

Abstract
Objective
To determine whether the relationship between bullying and psychosocial adjustment is consistent across countries by standard measures and methods.
Design
Cross-sectional self-report surveys were obtained from nationally representative samples of students in 25 countries. Involvement in bullying, as bully, victim, or both bully and victim, was assessed.
Setting
Surveys were conducted at public and private schools throughout the participating countries.
Participants
Participants included all consenting students in sampled classrooms, for a total of 113200 students at average ages of 11.5, 13.5, and 15.5 years.
Main Outcome Measures
Psychosocial adjustment dimensions assessed included health problems, emotional adjustment, school adjustment, relationships with classmates, alcohol use, and weapon carrying.
Results
Involvement in bullying varied dramatically across countries, ranging from 9% to 54% of youth. However, across all countries, involvement in bullying was associated with poorer psychosocial adjustment (P<.05). In all or nearly all countries, bullies, victims, and bully-victims reported greater health problems and poorer emotional and social adjustment. Victims and bully-victims consistently reported poorer relationships with classmates, whereas bullies and bully-victims reported greater alcohol use and weapon carrying.
Conclusions
The association of bullying with poorer psychosocial adjustment is remarkably similar across countries. Bullying is a critical issue for the health of youth internationally.
The problem of bullying among youth has become an international concern.1 Recent studies on school-aged children in Australia,2 England,3 Finland,4 Germany,3 Scotland,5 and the United States6 suggest that bullying is associated with adverse outcomes for both the victim and the bully, including poorer social, emotional, and physical health. Findings from research in Australia, Finland, and Norway indicate that these psychosocial challenges may persist into later adolescence7,8 and adulthood.9,10
According to Olweus,11 bullying is characterized by (1) aggressive behavior or intentional harm-doing that is (2) carried out repeatedly over time in (3) an interpersonal relationship characterized by an imbalance of power. This aggressive behavior may be verbal, physical, or relational. Whereas verbal aggression is common among both girls and boys, physical aggression and taking of personal belongings tend to occur more frequently among boys, and rejection or isolation is more common among girls.12,13
Research published during the past 15 years has shown that bullying is prevalent across countries.3,4–23 However, studies vary as to the definition of bullying used, the methods used to measure bullying, and the cutoff point used for reporting of prevalence. Consequently, comparing prevalence and outcomes of bullying cross-nationally has been difficult.3
The Health Behaviour in School-aged Children (HBSC) Study provides a unique opportunity to compare data on bullying across countries. This international collaborative effort was coordinated by a multicountry committee with measures, sampling, and administration procedures designed to be consistent across participating countries, thus allowing for international comparisons. In addition, the sampling design provides nationally representative estimates, as opposed to reflecting smaller regions or communities of unknown generalizability. In the present study, we used data collected from the 1997–1998 HBSC Study in 25 countries. The purpose of this study is to compare the relationship between bullying and psychosocial adjustment across countries by standard measures and methods. We examined the relationship of being bullied and bullying others with physical health, emotional adjustment, school adjustment, peer relationships, alcohol use, and weapon carrying.
METHODS
STUDY POPULATION AND PROCEDURES
The HBSC Study is an international collaborative study in which cross-sectional survey data on health-related behaviors are collected from students at average ages of 11.5, 13.5, and 15.5 years. School-based anonymous surveys were conducted during the 1997–1998 academic year according to a common research protocol.24 Excepting Greenland, which surveyed the entire student population, a cluster sample design of classrooms within schools was used in each country. Statistical precision requirements from the HBSC sampling criteria are used to assess the reliability of variable estimates. Criteria specify that samples submitted for international comparisons are sufficient to provide confidence internals of ±3% for representative estimates with sample design effects no more than 1.4 times greater than would be obtained from a simple random sample. Student response rates ranged from 74% to 99%.
Participating research teams may collect information from administrative regions rather than whole countries as long as the population is more than 1 million, as was done in Flemish Belgium and the North Rhine–Westphalia region of Germany. Human subject protection guidelines within each country or sponsoring institution were followed as required. In the United States, the protocol was approved by the National Institute of Child Health and Human Development Institutional Review Board with active consent from parents and students. A total of 28 countries or regions met criteria for inclusion in the 1997–1998 HBSC dataset. However, 3 countries lacked sufficient information on sampling units to analytically account for the cluster sample design and were not included in this analysis. For the 25 countries included in this study, sample sizes ranged from 1648 to 6567, with a mean of 4528.
