

Abstract
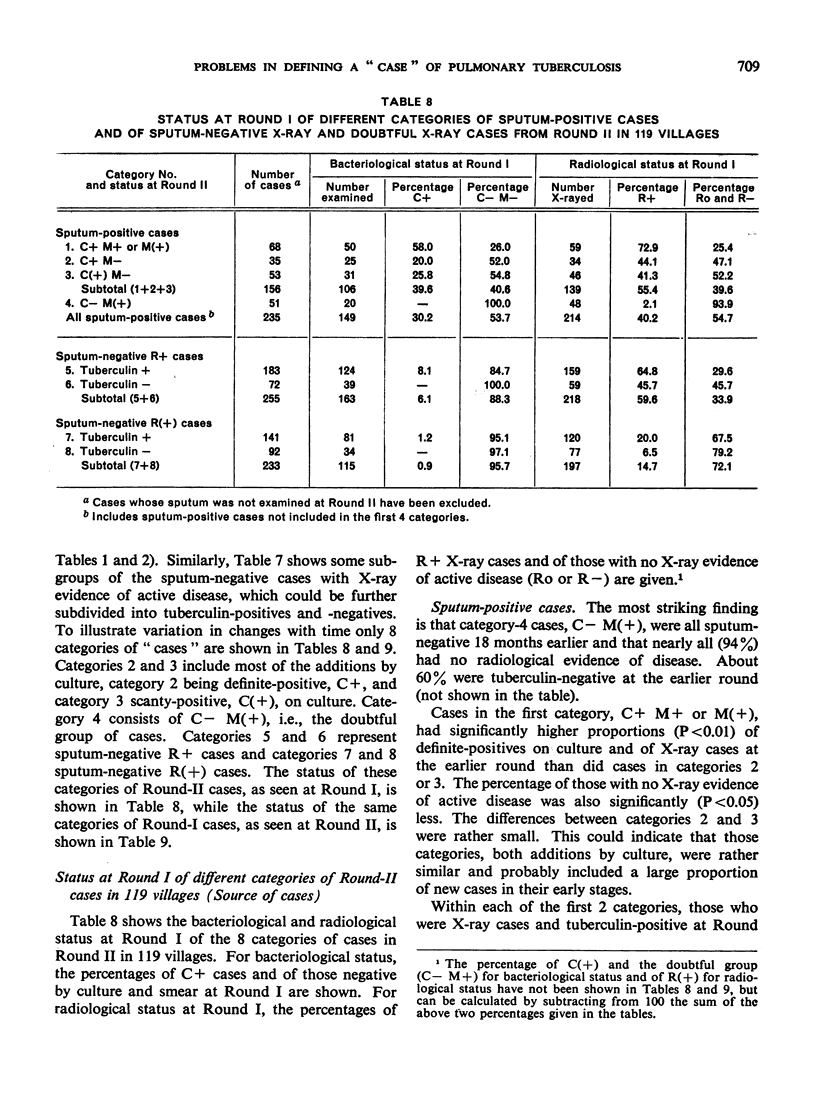
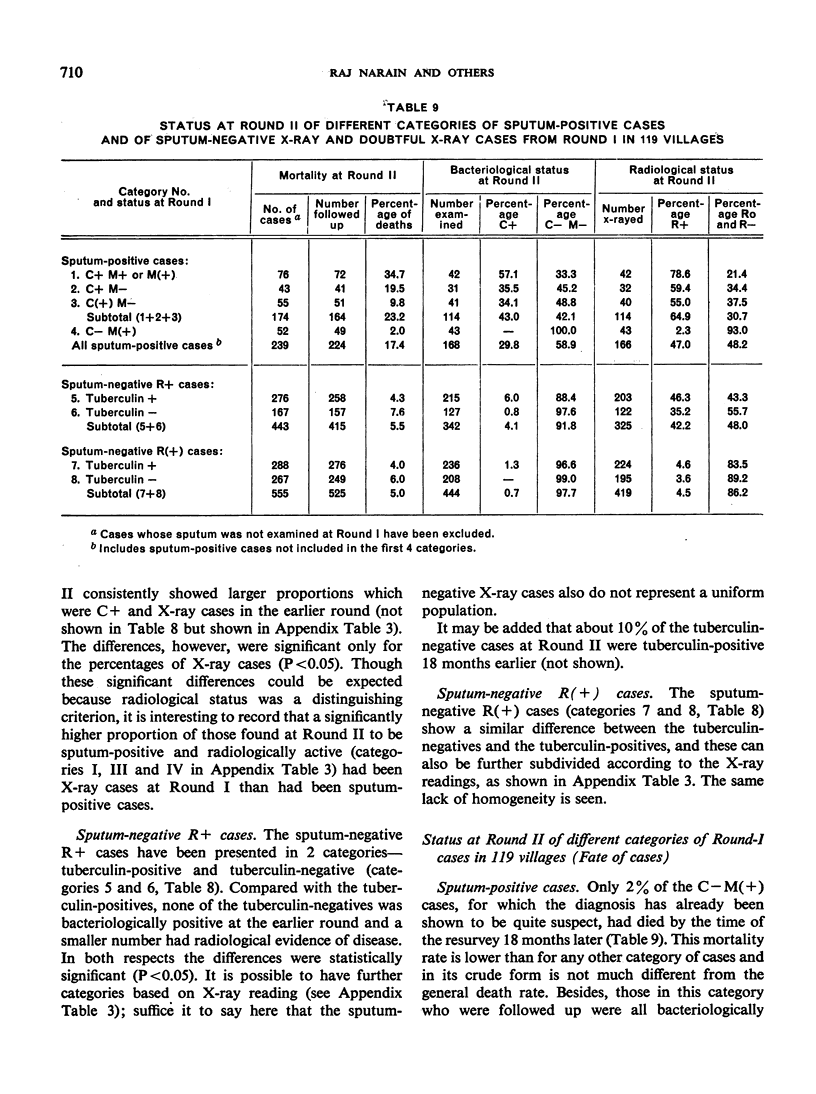
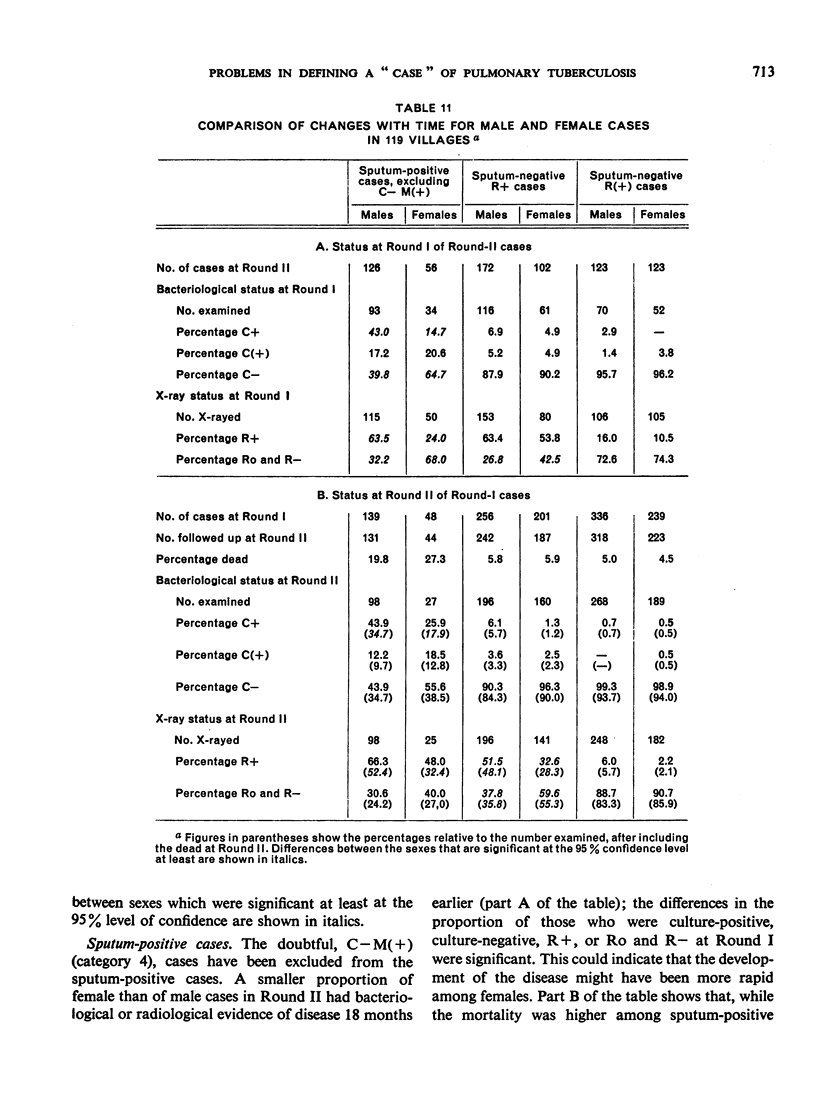
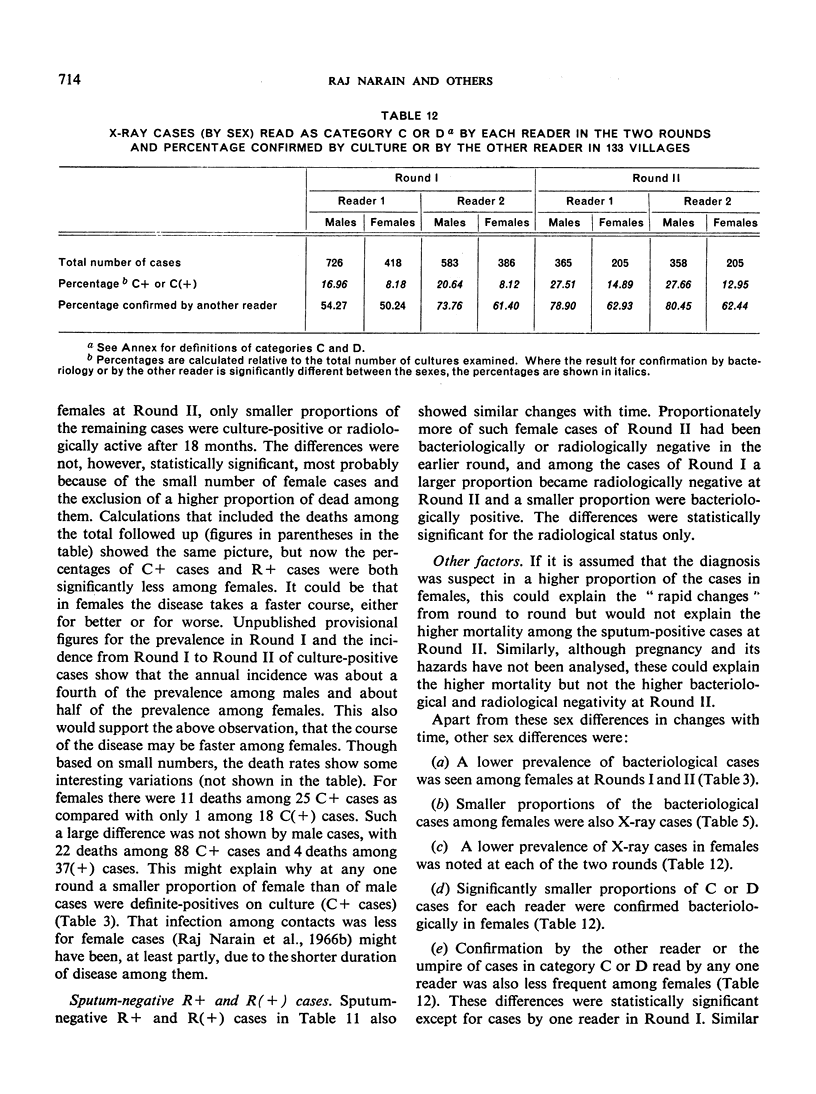
