

Abstract
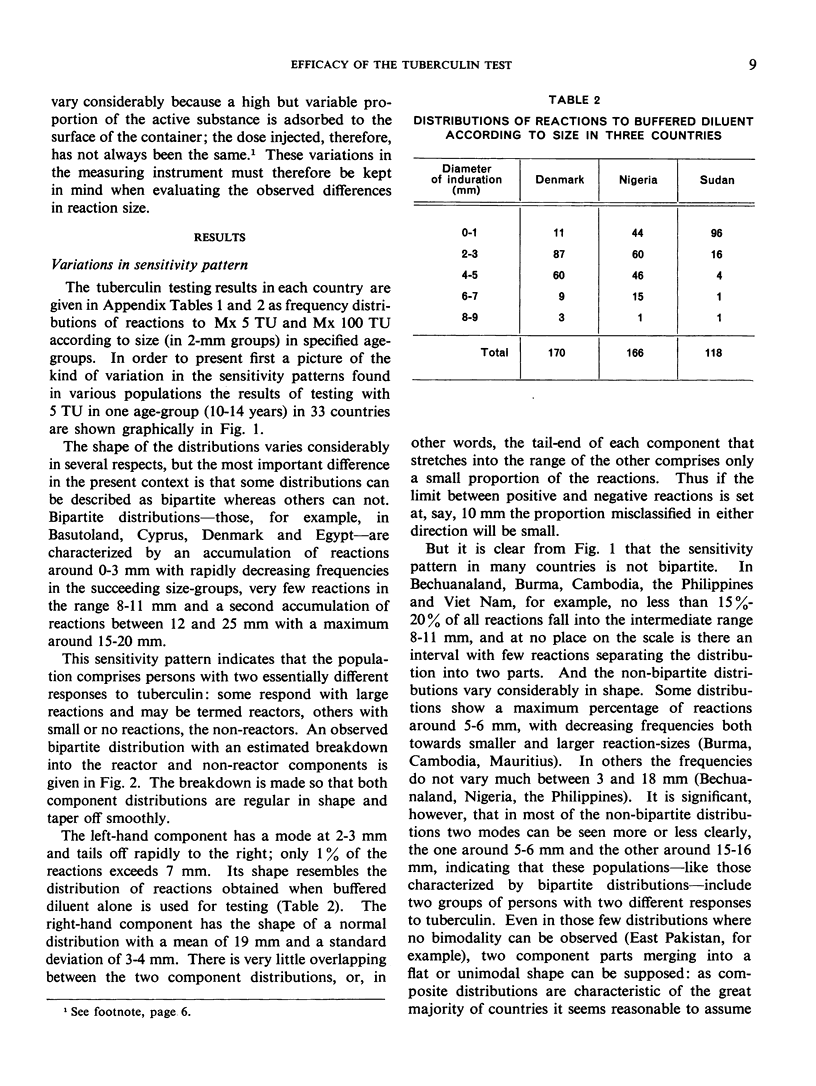
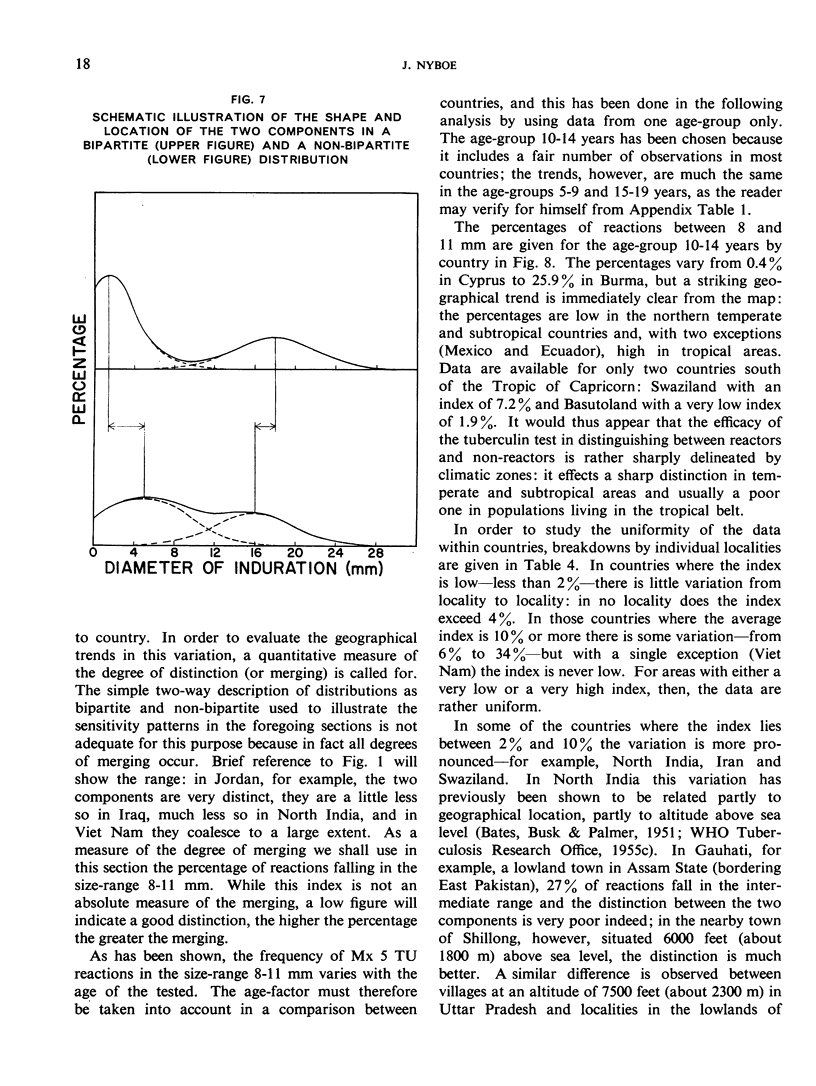
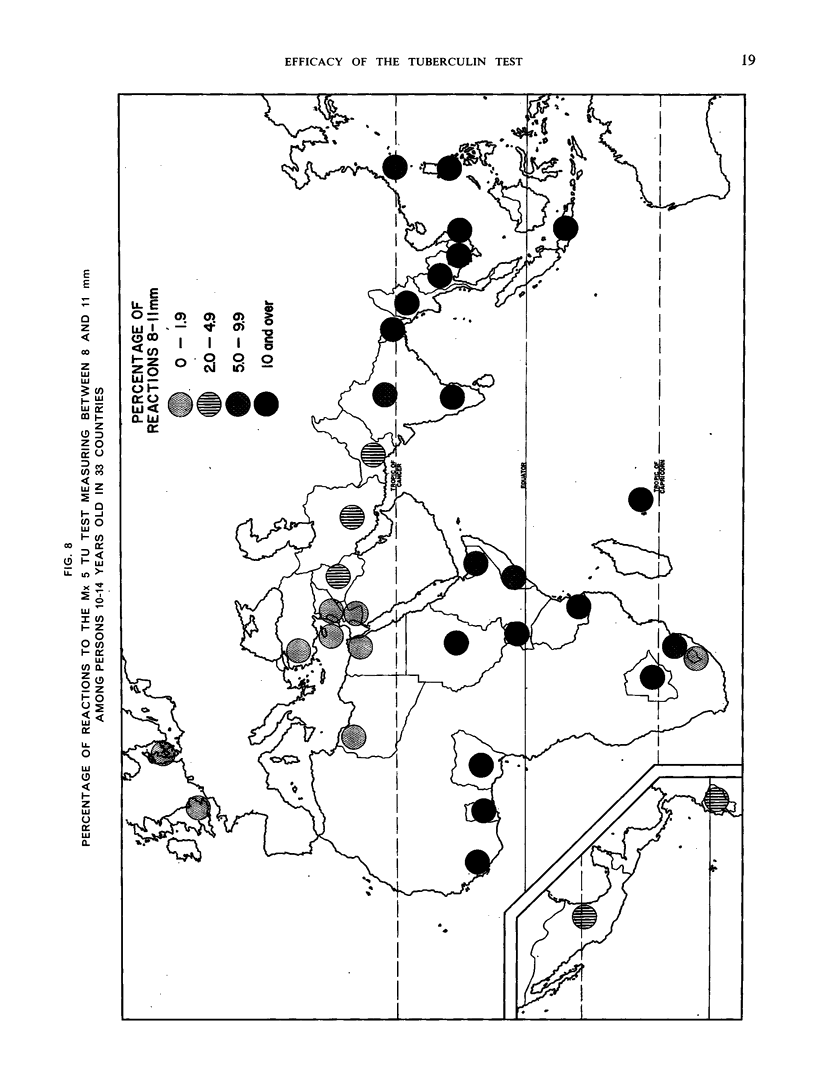
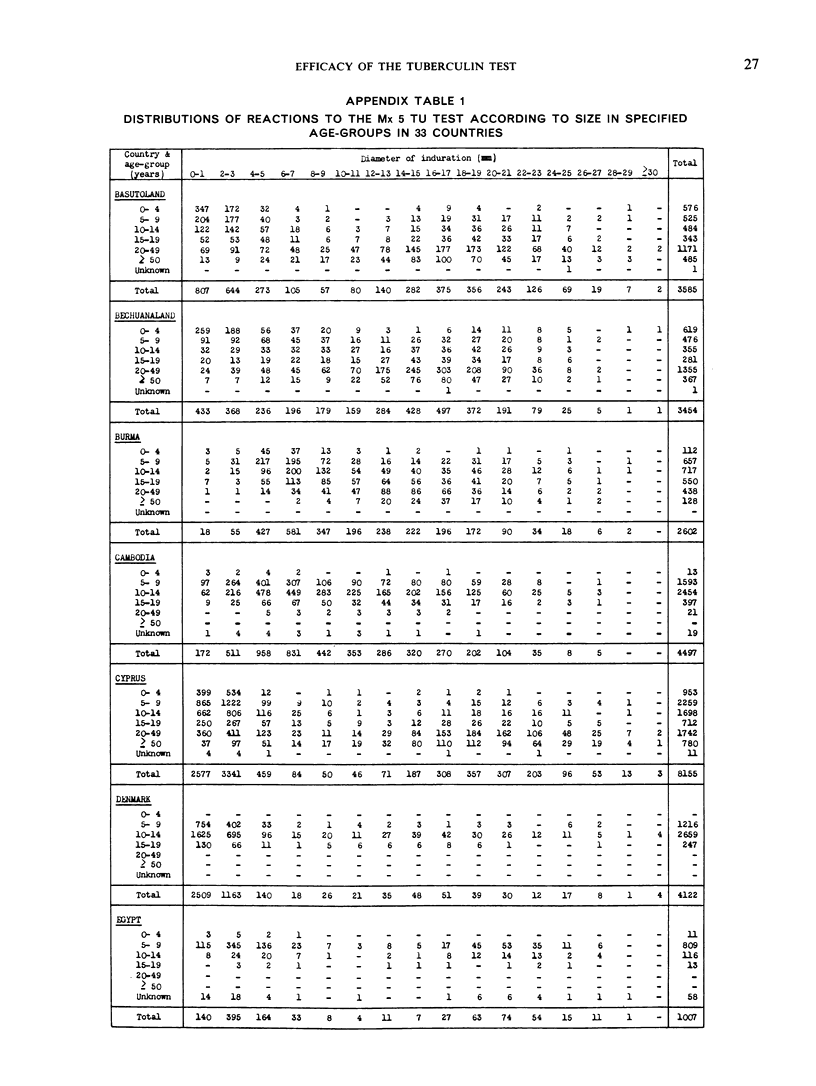
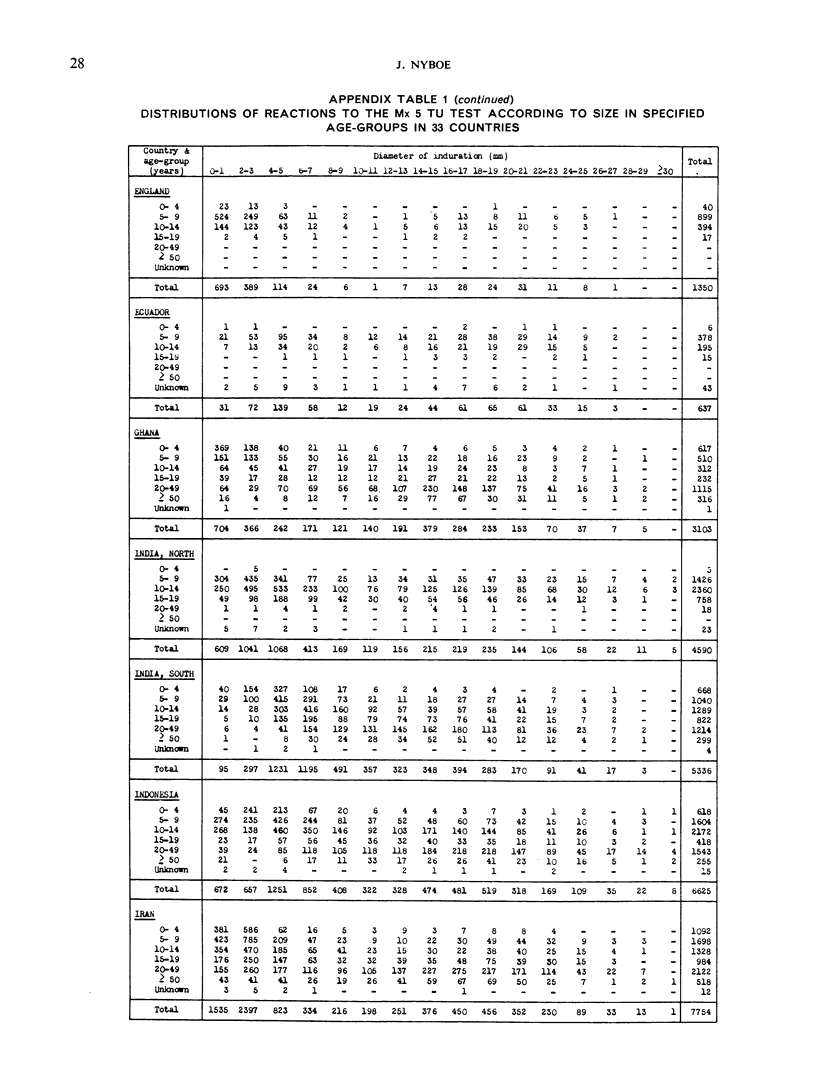
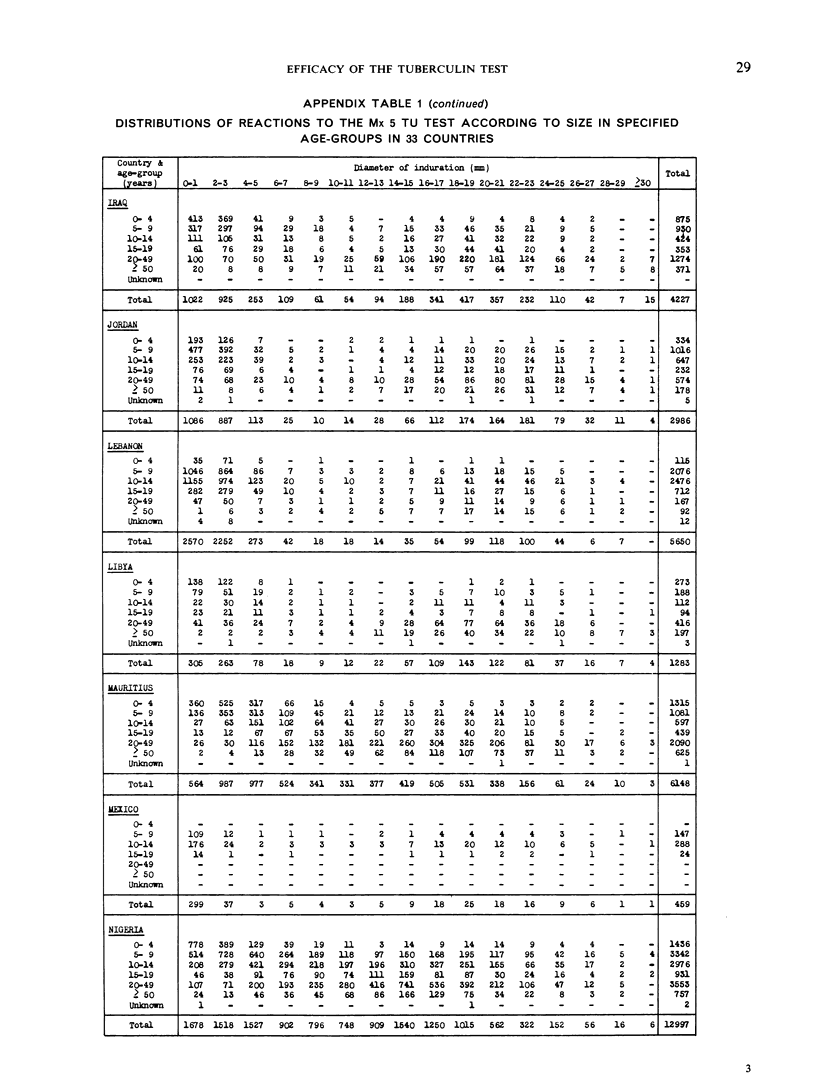
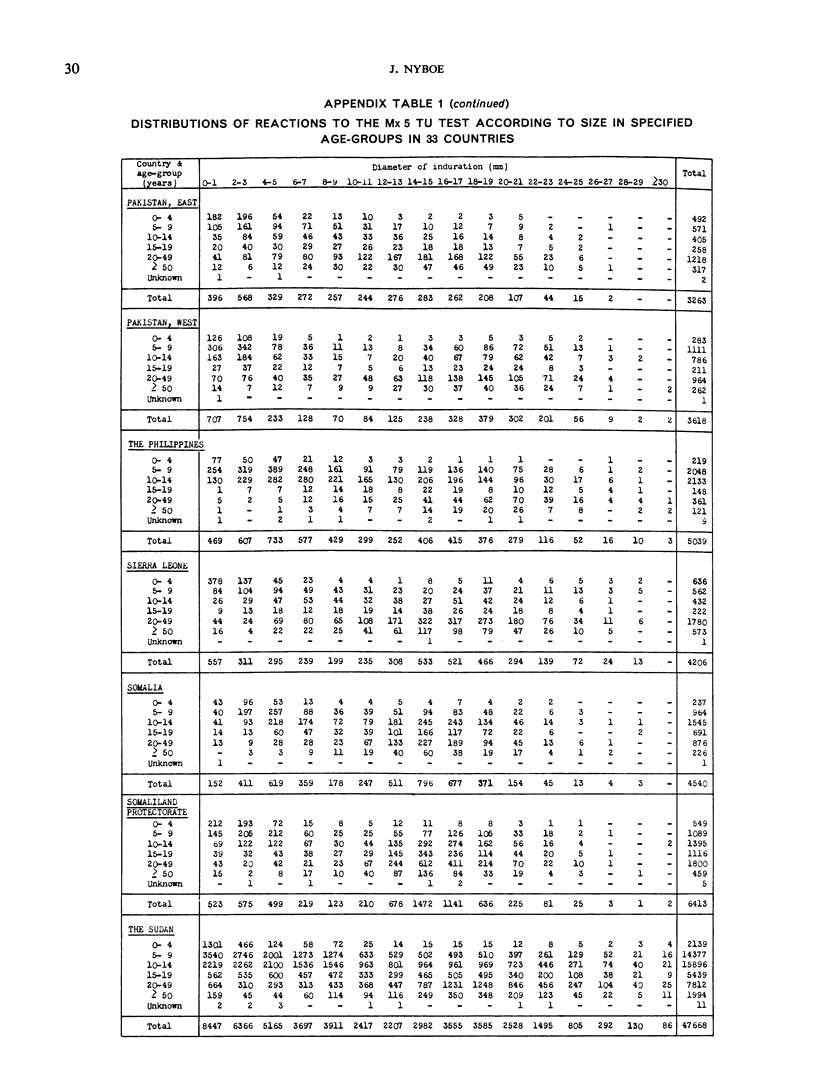
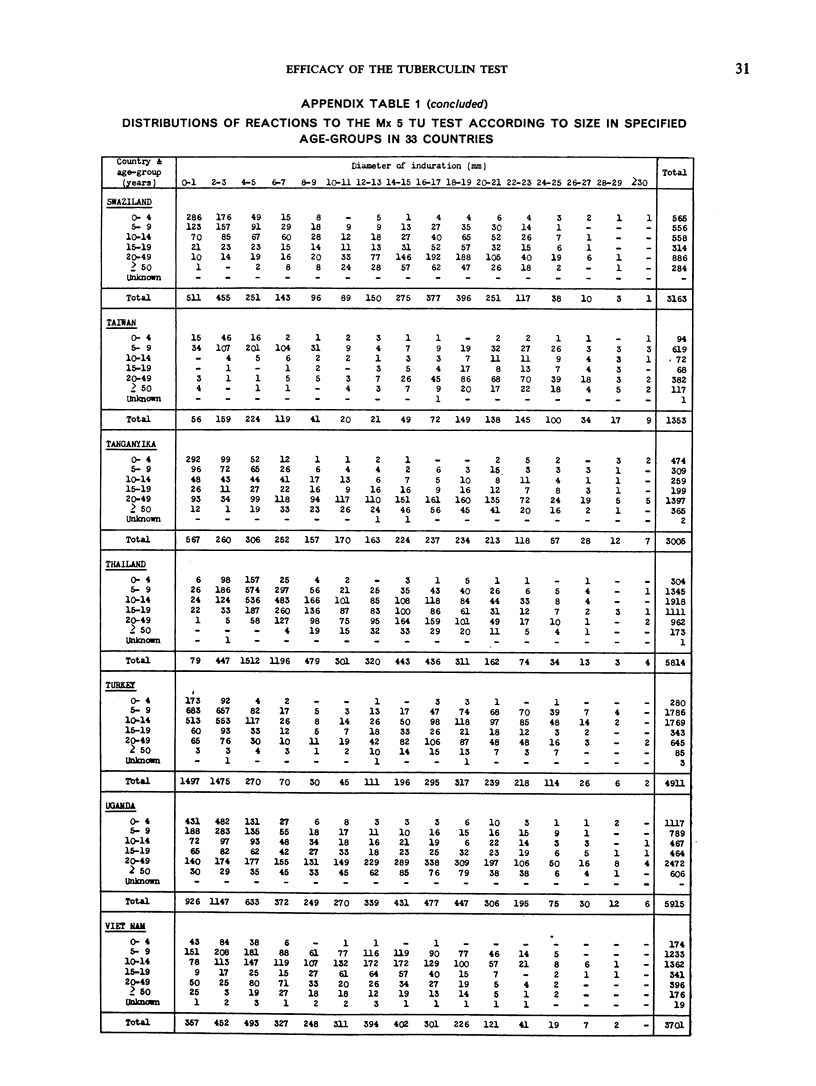
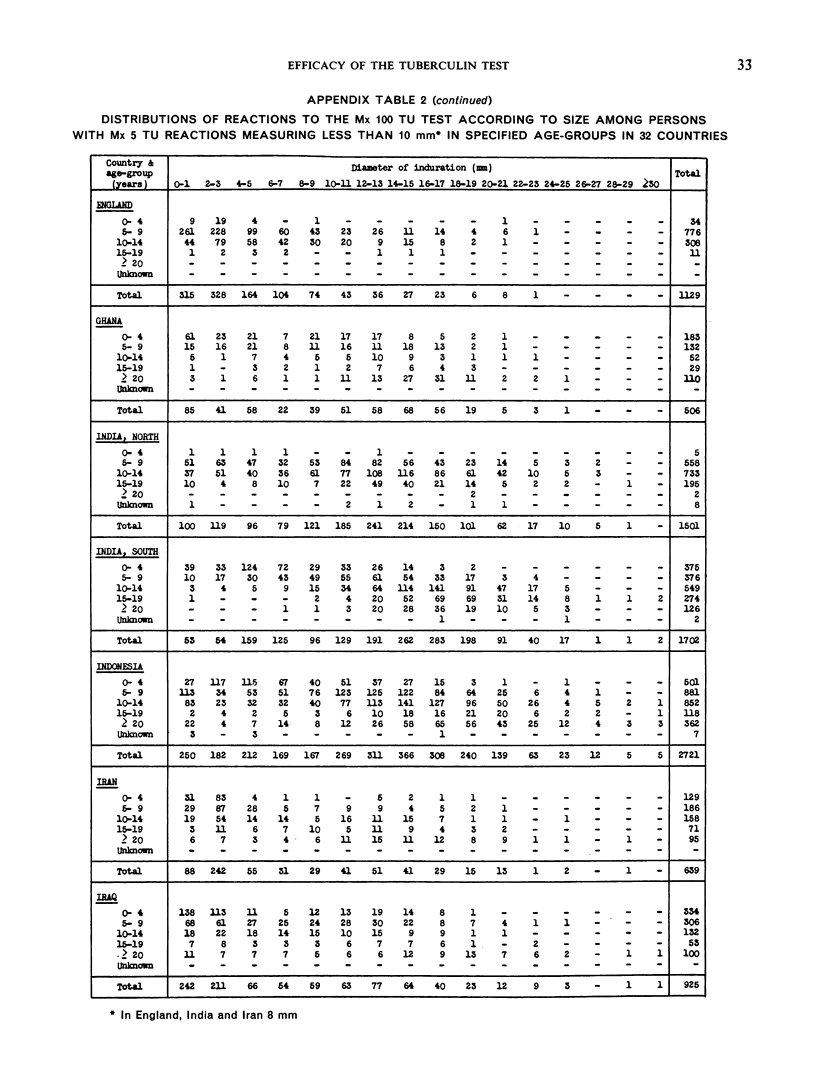
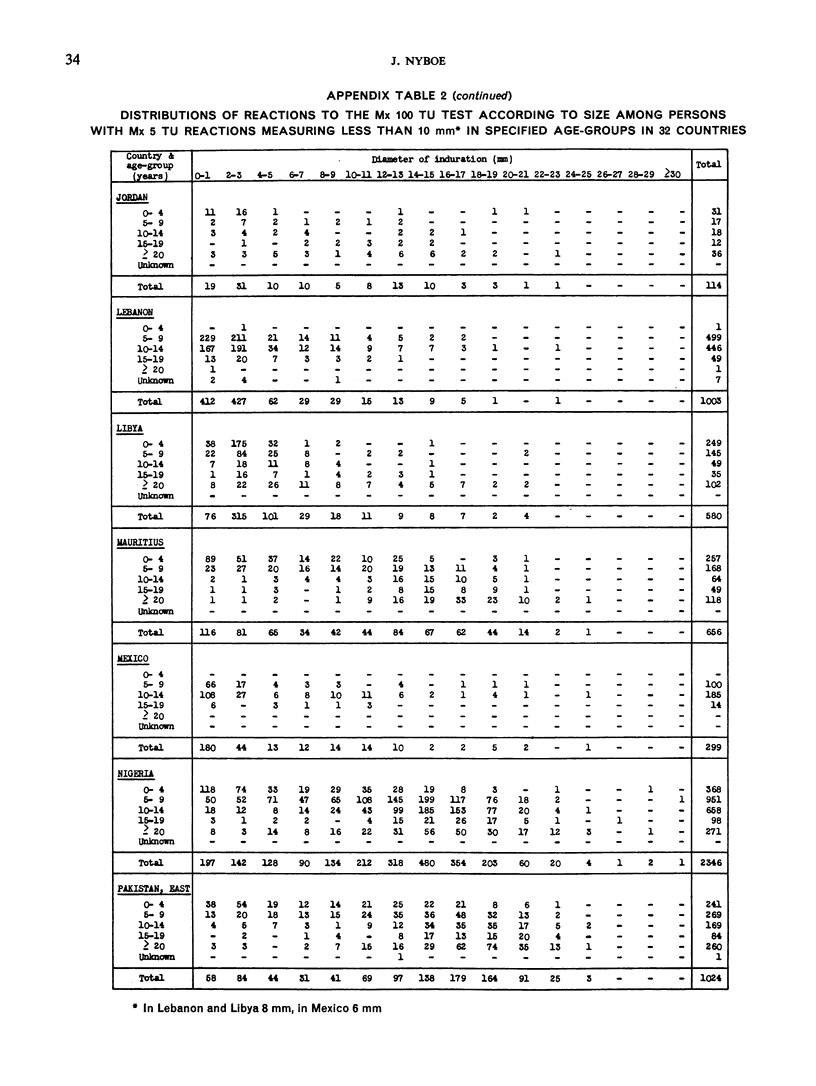
