

Abstract
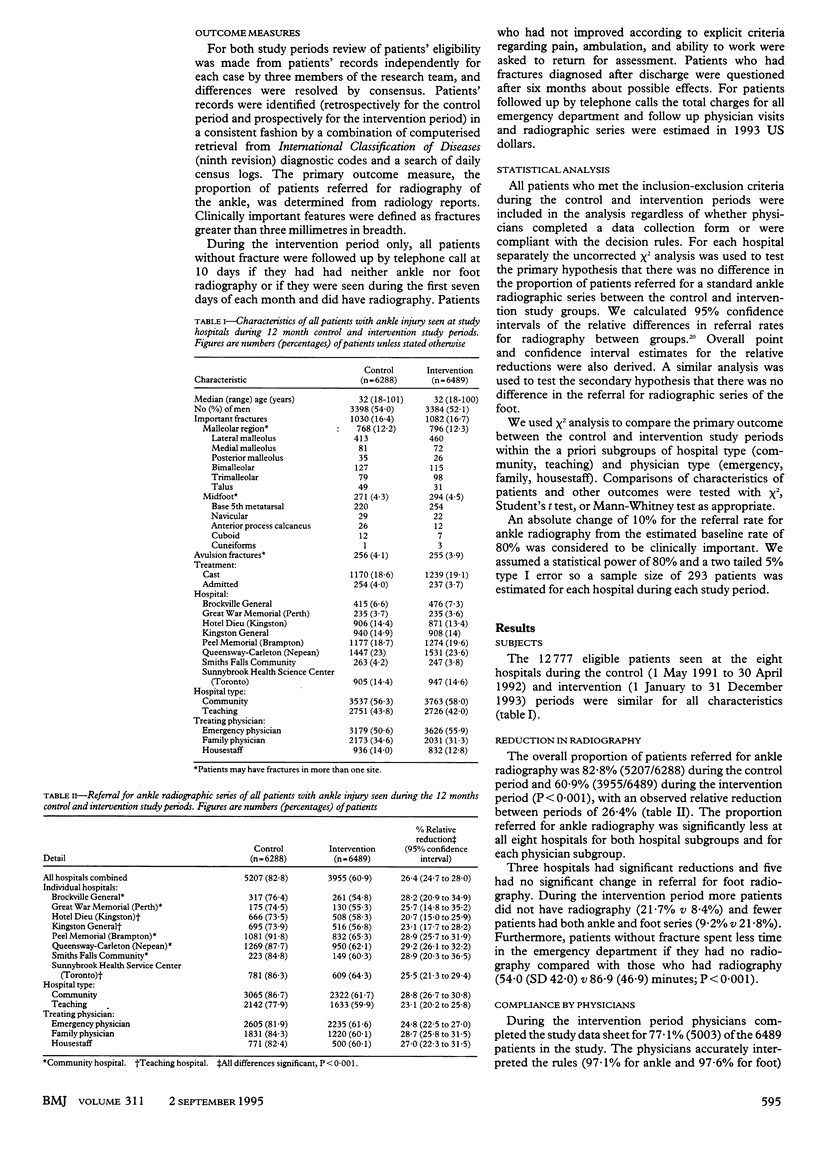
OBJECTIVE--To assess the feasibility and impact of introducing the Ottawa ankle rules to a large number of physicians in a wide variety of hospital and community settings over a prolonged period of time. DESIGN--Multicentre before and after controlled clinical trial. SETTING--Emergency departments of eight teaching and community hospitals in Canadian communities (population 10,000 to 3,000,000). SUBJECTS--All 12,777 adults (6288 control, 6489 intervention) seen with acute ankle injuries during two 12 month periods before and after the intervention. INTERVENTION--More than 200 physicians of varying experience were taught to order radiography according to the Ottawa ankle rules. MAIN OUTCOME MEASURES--Referral for ankle and foot radiography. RESULTS--There were significant reductions in use of ankle radiography at all eight hospitals and within a priori subgroups: for all hospitals combined 82.8% control v 60.9% intervention(P < 0.001); for community hospitals 86.7% v 61.7%; (P < 0.001); for teaching hospitals 77.9% v 59.9%; (P < 0.001); for emergency physicians 82.1% v 61.6%; (P < 0.001); for family physicians 84.3% v 60.1%; (P < 0.001); and for housestaff 82.3% v 60.1%; (P < 0.001). Compared with patients without fracture who had radiography during the intervention period those who had no radiography spent less time in the emergency department (54.0 v 86.9 minutes; P < 0.001) and had lower medical charges ($70.20 v $161.60; P < 0.001). There was no difference in the rate of fractures diagnosed after discharge from the emergency department (0.5 v 0.4%). CONCLUSIONS--Introduction of the Ottawa ankle rules proved to be feasible in a large variety of hospital and community settings. Use of the rules over a prolonged period of time by many physicians of varying experience led to a decrease in ankle radiography, waiting times, and costs without an increased rate of missed fractures. The multiphase methodological approach used to develop and implement these rules may be applied to other clinical problems.