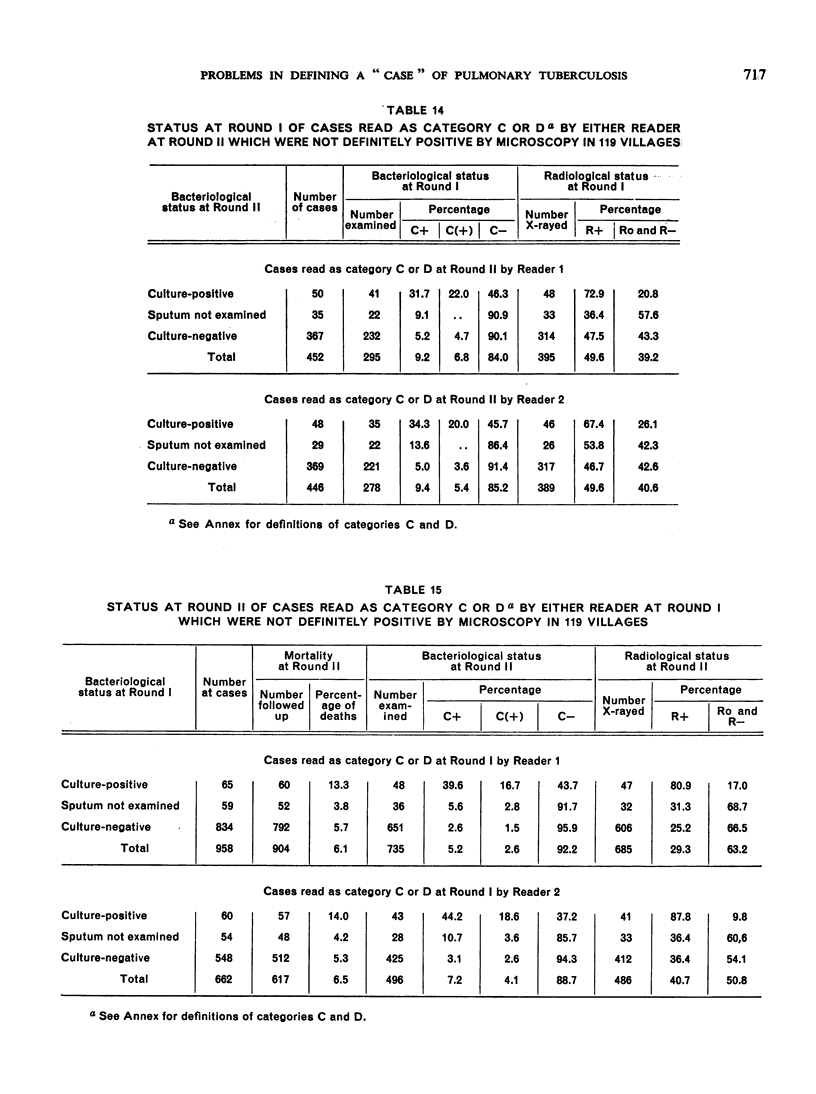
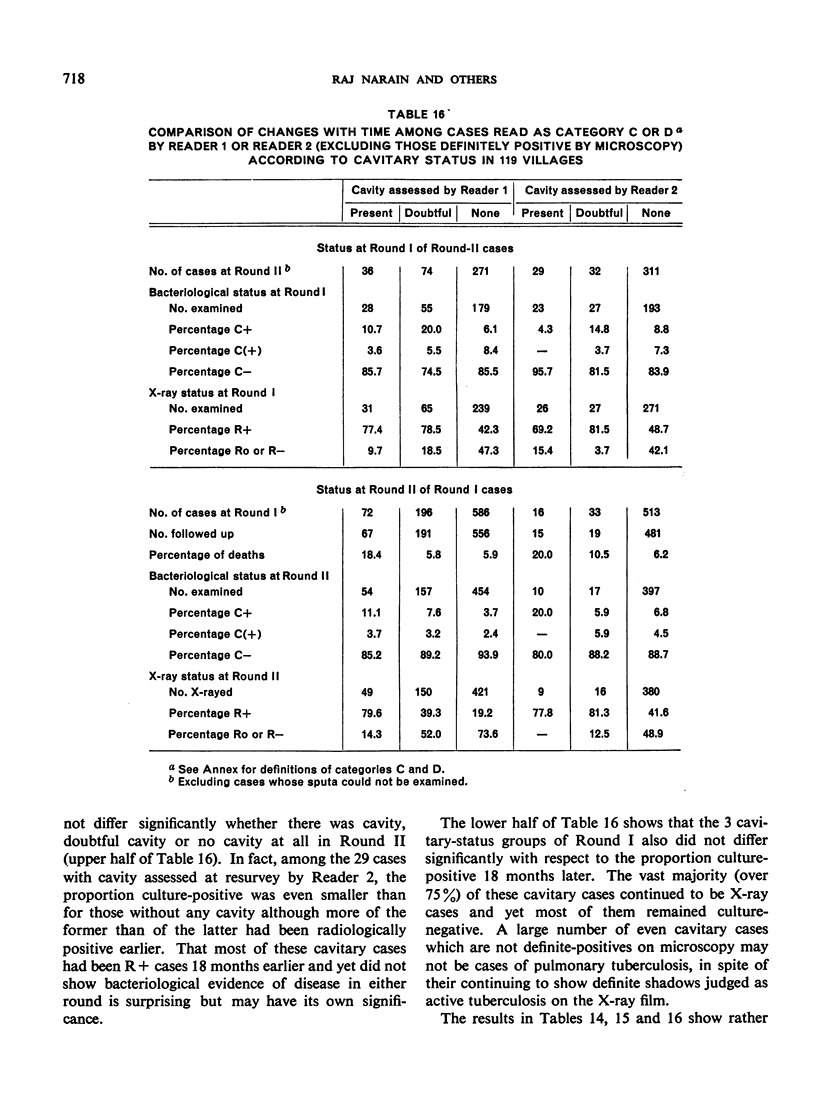
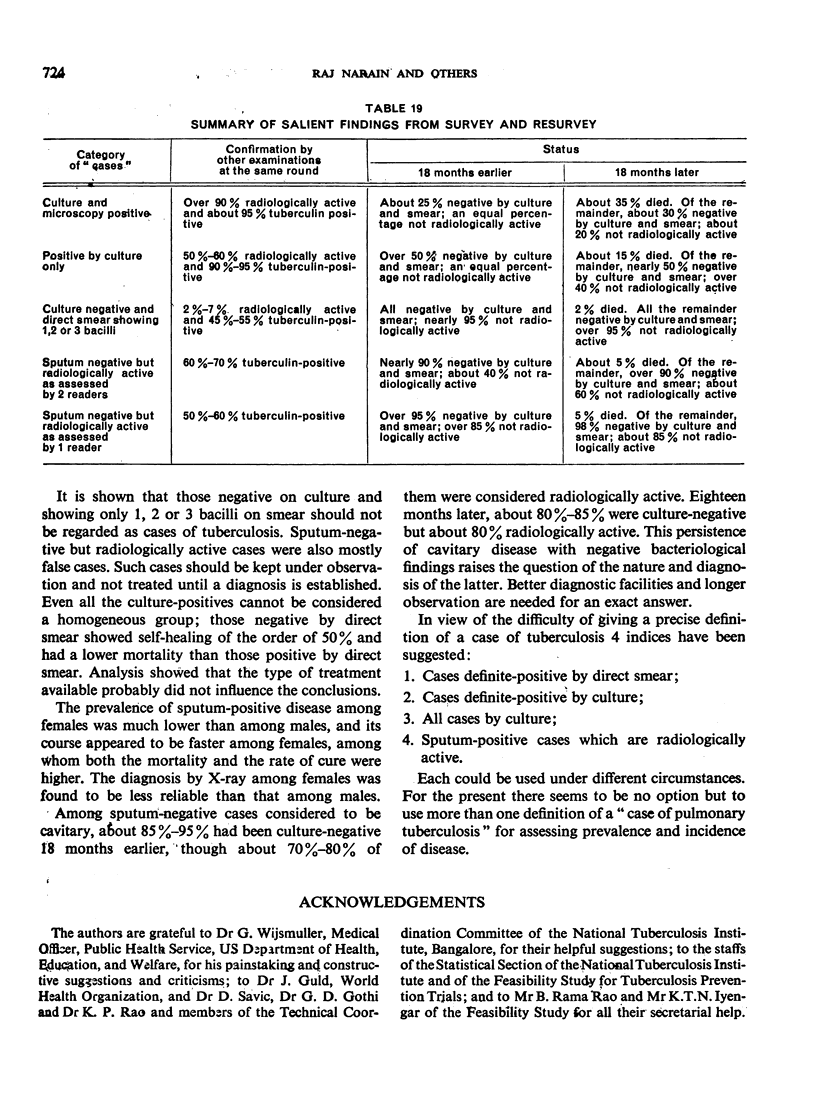
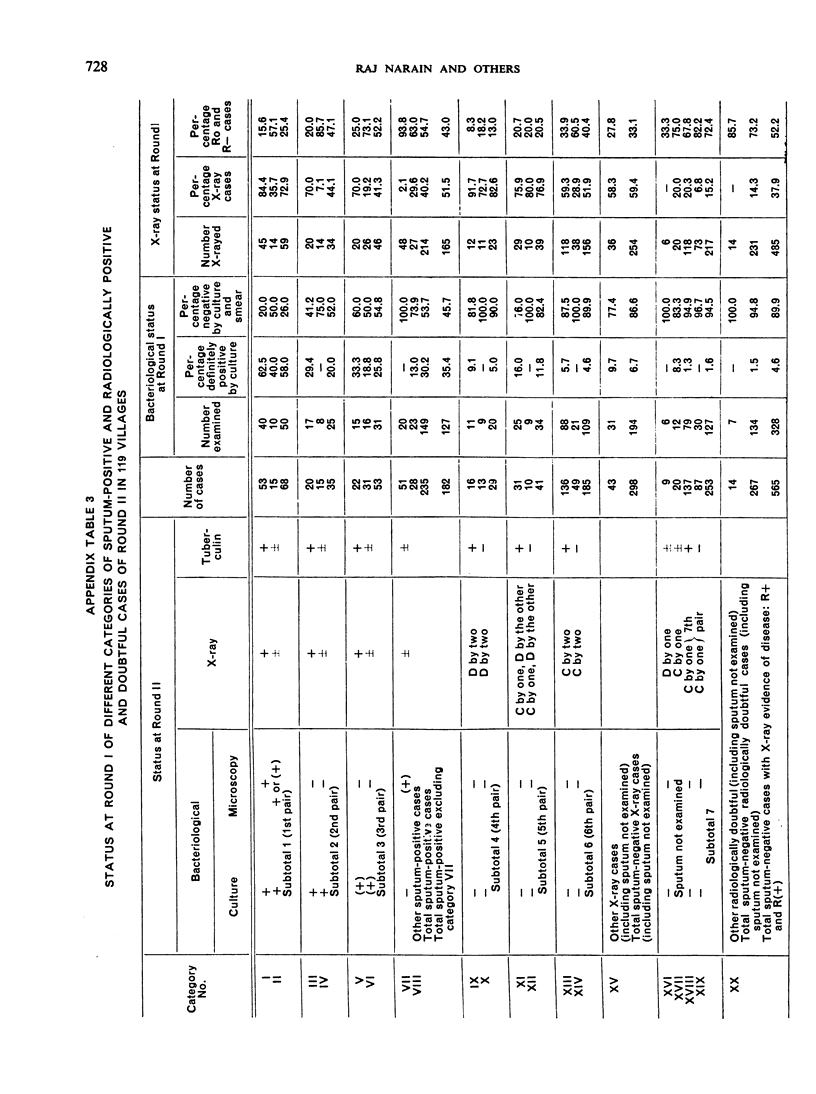
