

Abstract
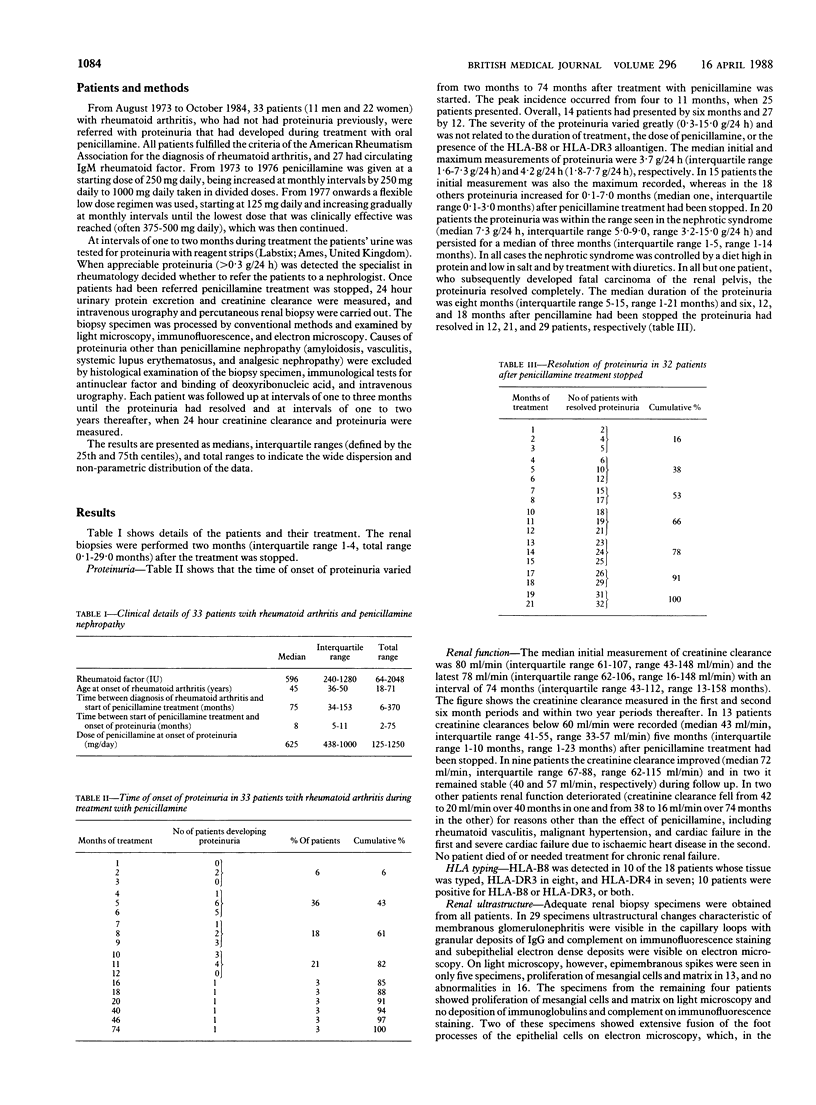
To elucidate the natural course of the nephropathy associated with penicillamine and thereby facilitate its clinical management 33 patients with rheumatoid arthritis who developed proteinuria during treatment with oral penicillamine were studied in detail throughout their renal illness. Renal biopsies were performed, and creatinine clearance and proteinuria were measured serially for 74 months (range 16-148 months). Fourteen patients developed proteinuria within six months after the start of treatment and 27 within 12 months. When treatment was stopped the proteinuria reached a median peak of 4·2 g/24 h (range 0·3-15·0 g/24 h) at one month (range 0-7 months) before resolving spontaneously by six months (12 patients), 12 months (21), or 18 months (29). In all patients but one, who developed carcinoma of the renal pelvis, proteinuria resolved by 21 months and its median duration was eight months. The median first and last measurements of creatinine clearance showed no appreciable change (80 ml/min and 78 ml/min), and no patient died from or needed treatment for renal failure. The HLA-B8 or HLA-DR3 alloantigen, or both, were identified in 10 patients. Renal biopsy specimens showed membranous glomerulonephritis in 29 patients, minimal change nephropathy in two, and electron dense deposits in the mesangial regions in two.
