

Abstract
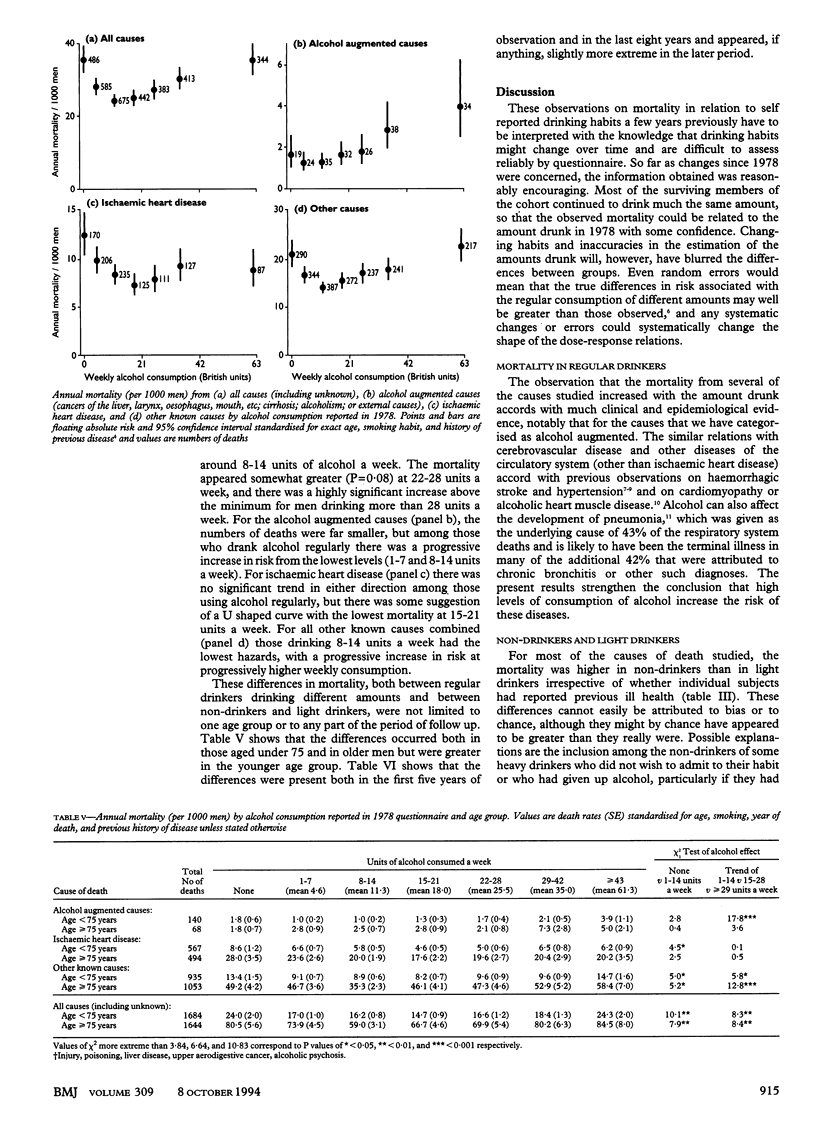
OBJECTIVE--To assess the risk of death associated with various patterns of alcohol consumption. DESIGN--Prospective study of mortality in relation to alcohol drinking habits in 1978, with causes of death sought over the next 13 years (to 1991). SUBJECTS--12,321 British male doctors born between 1900 and 1930 (mean 1916) who replied to a postal questionnaire in 1978. Those written to in 1978 were the survivors of a long running prospective study of the effects of smoking that had begun in 1951 and was still continuing. RESULTS--Men were divided on the basis of their response to the 1978 questionnaire into two groups according to whether or not they had ever had any type of vascular disease, diabetes, or "life threatening disease" and into seven groups according to the amount of alcohol they drank. By 1991 almost a third had died. All statistical analyses of mortality were standardised for age, calendar year, and smoking habit. There was a U shaped relation between all cause mortality and the average amount of alcohol reportedly drunk; those who reported drinking 8-14 units of alcohol a week (corresponding to an average of one to two units a day) had the lowest risks. The causes of death were grouped into three main categories: "alcohol augmented" causes (6% of all deaths: cirrhosis, liver cancer, upper aerodigestive (mouth, oesophagus, larynx, and pharynx) cancer, alcoholism, poisoning, or injury), ischaemic heart disease (33% of all deaths), and other causes. The few deaths from alcohol augmented causes showed, at least among regular drinkers, a progressive trend, with the risk increasing with dose. In contrast, the many deaths from ischaemic heart disease showed no significant trend among regular drinkers, but there were significantly lower rates in regular drinkers than in non-drinkers. The aggregate of all other causes showed a U shaped dose-response relation similar to that for all cause mortality. Similar differences persisted irrespective of a history of previous disease, age (under 75 or 75 and older), and period of follow up (first five and last eight years). Some, but apparently not much, of the excess mortality in non-drinkers could be attributed to the inclusion among them of a small proportion of former drinkers. CONCLUSION--The consumption of alcohol appeared to reduce the risk of ischaemic heart disease, largely irrespective of amount. Among regular drinkers mortality from all causes combined increased progressively with amount drunk above 21 units a week. Among British men in middle or older age the consumption of an average of one or two units of alcohol a day is associated with significantly lower all cause mortality than is the consumption of no alcohol, or the consumption of substantial amounts. Above about three units (two American units) of alcohol a day, progressively greater levels of consumption are associated with progressively higher all cause mortality.