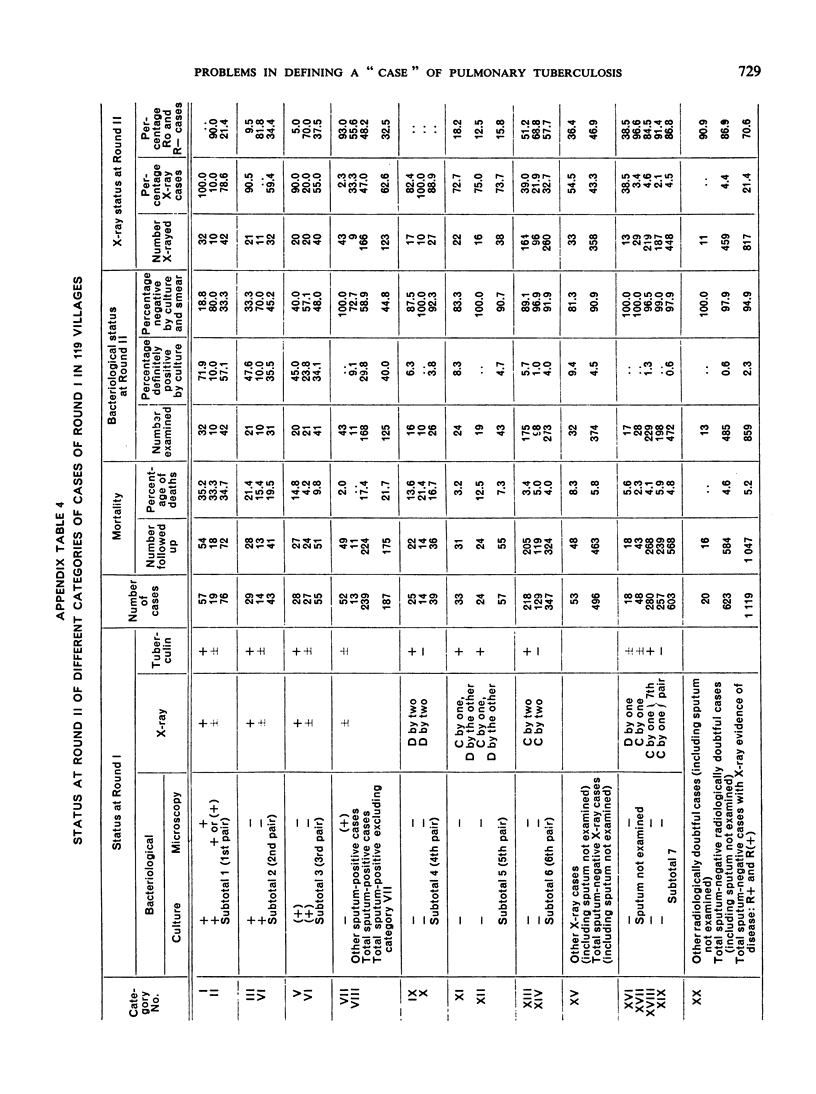
An analysis of data from two successive tuberculosis prevalence surveys (conducted at an interval of 18 months) in a random sample of villages in Bangalore District, South India, has shown that the term “a case of pulmonary tuberculosis” does not represent a single uniform entity, but rather embraces cases of several types, differing considerably in their mortality experience, tuberculin sensitivity, results of X-ray and sputum examinations, and in the reliability of their diagnosis.