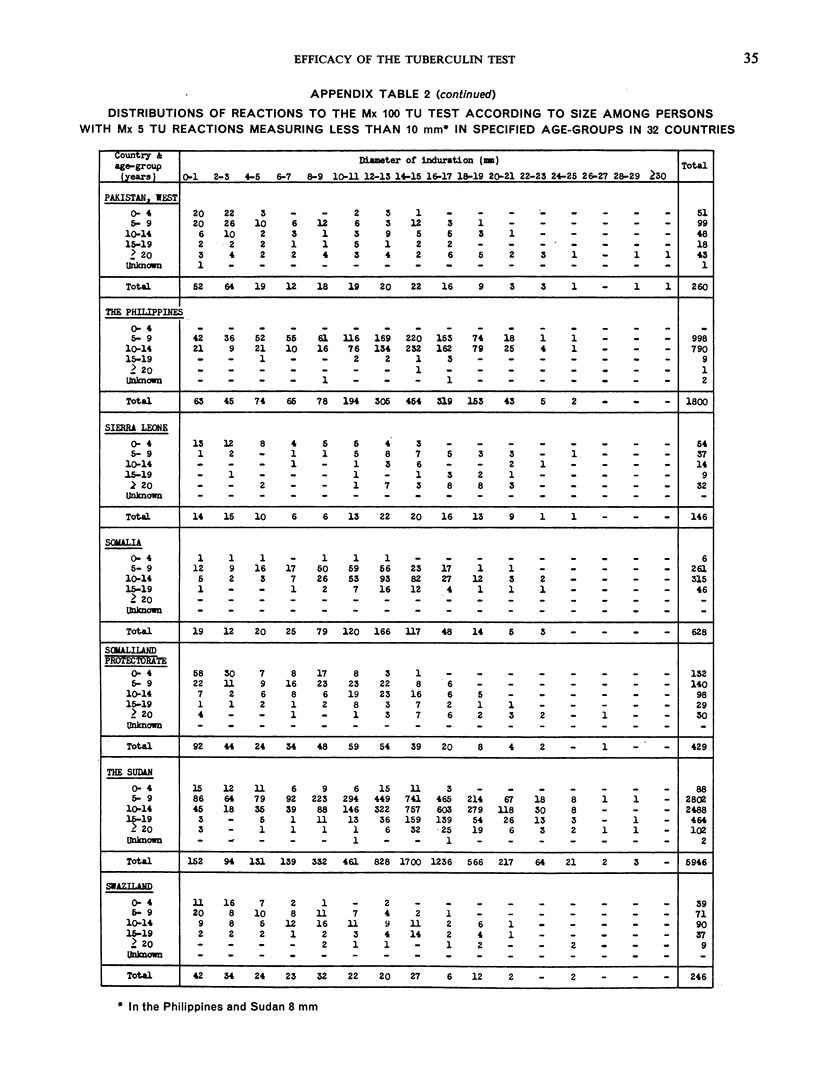
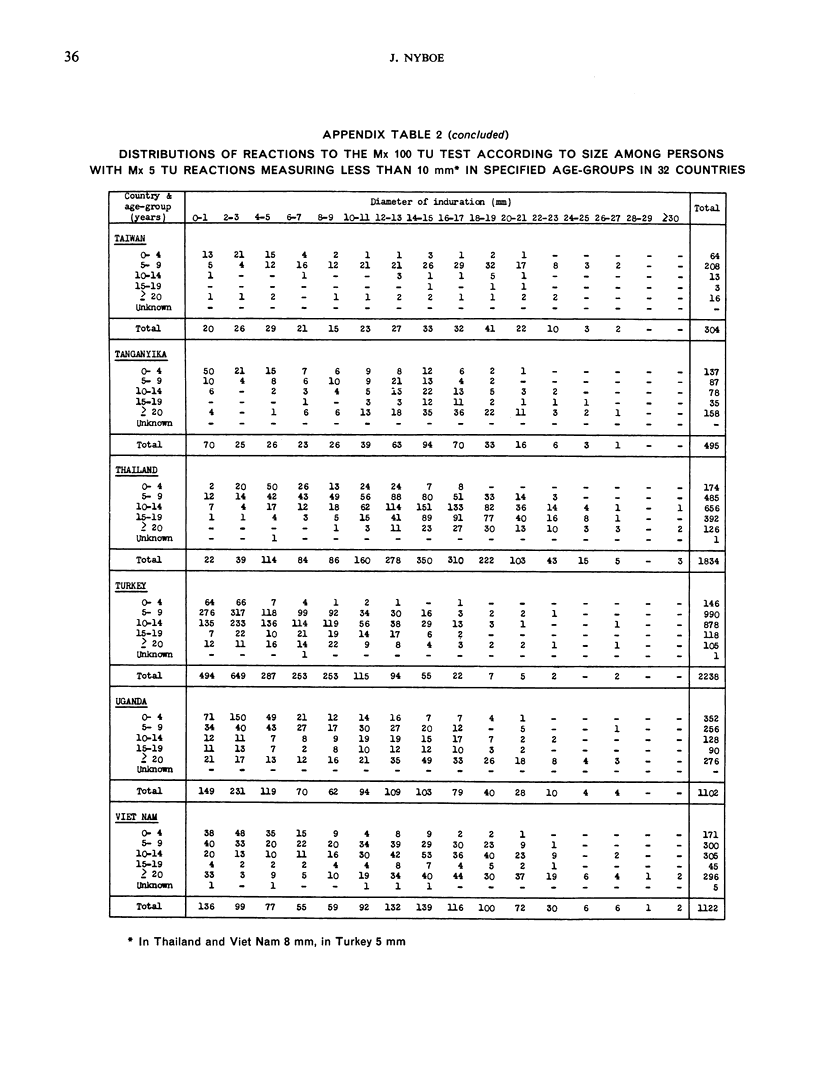
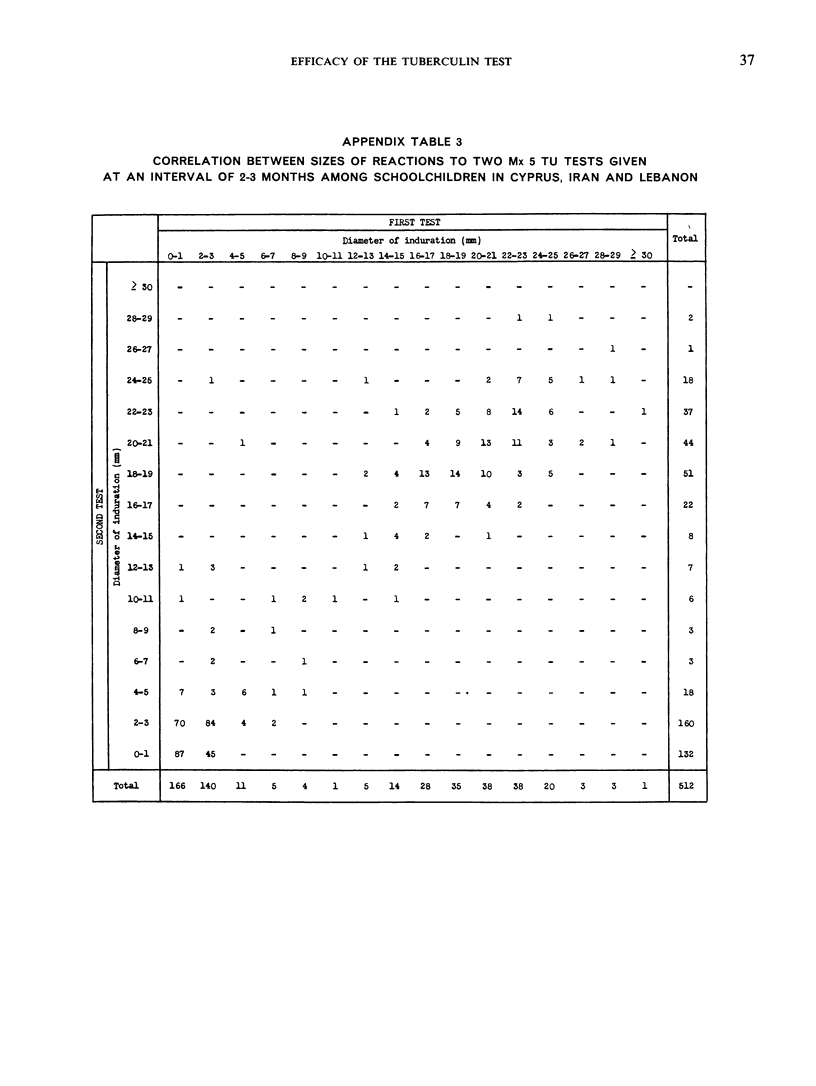
Is it always justified to take a tuberculin reaction over a certain size limit as indicative of infection with tubercle bacilli and reactions below the limit as indicative of absence of such infection? Information on this point is here derived from a quantitative analysis of test reactions found in general population