Full text
PDF




Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Beaglehole R., Jackson R. Alcohol, cardiovascular diseases and all causes of death: a review of the epidemiological evidence. Drug Alcohol Rev. 1992;11(3):275–289. doi: 10.1080/09595239200185811. [DOI] [PubMed] [Google Scholar]
- Boffetta P., Garfinkel L. Alcohol drinking and mortality among men enrolled in an American Cancer Society prospective study. Epidemiology. 1990 Sep;1(5):342–348. doi: 10.1097/00001648-199009000-00003. [DOI] [PubMed] [Google Scholar]
- Colditz G. A., Branch L. G., Lipnick R. J., Willett W. C., Rosner B., Posner B., Hennekens C. H. Moderate alcohol and decreased cardiovascular mortality in an elderly cohort. Am Heart J. 1985 Apr;109(4):886–889. doi: 10.1016/0002-8703(85)90654-4. [DOI] [PubMed] [Google Scholar]
- Doll R., Peto R., Wheatley K., Gray R., Sutherland I. Mortality in relation to smoking: 40 years' observations on male British doctors. BMJ. 1994 Oct 8;309(6959):901–911. doi: 10.1136/bmj.309.6959.901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Easton D. F., Peto J., Babiker A. G. Floating absolute risk: an alternative to relative risk in survival and case-control analysis avoiding an arbitrary reference group. Stat Med. 1991 Jul;10(7):1025–1035. doi: 10.1002/sim.4780100703. [DOI] [PubMed] [Google Scholar]
- Farchi G., Fidanza F., Mariotti S., Menotti A. Alcohol and mortality in the Italian rural cohorts of the Seven Countries Study. Int J Epidemiol. 1992 Feb;21(1):74–81. doi: 10.1093/ije/21.1.74. [DOI] [PubMed] [Google Scholar]
- Grønbaek M., Deis A., Sørensen T. I., Becker U., Borch-Johnsen K., Müller C., Schnohr P., Jensen G. Influence of sex, age, body mass index, and smoking on alcohol intake and mortality. BMJ. 1994 Jan 29;308(6924):302–306. doi: 10.1136/bmj.308.6924.302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haskell W. L., Camargo C., Jr, Williams P. T., Vranizan K. M., Krauss R. M., Lindgren F. T., Wood P. D. The effect of cessation and resumption of moderate alcohol intake on serum high-density-lipoprotein subfractions. A controlled study. N Engl J Med. 1984 Mar 29;310(13):805–810. doi: 10.1056/NEJM198403293101301. [DOI] [PubMed] [Google Scholar]
- Hendriks H. F., Veenstra J., Velthuis-te Wierik E. J., Schaafsma G., Kluft C. Effect of moderate dose of alcohol with evening meal on fibrinolytic factors. BMJ. 1994 Apr 16;308(6935):1003–1006. doi: 10.1136/bmj.308.6935.1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jarvis M. J. A profile of tobacco smoking. Addiction. 1994 Nov;89(11):1371–1376. doi: 10.1111/j.1360-0443.1994.tb03732.x. [DOI] [PubMed] [Google Scholar]
- MacMahon S., Peto R., Cutler J., Collins R., Sorlie P., Neaton J., Abbott R., Godwin J., Dyer A., Stamler J. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet. 1990 Mar 31;335(8692):765–774. doi: 10.1016/0140-6736(90)90878-9. [DOI] [PubMed] [Google Scholar]
- Marmot M. G., Elliott P., Shipley M. J., Dyer A. R., Ueshima H., Beevers D. G., Stamler R., Kesteloot H., Rose G., Stamler J. Alcohol and blood pressure: the INTERSALT study. BMJ. 1994 May 14;308(6939):1263–1267. doi: 10.1136/bmj.308.6939.1263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marmot M., Brunner E. Alcohol and cardiovascular disease: the status of the U shaped curve. BMJ. 1991 Sep 7;303(6802):565–568. doi: 10.1136/bmj.303.6802.565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meade T. W., Imeson J., Stirling Y. Effects of changes in smoking and other characteristics on clotting factors and the risk of ischaemic heart disease. Lancet. 1987 Oct 31;2(8566):986–988. doi: 10.1016/s0140-6736(87)92556-6. [DOI] [PubMed] [Google Scholar]
- Preedy V. R., Richardson P. J. Ethanol induced cardiovascular disease. Br Med Bull. 1994 Jan;50(1):152–163. doi: 10.1093/oxfordjournals.bmb.a072873. [DOI] [PubMed] [Google Scholar]
- Renaud S., de Lorgeril M. Wine, alcohol, platelets, and the French paradox for coronary heart disease. Lancet. 1992 Jun 20;339(8808):1523–1526. doi: 10.1016/0140-6736(92)91277-f. [DOI] [PubMed] [Google Scholar]
- Rimm E. B., Giovannucci E. L., Willett W. C., Colditz G. A., Ascherio A., Rosner B., Stampfer M. J. Prospective study of alcohol consumption and risk of coronary disease in men. Lancet. 1991 Aug 24;338(8765):464–468. doi: 10.1016/0140-6736(91)90542-w. [DOI] [PubMed] [Google Scholar]
- Shaper A. G., Wannamethee G., Walker M. Alcohol and coronary heart disease: a perspective from the British Regional Heart Study. Int J Epidemiol. 1994 Jun;23(3):482–494. doi: 10.1093/ije/23.3.482. [DOI] [PubMed] [Google Scholar]