Full text
PDF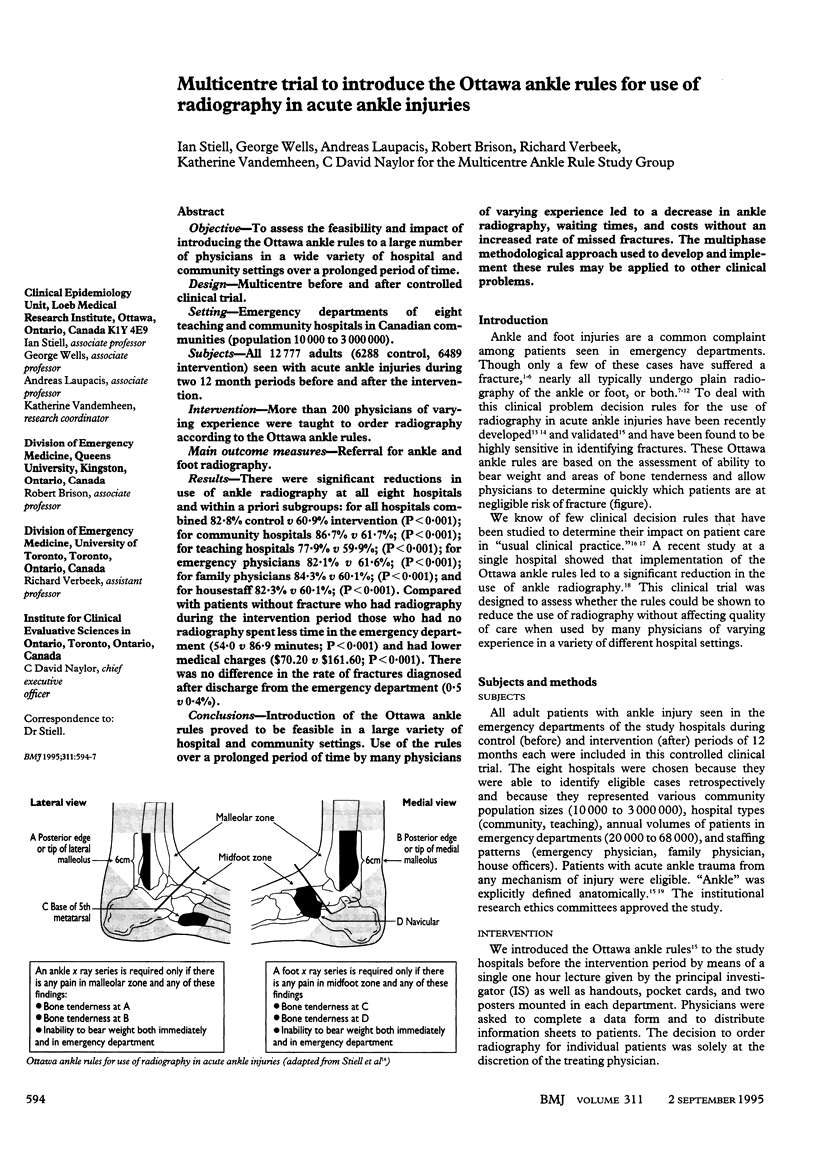


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson G. Implementing practice guidelines. CMAJ. 1993 Mar 1;148(5):753–755. [PMC free article] [PubMed] [Google Scholar]
- Angell M. Cost containment and the physician. JAMA. 1985 Sep 6;254(9):1203–1207. [PubMed] [Google Scholar]
- Brand D. A., Frazier W. H., Kohlhepp W. C., Shea K. M., Hoefer A. M., Ecker M. D., Kornguth P. J., Pais M. J., Light T. R. A protocol for selecting patients with injured extremities who need x-rays. N Engl J Med. 1982 Feb 11;306(6):333–339. doi: 10.1056/NEJM198202113060604. [DOI] [PubMed] [Google Scholar]
- Brooks S. C., Potter B. T., Rainey J. B. Inversion injuries of the ankle: clinical assessment and radiographic review. Br Med J (Clin Res Ed) 1981 Feb 21;282(6264):607–608. doi: 10.1136/bmj.282.6264.607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diehr P., Highley R., Dehkordi F., Wood R., Krueger L., Teitz C., Hermanson B. Prediction of fracture in patients with acute musculoskeletal ankle trauma. Med Decis Making. 1988 Jan-Mar;8(1):40–47. doi: 10.1177/0272989X8800800106. [DOI] [PubMed] [Google Scholar]
- Dunlop M. G., Beattie T. F., White G. K., Raab G. M., Doull R. I. Guidelines for selective radiological assessment of inversion ankle injuries. Br Med J (Clin Res Ed) 1986 Sep 6;293(6547):603–605. doi: 10.1136/bmj.293.6547.603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feinstein A. R. The 'chagrin factor' and qualitative decision analysis. Arch Intern Med. 1985 Jul;145(7):1257–1259. [PubMed] [Google Scholar]
- Gleadhill D. N., Thomson J. Y., Simms P. Can more efficient use be made of x ray examinations in the accident and emergency department? Br Med J (Clin Res Ed) 1987 Apr 11;294(6577):943–947. doi: 10.1136/bmj.294.6577.943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayward R. S., Laupacis A. Initiating, conducting and maintaining guidelines development programs. CMAJ. 1993 Feb 15;148(4):507–512. [PMC free article] [PubMed] [Google Scholar]
- Lee T. H. Evaluating decision aids: the next painful step. J Gen Intern Med. 1990 Nov-Dec;5(6):528–529. doi: 10.1007/BF02600886. [DOI] [PubMed] [Google Scholar]
- Long A. E. Radiographic decision-making by the emergency physician. Emerg Med Clin North Am. 1985 Aug;3(3):437–446. [PubMed] [Google Scholar]
- McCaig L. F. National Hospital Ambulatory Medical Care Survey: 1992 emergency department summary. Adv Data. 1994 Mar 2;(245):1–12. [PubMed] [Google Scholar]
- Moloney T. W., Rogers D. E. Medical technology -- a different view of the contentious debate over costs. N Engl J Med. 1979 Dec 27;301(26):1413–1419. doi: 10.1056/NEJM197912273012603. [DOI] [PubMed] [Google Scholar]