groups. The data were collected by specially trained international teams operating simultaneously with or as a preliminary to large-scale tuberculosis control programmes. Because of the international character of the work it has been possible to compile a picture which shows the tuberculin sensitivity in a large part of the world, yet which is based on highly uniform techniques. It is hereby demonstrated that the pattern of tuberculin sensitivity varies widely between different populations, but follows a definite geographical trend. In temperate and subtropical countries almost all test reactions are either clearly ”positive” or clearly ”negative”, indicating that the test is highly efficient. In tropical regions, on the other hand, a large proportion of the reactions are intermediate in size, and distinction between two kinds of reaction is therefore difficult. The data strongly suggest that the cause of the intermediate reactions is that the population is being massively exposed to certain unidentified agents producing cross-reactions to tuberculin. In tropical regions a clear-cut distinction between tuberculosis infected and uninfected evidently cannot be made by means of the present tuberculin test.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BATES L. E., BUSK T., PALMER C. E. Research contributions of BCG vaccination programs. II. Tuberculin sensitivity at different altitudes of residence. Public Health Rep. 1951 Nov 2;66(44):1427–1441. [PubMed] [Google Scholar]
- EDWARDS L. B., PALMER C. E. Epidemiologic studies of tuberculin sensitivity. I. Preliminary results with purified protein derivatives prepared from atypical acid-fast organisms. Am J Hyg. 1958 Sep;68(2):213–231. [PubMed] [Google Scholar]
- GROTH-PETERSEN E., KNUDSEN J., WILBEK E. Konsekvensen af den aendrede epidemiologiske situation i tuberkulosearbejdet; tuberkulosemorbiditeten i den danske befolkning og i specifikke grupper af denne. Nord Med. 1957 Sep 19;58(38):1361–1369. [PubMed] [Google Scholar]
- PALMER C. E., SHAW L. W., COMSTOCK G. W. Community trials of BCG vaccination. Am Rev Tuberc. 1958 Jun;77(6):877–907. doi: 10.1164/artpd.1958.77.6.877. [DOI] [PubMed] [Google Scholar]
- PALMER C. E. Tuberculin sensitivity and contact with tuberculosis; further evidence of nonspecific sensitivity. Am Rev Tuberc. 1953 Nov;68(5):678–694. doi: 10.1164/art.1953.68.5.678. [DOI] [PubMed] [Google Scholar]
- WAALER H., GULD J., MAGNUS K., MAGNUSSON M. Adsorption of tuberculin to glass. Bull World Health Organ. 1958;19(5):783–798. [PMC free article] [PubMed] [Google Scholar]