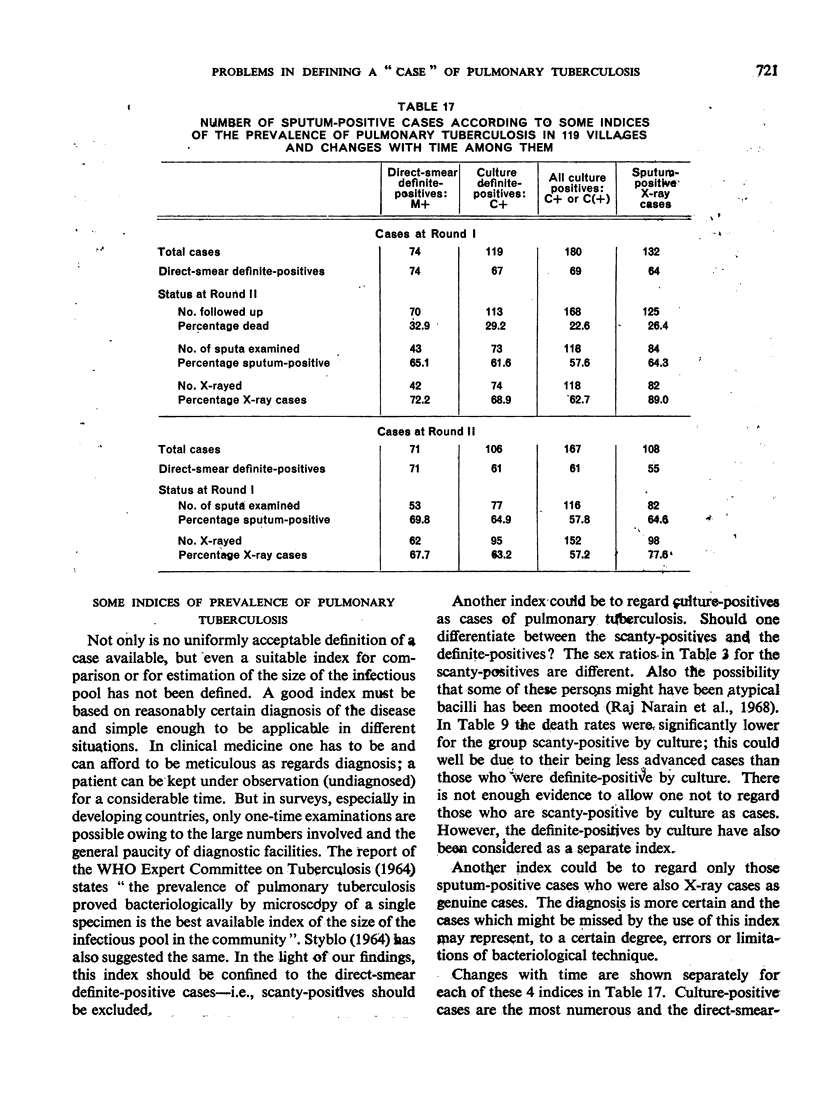
The status at the first survey of the cases found at the resurvey and that at resurvey of those found at the initial survey give an indication of changes with time. Such changes show considerable differences for the various types of cases and provide another dimension to study the differences among them. The authors consider that, in spite of the great need and importance of a single straightforward definition of a case, no such definition is suitable for all situations; there is no other option but to continue to use more than one definition.