- Montague A. P., McQuillan R. F. Clinical assessment of apparently sprained ankle and detection of fracture. Injury. 1985 Sep;16(8):545–546. doi: 10.1016/0020-1383(85)90082-8. [DOI] [PubMed] [Google Scholar]
- Standards, guidelines and clinical policies. Health Services Research Group. CMAJ. 1992 Mar 15;146(6):833–837. [PMC free article] [PubMed] [Google Scholar]
- Stiell I. G., Greenberg G. H., McKnight R. D., Nair R. C., McDowell I., Reardon M., Stewart J. P., Maloney J. Decision rules for the use of radiography in acute ankle injuries. Refinement and prospective validation. JAMA. 1993 Mar 3;269(9):1127–1132. doi: 10.1001/jama.269.9.1127. [DOI] [PubMed] [Google Scholar]
- Stiell I. G., Greenberg G. H., McKnight R. D., Nair R. C., McDowell I., Worthington J. R. A study to develop clinical decision rules for the use of radiography in acute ankle injuries. Ann Emerg Med. 1992 Apr;21(4):384–390. doi: 10.1016/s0196-0644(05)82656-3. [DOI] [PubMed] [Google Scholar]
- Stiell I. G., McDowell I., Nair R. C., Aeta H., Greenberg G., McKnight R. D., Ahuja J. Use of radiography in acute ankle injuries: physicians' attitudes and practice. CMAJ. 1992 Dec 1;147(11):1671–1678. [PMC free article] [PubMed] [Google Scholar]
- Stiell I. G., McKnight R. D., Greenberg G. H., McDowell I., Nair R. C., Wells G. A., Johns C., Worthington J. R. Implementation of the Ottawa ankle rules. JAMA. 1994 Mar 16;271(11):827–832. [PubMed] [Google Scholar]
- Stiell I. G., McKnight R. D., Greenberg G. H., Nair R. C., McDowell I., Wallace G. J. Interobserver agreement in the examination of acute ankle injury patients. Am J Emerg Med. 1992 Jan;10(1):14–17. doi: 10.1016/0735-6757(92)90117-g. [DOI] [PubMed] [Google Scholar]
- Stother I. G. Incidence of minor fractures in twisting injuries of the ankle. Injury. 1974 Feb;5(3):213–214. doi: 10.1016/s0020-1383(74)80007-0. [DOI] [PubMed] [Google Scholar]
- Sujitkumar P., Hadfield J. M., Yates D. W. Sprain or fracture? An analysis of 2000 ankle injuries. Arch Emerg Med. 1986 Jun;3(2):101–106. doi: 10.1136/emj.3.2.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vargish T., Clarke W. R., Young R. A., Jensen A. The ankle injury--indications for the selective use of X-rays. Injury. 1983 May;14(6):507–512. doi: 10.1016/0020-1383(83)90053-0. [DOI] [PubMed] [Google Scholar]
- Wasson J. H., Sox H. C., Neff R. K., Goldman L. Clinical prediction rules. Applications and methodological standards. N Engl J Med. 1985 Sep 26;313(13):793–799. doi: 10.1056/NEJM198509263131306. [DOI] [PubMed] [Google Scholar]