MEASURES
Measures for this study were obtained from a self-report questionnaire containing 84 core questions and additional country-specific items (http://www.hbsc.org). Participants were provided with a standard definition of bullying and asked to report how frequently they had been bullied at school during the current school term and how frequently they had bullied others at school during the current term. With the use of a cutoff of greater than twice for involvement in bullying, students were classified into mutually exclusive categories as noninvolved, victims, bullies, or both bully and victim.25 Psychosocial adjustment was assessed by 5 composite measures: health problems (α=0.76), emotional adjustment (α=0.72), school adjustment (α=0.83), relationship with classmates (α=0.70), and alcohol use (α=0.81). Weapon carrying was an optional item assessed in 6 countries; responses were dichotomized to indicate ever or never weapon carrying during the past 30 days.
Composite measures of psychosocial status were factor-analytically derived, with a random half of the sample used for the initial factor analysis and items deleted that did not load above 0.4. Factor structures were confirmed on the second half of the sample and then checked for each individual country. Items that did not load consistently across countries were deleted. If a student completed at least three fifths of the items composing a scale, the value for any missing items was imputed on the basis of the mean of completed items composing that measure.26 To allow for meaningful interpretation of scores, scale scores were transformed to z scores by country, standardized to a mean of 0 and an SD of 1. Means could then be interpreted as percentiles, with values of 0 at the 50th percentile, scores near 1 at about the 85th percentile, and scores near −1 at about the 15th percentile.
ANALYSES
Data analyses were conducted with SUDAAN software (Research Triangle Institute, Research Triangle Park, NC) to adjust variance estimates to account for the sample design and clustering. Linear regression analyses were used to assess differences among bully and victim groups in health problems, emotional adjustment, school adjustment, relationship with classmates, and alcohol use for each country, and then for the full sample. Because bullying has been shown to be related to age and sex, both age and sex were entered as covariates in the models. Logistic regression analyses, with age and sex as covariates, were used to examine the relationship between involvement in bullying and weapon carrying for the 6 countries that included an assessment of weapon carrying as part of the survey.
RESULTS
Involvement in bullying at school—as bully, victim, or both—ranged from 9% in Sweden to 54% in Lithuania (Figure 1). Children classified as being victims ranged from 5% in Sweden to 20% in Lithuania, with an average across countries of 11%. With respect to bullying others, Sweden and Wales had the lowest rates at 3% while Denmark had the highest prevalence at 20%, with an overall average of 10%. Lithuania reported the highest prevalence of bully-victims at 20%, and Sweden had the lowest at 1%, with the countries averaging 6%.
Figure 1.

Involvement in bullying more than twice during the current school term in 25 countries.
Across all countries, involvement in bullying was associated with poorer psychosocial adjustment for bullies, victims, and bully-victims (Figure 2 and Figure 3). Youth involved in bullying—as bully, victim, or both—consistently reported significantly higher levels of health problems, poorer emotional adjustment, and poorer school adjustment than noninvolved youth. Victims and bully-victims also consistently reported significantly poorer relationships with classmates than noninvolved youth; bullies reported significantly poorer relationships in a little more than half of the countries. Bullies and bully-victims (but not victims) consistently reported significantly more frequent alcohol use.
Figure 2.

Standardized mean scores on psychosocial adjustment (health problems [A], emotional adjustment [B], and alcohol use [C]) by involvement in bullying in 25 countries (adjusted for age and sex).
Figure 3.

Standardized mean scores on psychosocial adjustment (school adjustment [A] and relationship with classmates [B]) by involvement in bullying in 25 countries (adjusted for age and sex).
Several differences between bullies and victims were noted (Table 1). Victims reported poorer emotional adjustment and poorer relationships with classmates than bullies. Specifically, in all countries, victims showed poorer emotional adjustment than bullies, and in all but 2 countries, they showed poorer relationships with classmates. In contrast, bullies reported poorer school adjustment and more frequent alcohol use than victims. In 12 of the 25 countries, bullies demonstrated poorer school adjustment than victims; although in 2 countries, victims reported poorer adjustment (with no significant differences in the other 11 countries). In all countries, bullies reported greater alcohol use than victims. Fewer differences were observed for health problems. Victims reported more health problems than bullies in only 6 of the 25 countries while bullies had greater health problems than victims in 2 countries (with no significant differences in the other 17 countries).
Table 1.