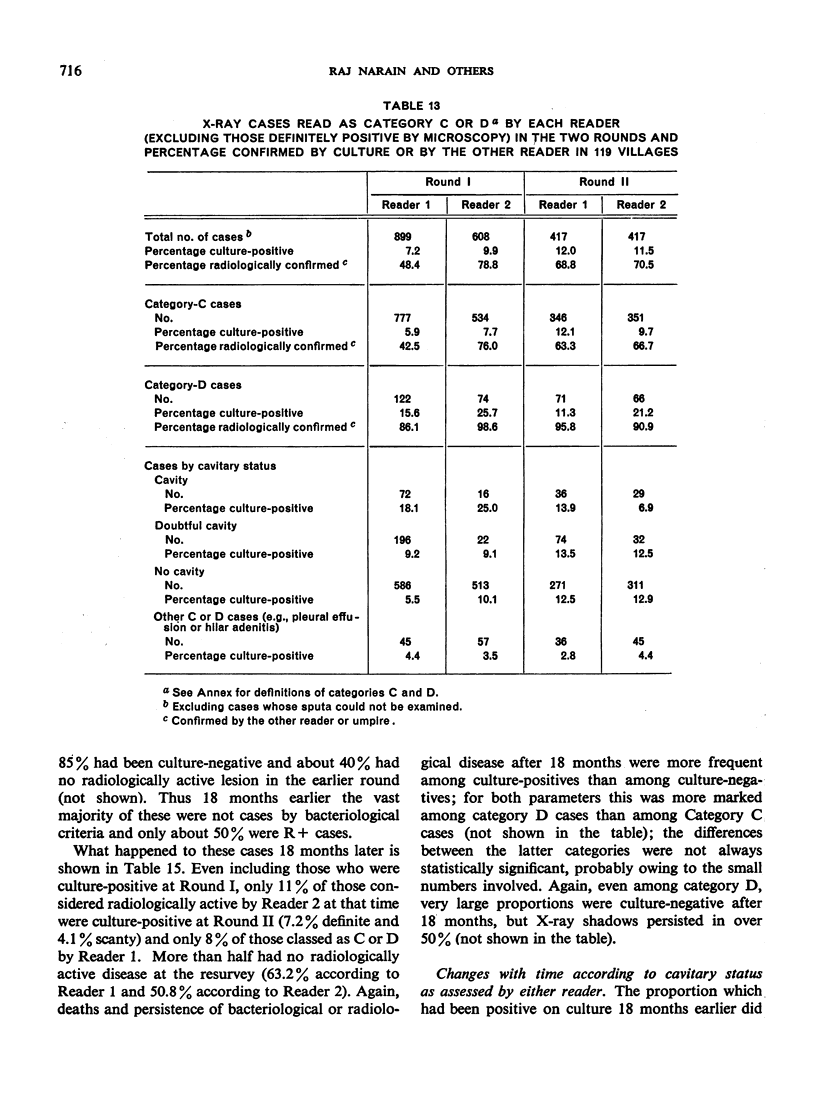
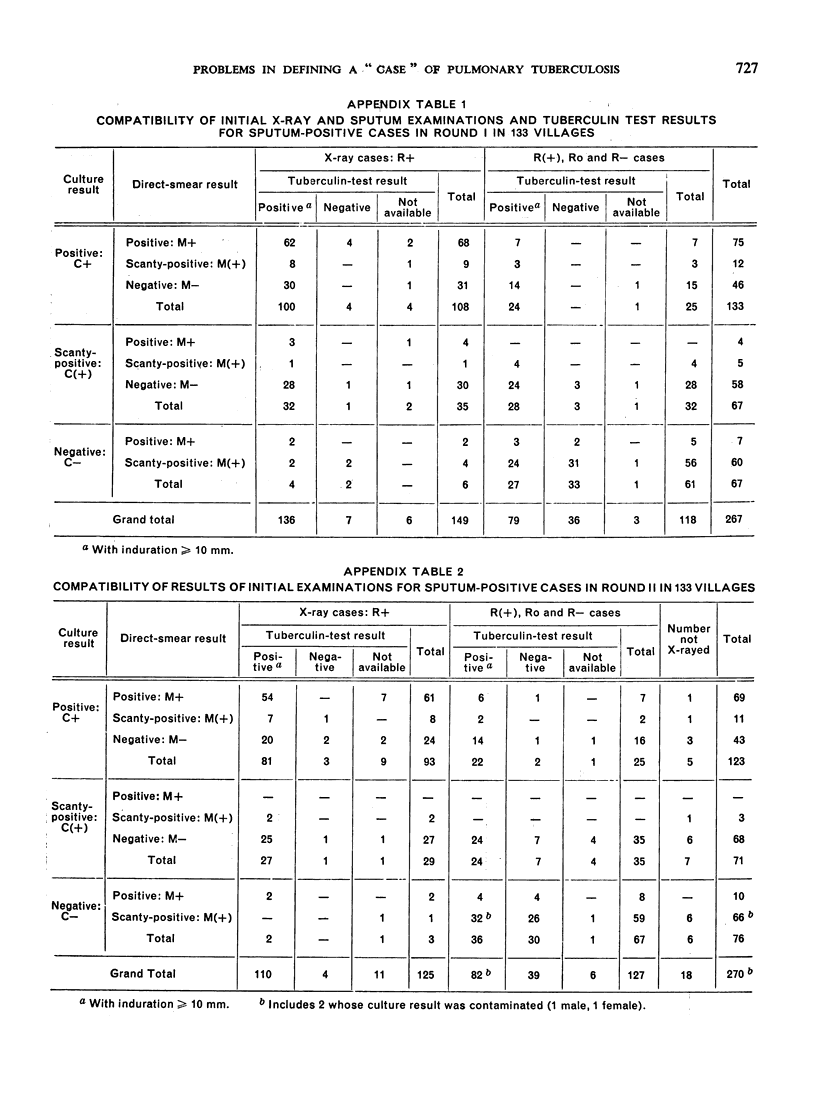
Although, theoretically, finding a single bacillus in the sputum should be adequate proof of pulmonary tuberculosis, it is shown that finding of a few bacilli, 3 or less, is probably far too often due to artefacts and should not be the basis for a diagnosis.