In all the patients whose nephropathy was due solely to treatment with penicillamine the proteinuria resolved completely when the drug was withdrawn; renal function did not deteriorate, and corticosteroids were unnecessary.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bacon P. A., Tribe C. R., Mackenzie J. C., Verrier-Jones J., Cumming R. H., Amer B. Penicillamine nephropathy in rheumatoid arthritis. A clinical, pathological and immunological study. Q J Med. 1976 Oct;45(180):661–684. [PubMed] [Google Scholar]
- Davison A. M., Day A. T., Golding J. R., Thomson D. Effect of penicillamine on the kidney. Proc R Soc Med. 1977;70 (Suppl 3):109–113. [PMC free article] [PubMed] [Google Scholar]
- Day A. T., Golding J. R., Lee P. N., Butterworth A. D. Penicillamine in rheumatoid disease: a long-term study. Br Med J. 1974 Feb 2;1(5900):180–183. doi: 10.1136/bmj.1.5900.180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dische F. E., Swinson D. R., Hamilton E. B., Parsons V. Immunopathology of penicillamine-induced glomerular disease. J Rheumatol. 1976 Jun;3(2):145–154. [PubMed] [Google Scholar]
- Gibson T., Burry H. C., Ogg C. Letter: Goodpasture syndrome and D-penicillamine. Ann Intern Med. 1976 Jan;84(1):100–100. doi: 10.7326/0003-4819-84-1-100_1. [DOI] [PubMed] [Google Scholar]
- Golding J. R., Day A. T., Tomlinson M. R., Brown R. M., Hassan M. O., Langstaff S. R. Rheumatoid arthritis treated with small doses of penicillamine. Proc R Soc Med. 1977;70 (Suppl 3):131–135. [PMC free article] [PubMed] [Google Scholar]
- Hill H. F., Hill A. G., Day A. T., Brown R. M., Golding J. R., Lyle W. H. Maintenance dose of penicillamine in rheumatoid arthritis: a comparison between a standard and a response-related flexible regimen. Ann Rheum Dis. 1979 Oct;38(5):429–433. doi: 10.1136/ard.38.5.429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Honkanen E., Törnroth T., Pettersson E., Skrifvars B. Membranous glomerulonephritis in rheumatoid arthritis not related to gold or D-penicillamine therapy: a report of four cases and review of the literature. Clin Nephrol. 1987 Feb;27(2):87–93. [PubMed] [Google Scholar]
- Jaffe I. A. Penicillamine in rheumatoid arthritis: clinical pharmacology and biochemical properties. Scand J Rheumatol Suppl. 1979;(28):58–64. doi: 10.3109/03009747909108238. [DOI] [PubMed] [Google Scholar]
- Kirby J. D., Dieppe P. A., Huskisson E. C., Smith B. D-penicillamine and immune complex deposition. Ann Rheum Dis. 1979 Aug;38(4):344–346. doi: 10.1136/ard.38.4.344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neild G. H., Gärtner H. V., Bohle A. Letter: D-penicillamine-induced membranous glomerulonephritis. Lancet. 1975 May 24;1(7917):1201–1202. doi: 10.1016/s0140-6736(75)93197-9. [DOI] [PubMed] [Google Scholar]
- Ross J. H., McGinty F., Brewer D. G. Penicillamine nephropathy. Nephron. 1980;26(4):184–186. doi: 10.1159/000181984. [DOI] [PubMed] [Google Scholar]
- Samuels B., Lee J. C., Engleman E. P., Hopper J., Jr Membranous nephropathy in patients with rheumatoid arthritis: relationship to gold therapy. Medicine (Baltimore) 1978 Jul;57(4):319–327. doi: 10.1097/00005792-197807000-00003. [DOI] [PubMed] [Google Scholar]
- Stephens A. D. The management of cystinuria in 1976. Proc R Soc Med. 1977;70 (Suppl 3):24–26. [PMC free article] [PubMed] [Google Scholar]
- Wooley P. H., Griffin J., Panayi G. S., Batchelor J. R., Welsh K. I., Gibson T. J. HLA-DR antigens and toxic reaction to sodium aurothiomalate and D-penicillamine in patients with rheumatoid arthritis. N Engl J Med. 1980 Aug 7;303(6):300–302. doi: 10.1056/NEJM198008073030602. [DOI] [PubMed] [Google Scholar]