

Abstract
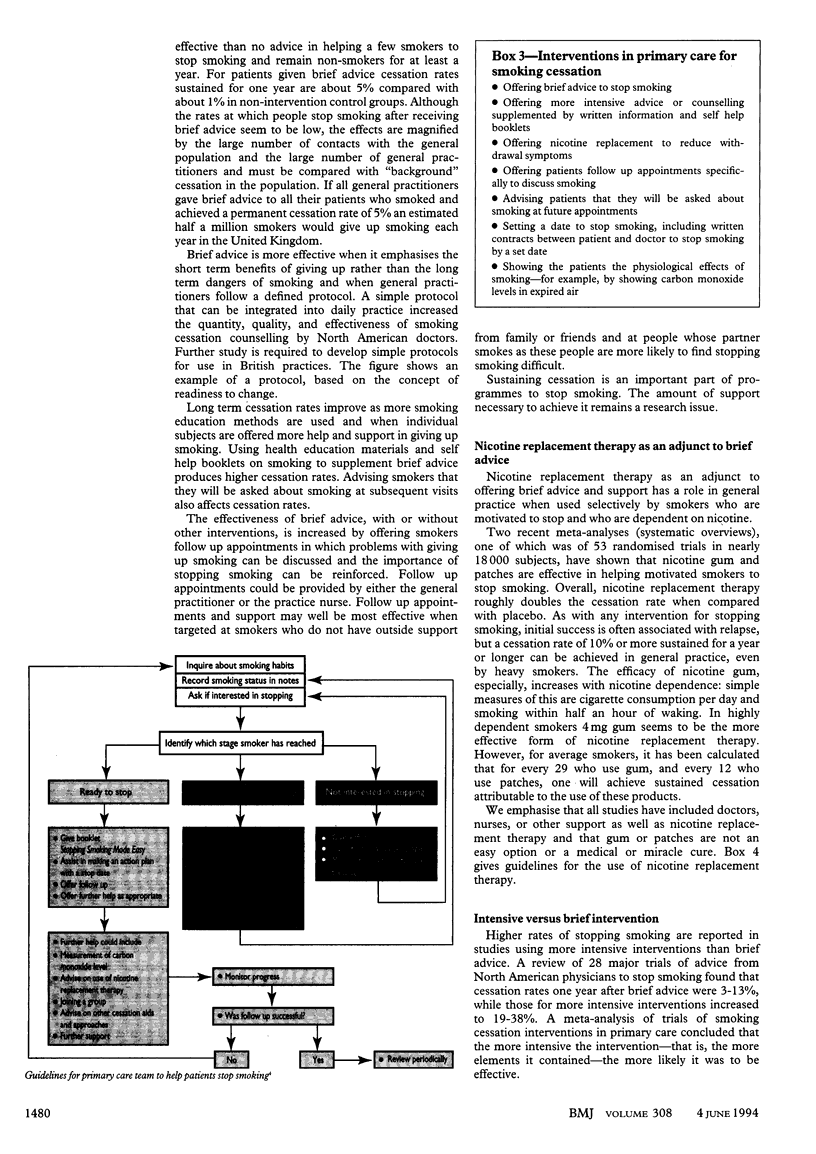
Smoking is the single most important cause of cancer. The risk of developing cancer is reduced by stopping smoking and decreases substantially after five years. Reduction in smoking must be central to any programme aimed seriously at the prevention of cancer. An individual approach, based in primary care, has the potential to bring about modest but important reductions in risk. Many randomised trials have shown the effectiveness of various smoking cessation interventions in primary care. Given resource limitations in primary care, individual effort should be focused on those at highest risk who are motivated to stop smoking. A population strategy has considerable advantages over the high risk approach as the potential for reducing morbidity and mortality in the whole population is much greater. The government must acknowledge its major responsibility; the outstanding example of its failure to do this is its persistent refusal to ban outright all forms of advertising and promotion of tobacco. There is clear evidence that a ban would contribute to a reduction in smoking prevalence and especially in the uptake of smoking by children.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- DiClemente C. C., Prochaska J. O., Fairhurst S. K., Velicer W. F., Velasquez M. M., Rossi J. S. The process of smoking cessation: an analysis of precontemplation, contemplation, and preparation stages of change. J Consult Clin Psychol. 1991 Apr;59(2):295–304. doi: 10.1037//0022-006x.59.2.295. [DOI] [PubMed] [Google Scholar]
- Frey G. H. Use of aspartame by apparently healthy children and adolescents. J Toxicol Environ Health. 1976 Nov;2(2):401–415. doi: 10.1080/15287397609529442. [DOI] [PubMed] [Google Scholar]
- Kottke T. E., Battista R. N., DeFriese G. H., Brekke M. L. Attributes of successful smoking cessation interventions in medical practice. A meta-analysis of 39 controlled trials. JAMA. 1988 May 20;259(19):2883–2889. doi: 10.1001/jama.259.19.2883. [DOI] [PubMed] [Google Scholar]
- Schiffman S. S., Buckley C. E., 3rd, Sampson H. A., Massey E. W., Baraniuk J. N., Follett J. V., Warwick Z. S. Aspartame and susceptibility to headache. N Engl J Med. 1987 Nov 5;317(19):1181–1185. doi: 10.1056/NEJM198711053171903. [DOI] [PubMed] [Google Scholar]
- Silagy C., Mant D., Fowler G., Lodge M. Meta-analysis on efficacy of nicotine replacement therapies in smoking cessation. Lancet. 1994 Jan 15;343(8890):139–142. doi: 10.1016/s0140-6736(94)90933-4. [DOI] [PubMed] [Google Scholar]
- Tang J. L., Law M., Wald N. How effective is nicotine replacement therapy in helping people to stop smoking? BMJ. 1994 Jan 1;308(6920):21–26. doi: 10.1136/bmj.308.6920.21. [DOI] [PMC free article] [PubMed] [Google Scholar]