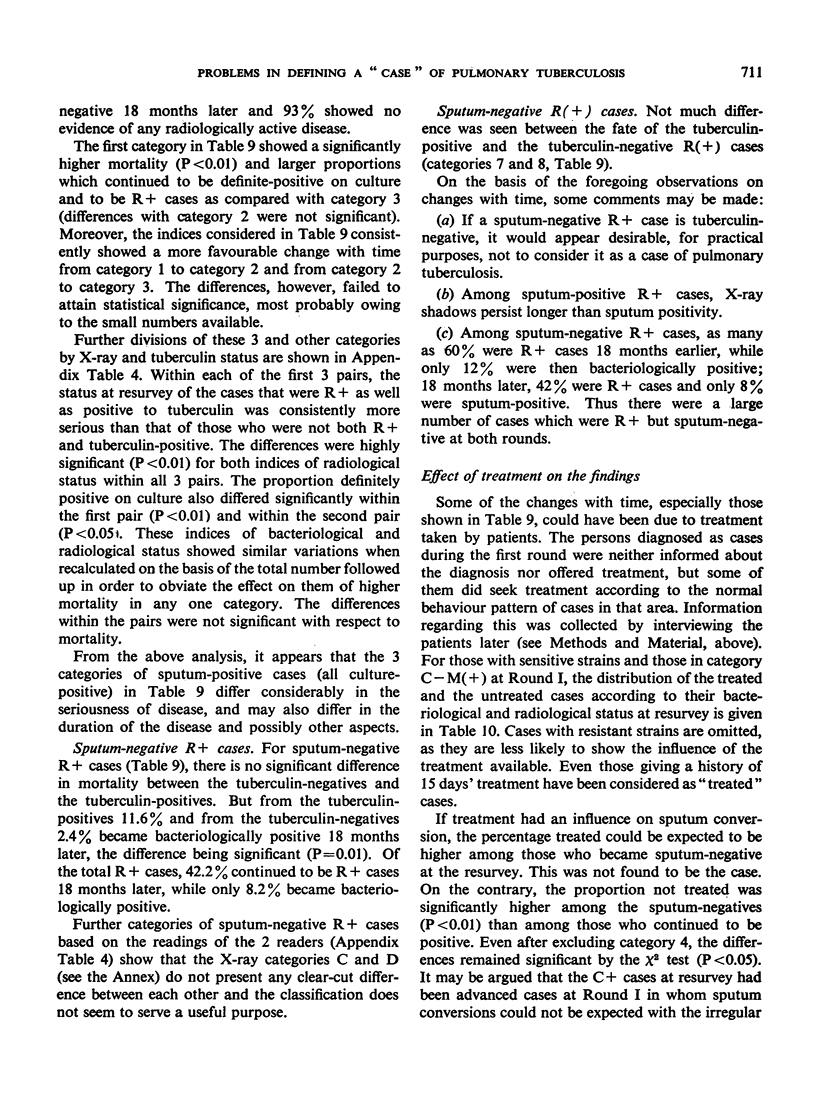
The findings also well bear out the notion that positive radiological findings, in the absence of bacteriological confirmation, indicate, not pulmonary tuberculosis, but only a high risk of the disease. Direct microscopy appears to be a consistent index of disease but, in community surveys, has the limitations of missing a substantial proportion of cases and of adding some false cases. The extent of these limitations, so far as symptomatic patients in a community tuberculosis control programme are concerned, remains to be investigated.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- NARAIN R., GESER A., JAMBUNATHAN M. V., SUBRAMANIAN M. SOME ASPECTS OF A TUBERCULOSIS PREVALENCE SURVEY IN A SOUTH INDIAN DISTRICT. Bull World Health Organ. 1963;29:641–664. [PMC free article] [PubMed] [Google Scholar]
- Narain R., Chandrasekhar P., Satyanarayanachar R. A., Lal P. Resistant and sensitive strains of Mycobacterium tuberculosis found in repeated surveys among a South Indian rural population. Bull World Health Organ. 1968;39(5):681–699. [PMC free article] [PubMed] [Google Scholar]
- Narain R., Nair S. S., Rao G. R., Chandrasekhar P. Distribution of tuberculous infection and disease among households in a rural community. Bull World Health Organ. 1966;34(4):639–654. [PMC free article] [PubMed] [Google Scholar]
- Narain R., Nair S. S., Rao G. R., Chandrasekhar P., Lal P. Enhancing of tuberculin allergy by previous tuberculin testing. Bull World Health Organ. 1966;34(4):623–638. [PMC free article] [PubMed] [Google Scholar]
- ROELSGAARD E., IVERSEN E., BLOCHER C. TUBERCULOSIS IN TROPICAL AFRICA. AN EPIDEMIOLOGICAL STUDY. Bull World Health Organ. 1964;30:459–518. [PMC free article] [PubMed] [Google Scholar]
- Styblo K. Possibilities of international comparison of newly detected cases of tuberculosis (incidence). Bull Int Union Tuberc. 1964 May;34(1):49–52. [PubMed] [Google Scholar]
- Wijsmuller G., Narain R., Mayurnath S., Palmer C. E. On the nature of tuberculin sensitivity in South India. Am Rev Respir Dis. 1968 Mar;97(3):429–443. doi: 10.1164/arrd.1968.97.3.429. [DOI] [PubMed] [Google Scholar]