, girls with higher weight status reported lower perceived cognitive ability. This finding suggests that there may be a spillover effect of weight status on domains of self that are less central to physical appearance. There are a variety of possible explanations for this relationship. First, girls with higher weight status may endorse the stereotype, often portrayed in children’s programs, that fat is synonymous with stupid.12 Second, girls with higher weight status may be more likely to come from families with lower levels of education who, as a result, place less emphasis on the importance of education and academic achievement. In this sample, however, no differences in parent education were noted for overweight (≥85th WHP) and nonoverweight girls (<85th WHP). Third, girls with higher weight status may actually have lower cognitive ability than girls with lower weight status. Finally, lower cognitive ability may have preceded higher weight status. Unfortunately, only familial differences in educational status as a possible mediator of the relationship between weight status and perceived cognitive ability could be addressed in the present study.
Higher concern among mothers with their daughters’ weight status was associated with lower perceived cognitive ability among girls, independent of girls’ weight status. That is, maternal concern was associated with lower perceived cognitive ability for girls’ with higher and lower weight status alike. In addition, higher levels of maternal restriction of daughters’ access to food, such as keeping snack foods out of girls’ reach, were associated with lower perceived cognitive ability for girls with higher weight status, but not for girls with lower weight status. Interestingly, girls with higher weight status did not experience higher levels of parental restriction (as shown in Table 1) rather they seem to be differentially influenced by parental restriction. Although parental concern and restriction are associated with general control in the domain of parenting, referred to as authoritarian parenting, the relationships identified were found to be independent of general levels of parental control. Therefore, it seems that mechanisms linking parental concern or restriction and child self-concept are specific to the feeding domain and are independent of general parenting style. Control specific to the feeding domain, when combined with high weight status, may send children messages of incompetence that generalize across a multiple domains of self. As previously mentioned for parental concern, it is unknown how parents’ reports of restriction are related to their actual behavior. Future research should assess the links between: 1) parents’ reported behavior, attitudes, and beliefs about child feeding and 2) actual practices in the domain of child feeding.
Perceived Physical Ability
Higher weight status among girls was not associated with lower perceived physical ability. As with perceived cognitive ability, however, higher concern among mothers about their daughter’s weight status was associated with lower perceived physical ability among girls, independent of girls’ weight status. In addition, higher maternal restriction of girls’ access to food was associated with lower perceived physical ability for girls with higher weight status but not for girls with lower weight status. Perhaps mothers who are concerned about their daughter’s weight status communicate lower expectations of their child’s athletic ability as a result of stereotypes concerning overweight and physical activity or because of their child’s lack of interest in physical activity. Mothers who restrict their daughter’s access to food may also strongly encourage their daughters to be physically active, possibly to the point of coercion, in an attempt to promote weight loss. Girls with higher weight status may be more likely to perceive such encouragement as a lack of acceptance in comparison to girls with lower weight status and as a result reject physical activity in general. These possibilities are speculative and require further investigation.
Perceived Peer and Maternal Acceptance
No association was found between girls’ perceived peer and maternal acceptance and girls’ weight status, parental concern, or parental restriction. The absence of a relationship between girls’ weight status and maternal acceptance may be explained by a social desirability bias or by the fact that mothers of girls with higher weight status tended to be overweight themselves (r = .20), reflecting familial patterns in adiposity. Because of similarity in weight status, mothers of overweight girls may be generally accepting of their daughter’s weight status and maintain positive interactions with their daughters. The absence of a relationship between girls’ weight status and girls’ perceived peer acceptance may be explained by the fact that girls had not yet begun school, where peer influence becomes particularly important.
Summary and Conclusions
Previous research has shown that overweight school-aged children and adolescents experience lower self-concept and lower body esteem than do their normal weight peers.8–11 Results from the present study reveal that negative associations between weight status and self-concept are present in girls as young as 5 years of age. In addition, results of the present study extend results of previous research by suggesting that maternal and paternal concern about their daughter’s weight status and mothers’ restriction of daughter’s food intake may have a negative impact on girls’ developing self-evaluations in several domains. It must be kept in mind, however, that the directionality of these results cannot be determined because the data are cross-sectional. It is also possible that low self-concept preceded high weight status or that parents were concerned about their daughter’s weight status and restricted their daughter’s access to food as a result of their daughters being overweight and exhibiting low self-concept. In addition, the results from the present study can only be generalized to reasonably well-educated, non-Hispanic white families. Therefore, additional research with longitudinal data and with more diverse ethnic and socioeconomic status groups is needed to determine the directionality and generalizability of the obtained results.
Regardless of the directionality of effects, findings from the present study are a cause for concern. Low body esteem, perceived cognitive ability, and perceived physical ability among girls may negatively affect their emotional, cognitive, and physical development. Overweight girls who express lower body esteem may be at risk of higher weight concerns and early dieting as a means of improving body satisfaction and/or general self-worth.42,43 Early dieting and excessive weight control practices may result in insufficient caloric intake and the impediment of growth velocity in children. Low perceived cognitive ability among young girls may have implications for future cognitive achievement. Finally, girls with low perceived physical ability may be less likely to participate in sports and general physical activity, which could contribute to positive energy balance and lead to the development or exacerbation of overweight.
With 25% of US children overweight today and with concern about childhood overweight on the rise, findings from the present study suggest that how we deal with children’s overweight may have implications for the psychological health of a considerable proportion of US children. Public health programs that simply raise parental awareness about childhood overweight without providing parents with concrete alternatives for addressing their concerns about their child’s weight status may be harmful. These findings suggest that anticipatory guidance for parents of overweight girls should include information regarding the possible risks of restriction and parental concern and should include constructive messages for parents, that address both sides of the energy balance equation. Unfortunately, the research basis for making specific suggestions is extremely limited. Suggestions could include encouraging family leisure activities that incorporate and promote opportunities for active play for girls but that minimize opportunities for negative evaluation. With respect to messages for parents regarding girls’ food intake, there is evidence that restricted access is not an effective strategy and may be counter productive. Recent research indicates that in addition to being associated with negative self-evaluations in girls, restriction can actually promote intake of restricted, palatable foods and encourage eating in the absence of hunger.44,45 There are a variety of possible alternatives to restriction; research, however, is needed to evaluate their effectiveness. For example, parents could make a wide variety of foods available in the home, with a larger proportion of foods from the bottom of the Food Guide Pyramid, and allow children to make their own food choices. In addition, parents could act as role models to their children in terms of appropriate food choices. Although parent education is essential in the successful prevention and treatment of childhood overweight, a comprehensive solution must also include social, cultural, and economic factors that shape the larger environmental context in which families feed their children.
Acknowledgments
This research was supported by National Institutes of Health Grant RO1 HD 32973.
ABBREVIATIONS
- WHP
weight for height percentile
- PCSA
Pictorial Scale of Perceived Competence and Social Acceptance for Young Children
- GPCS
General Parental Control Scale
References
- 1.Troiano RP, Flegal KM. Overweight children and adolescents: description, epidemiology, and demographics. Pediatrics. 1998;101:497–504. [PubMed] [Google Scholar]
- 2.Ogden CL, Trioano RP, Briefel RR, Kuczmarski RJ, Flegal KM, Johnson CL. Prevalence of overweight among preschool children in the United States. Pediatrics. 1997;99(4) doi: 10.1542/peds.99.4.e1. URL: http://www.pediatrics.org/cgi/content/full/99/4/e1. [DOI] [PubMed] [Google Scholar]
- 3.Dietz WH. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics. 101(3):518–525. [PubMed] [Google Scholar]
- 4.Pinhas-Hamiel O, Dolan LM, Daniels SR, Standiford D, Khoury PR, Zeitler P. Increased incidence of non-insulin diabetes mellitus among adolescents. J Pediatr. 1996;128:608–615. doi: 10.1016/s0022-3476(96)80124-7. [DOI] [PubMed] [Google Scholar]
- 5.Rames LK, Clarke WR, Connor WE, Reiter MA, Lauer RM. Normal blood pressures and the elevation of sustained blood pressure elevation in childhood: the Muscatine Study. Pediatrics. 1978;61:245–251. [PubMed] [Google Scholar]
- 6.Mallory GB, Jr, Fisher D, Jackson R. Sleep-associated breathing disorders in morbidly obese children and adolescents. J Pediatr. 1989;115:892–897. doi: 10.1016/s0022-3476(89)80738-3. [DOI] [PubMed] [Google Scholar]
- 7.Wallace WJ, Sheslow D, Hassink S. Obesity in children: a risk for depression. In: Williams CL, Kimm SYS, editors. Annals of the New York Academy of Science: Prevention and Treatment of Childhood Obesity. New York, NY: New York Academy of Sciences; 1993. pp. 301–302. [DOI] [PubMed] [Google Scholar]
- 8.Hill AJ, Draper E, Stack J. A weight on children’s minds: body shape dissatisfaction at 9 years old. Int J Obes. 1994;18:383–389. [PubMed] [Google Scholar]
- 9.Mendelson BK, White DR. Relation between body-esteem and self-esteem of obese and normal children. Percept Mot Skills. 1982;54:899–905. doi: 10.2466/pms.1982.54.3.899. [DOI] [PubMed] [Google Scholar]
- 10.Banis HT, Varni JW, Wallander JL, et al. Psychological and social adjustment of obese children and their families. Child Care Health Dev. 1988;14:157–173. doi: 10.1111/j.1365-2214.1988.tb00572.x. [DOI] [PubMed] [Google Scholar]
- 11.Kimm SYS, Sweeney CG, Janosky JE, MacMillan JP. Self-concept measures and childhood obesity: a descriptive analysis. Dev Behav Pediatr. 1991;12:19–24. [PubMed] [Google Scholar]
- 12.Brylinskey JA, Moore JC. The identification of body build stereotypes in young children. J Res Person. 1994;28:170–181. [Google Scholar]
- 13.Jarvie GJ, Lahey B, Graziano W, Framer E. Childhood obesity and social stigma: what we know and what we don’t know. Dev Rev. 1983;3:237–273. [Google Scholar]
- 14.Maddox GL, Back K, Liederman V. Overweight as social deviance and disability. J Health Soc Behav. 1968;9:287–298. [PubMed] [Google Scholar]
- 15.Richardson S, Goodman N, Hastorf A, Dornbusch S. Cultural uniformity and reaction to physical disability. Am Soc Rev. 1961;26:241–247. [Google Scholar]
- 16.Marsh HW. Multidimensional, hierarchical self-concept: theoretical and empirical justification. Educ Psychol Rev. 1990;2:77–172. [Google Scholar]
- 17.Braet C, Mervielde I, Vandereycken W. Psychological aspects of childhood obesity: a controlled study in a clinical and non-clinical sample. J Pediatr Psychol. 1997;22:59–71. doi: 10.1093/jpepsy/22.1.59. [DOI] [PubMed] [Google Scholar]
- 18.Mendelson BK, White DR. Development of self-body esteem in overweight youngsters. Dev Psychol. 1985;21:90–96. [Google Scholar]
- 19.Pierce JW, Wardle J. Cause and effect beliefs and self-esteem of overweight children. J Child Psychol Psychiatry. 1997;38:645–650. doi: 10.1111/j.1469-7610.1997.tb01691.x. [DOI] [PubMed] [Google Scholar]
- 20.Sallade J. A comparison of psychological adjustment of obese versus non-obese children. J Psychosom Res. 1973;17:89–96. doi: 10.1016/0022-3999(73)90009-3. [DOI] [PubMed] [Google Scholar]
- 21.Strauss CC, Smith K, Frame C, Forehand R. Personal and interpersonal characteristics associated with childhood obesity. J Pediatr Psychol. 1985;10:337–343. doi: 10.1093/jpepsy/10.3.337. [DOI] [PubMed] [Google Scholar]
- 22.Phillips RG, Hill AJ. Fat, plain, but not friendless: self-esteem and peer acceptance of obese pre-adolescent girls. Int J Obes. 1998;22:287–293. doi: 10.1038/sj.ijo.0800582. [DOI] [PubMed] [Google Scholar]
- 23.Klesges RC, Haddock CK, Stein RJ, Eck LH, Hanson CL, Klesges LM. Relationship between psychosocial functioning and body fat in pre-school children: a longitudinal investigation. J Consult Clin Psychol. 1992;60:793–796. doi: 10.1037//0022-006x.60.5.793. [DOI] [PubMed] [Google Scholar]
- 24.Rumpel C, Harris TB. The influence of weight on adolescent self-esteem. J Psychosom Res. 1994;38:547–556. doi: 10.1016/0022-3999(94)90052-3. [DOI] [PubMed] [Google Scholar]
- 25.Wadden TA, Foster GD, Brownell KD, Finley E. Self-concept in obese and normal-weight children. J Consult Clin Psychol. 1984;52:1104–1105. doi: 10.1037//0022-006x.52.6.1104. [DOI] [PubMed] [Google Scholar]
- 26.Friedman MA, Brownell KD. Psychological correlates of obesity: moving to the next research generation. Psychol Bull. 1985;117:3–20. doi: 10.1037/0033-2909.117.1.3. [DOI] [PubMed] [Google Scholar]
- 27.Keel PK, Fulkerson JA, Leon GR. Disordered eating precursors in pre-and early adolescent girls and boys. J Youth Adolesc. 1997;26:203–217. [Google Scholar]
- 28.Rolland K, Farnill D, Griffiths RA. Children’s perceptions of their current and ideal body sizes and body mass index. Percept Mot Skills. 1996;82:651–656. doi: 10.2466/pms.1996.82.2.651. [DOI] [PubMed] [Google Scholar]
- 29.Wood KC, Becker JA, Thompson JK. Body image dissatisfaction in preadolescent children. J Appl Dev Psychol. 1996;17:85–100. [Google Scholar]
- 30.Lohman TG, Roche AF, Martorell R. Anthropometric Standardization Reference Manual. Campaign, IL: Human Kinetics Publishers Inc; 1988. [Google Scholar]
- 31.Harter S, Pike R. The pictorial scale of perceived competence and social acceptance for young children. Child Dev. 1984;55:1969–1982. [PubMed] [Google Scholar]
- 32.Birch LL, Fisher JO, Castro CN, Grimm-Thomas K, Sawyer R, Johnson S. Confirmatory factor analysis of the Child Feeding Questionnaire: a measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. doi: 10.1006/appe.2001.0398. Under review. [DOI] [PubMed] [Google Scholar]
- 33.Baumrind D. Current patterns of parental authority. Dev Psychol Monogr. 1971;4:1. [Google Scholar]
- 34.Himes JH, Dietz WH. Guidelines for overweight in adolescent preventive services: recommendations from an expert committee. Am J Clin Nutr. 1994;59:307–316. doi: 10.1093/ajcn/59.2.307. [DOI] [PubMed] [Google Scholar]
- 35.Feldman W, Feldman E, Goodman JT. Culture versus biology: children’s attitudes toward fatness and thinness. Pediatrics. 1988;81:190–194. [PubMed] [Google Scholar]
- 36.Sylvester GP, Achterberg C, Williams J. Children’s television and nutrition: friends or foes? Nutr Today. 1995;30:6–15. [Google Scholar]
- 37.Catterin J, Thompson JK. A three-year longitudinal study of body image, eating disturbances, and general psychological functioning in adolescent females. Eat Dis J Treat Prev. 1994;2:114–125. [Google Scholar]
- 38.Katz PA, Walsh V. Modification of children’s gender-stereotypical behavior. Child Dev. 1991;62:338–351. [Google Scholar]
- 39.Maccoby EE, Jacklin CN. The Psychology of Sex Differences. Stanford, CA: Stanford University Press; 1974. [Google Scholar]
- 40.Radin N, Sagi A. Childrearing fathers in intact families in Israel and the USA. Merrill-Palmer Q. 1982;28:111–136. [Google Scholar]
- 41.Burt JV, Hertzler AA. Parental influence on the child’s food preference. J Nutr Educ. 1978;10:127–130. [Google Scholar]
- 42.Hill AJ, Paulin V. Dieting awareness and low self-worth: related issues in 8-year-old girls. Int J Eat Dis. 1998;24:405–413. doi: 10.1002/(sici)1098-108x(199812)24:4<405::aid-eat7>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 43.Neumark-Sztainer D, Butler R, Palti H. Persistence of weight loss behaviors among adolescent girls in Jerusalem. Int J Adolesc Med Health. 1997;91:19–35. doi: 10.1515/IJAMH.1997.9.1.19. [DOI] [PubMed] [Google Scholar]
- 44.Fisher JO, Birch LL. Restricting access to a palatable food affects children’s behavioral response, food selection, and intake. Am J Clin Nutr. 1999a;69:1264–1272. doi: 10.1093/ajcn/69.6.1264. [DOI] [PubMed] [Google Scholar]
- 45.Fisher JO, Birch LL. Restricting access to foods and children’s eating. Appetite. 1999b;32:405–419. doi: 10.1006/appe.1999.0231. [DOI] [PubMed] [Google Scholar]