Numbers of Countries With Significant Differences Between Bullying Involvement Groups
| No. of Countries (N = 25)
|
|||||
|---|---|---|---|---|---|
| Health Problems | Emotional Adjustment | School Adjustment | Relationship With Classmates | Alcohol Use | |
| Comparison with noninvolved youth | |||||
| Victims report poorer adjustment than noninvolved | 25 | 25 | 25 | 25 | 0 |
| Bullies report poorer adjustment than noninvolved | 25 | 21 | 24 | 15 | 25 |
| Bully-victims report poorer adjustment than noninvolved | 25 | 25 | 24 | 25 | 23 |
| Comparisons of victims and bullies | |||||
| Victims report poorer adjustment than bullies | 6 | 25 | 2 | 23 | 0 |
| Bullies report poorer adjustment than victims | 2 | 0 | 12 | 0 | 25 |
| No significant difference between bullies and victims | 17 | 0 | 11 | 2 | 0 |
| Comparison of bully-victims with victims and bullies | |||||
| Bully-victims demonstrate poorer adjustment than victims | 2 | 0 | 11 | 0 | 22 |
| Bully-victims demonstrate poorer adjustment than bullies | 7 | 25 | 1 | 20 | 0 |
| Bully-victims demonstrate poorer adjustment than both victims and bullies | 8 | 0 | 5 | 1 | 1 |
| Bully-victims not significantly worse than either bullies or victims | 8 | 0 | 8 | 4 | 2 |
The most striking pattern of psychosocial adjustment was demonstrated by the bully-victims, who reported levels of emotional adjustment, relationships with classmates, and health problems similar to those of victims, with levels of school adjustment and alcohol use similar to those of bullies. Moreover, in some cases, their scores were significantly worse than those of either bullies or victims. In 8 countries bully-victims reported more health problems than the other 2 groups, and in 5 countries they reported more school adjustment problems.
Because findings were generally consistent across countries, analyses were conducted with combined data from all countries. As shown in Figure 4, victims, bullies, and bully-victims demonstrated significantly greater health problems and poorer school adjustment than the study population mean. In addition, victims and bully-victims demonstrated poorer emotional adjustment and relationship with classmates, whereas bullies and bully-victims demonstrated greater alcohol use.
Figure 4.
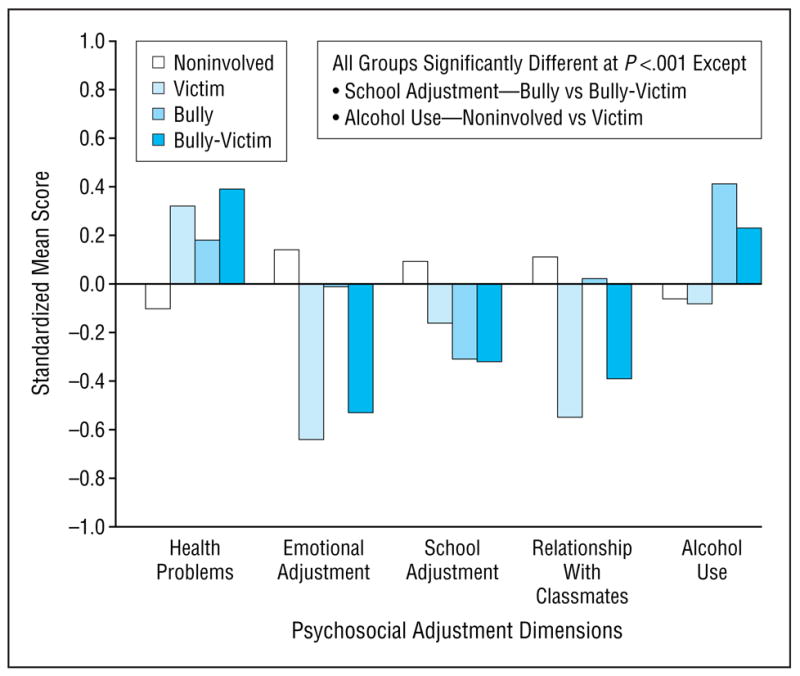
Standardized mean scores on psychosocial adjustment dimensions by involvement in bullying with the use of combined data from 25 countries (adjusted for age and sex).
Six countries assessed weapon carrying in the past 30 days (Table 2). In 3 of the 6 countries (Flemish Belgium, Hungary, and Portugal), victims of bullying did not show significantly greater odds of weapon carrying than noninvolved youth; however, in Israel, Republic of Ireland, and the United States, victims showed 1.98 to 2.27 greater odds of weapon carrying than noninvolved youth. With only 1 marginal exception (Hungary), both bullies and bully-victims across countries showed significantly greater odds of weapon carrying than noninvolved youth, with odds ratios ranging from 2.77 to 4.34 for bullies and 1.96 to 8.50 for bully-victims. In 5 of the 6 countries, bullies and bully-victims were not significantly different; however, in the United States, bully-victims demonstrated significantly greater odds of weapon carrying than bullies.
Table 2.
Odds Ratios for Weapon Carrying Among Bully-Victim Groups in 6 Countries (Adjusted for Age and Sex)
| Odds of Weapon Carrying (95% Confidence Interval)
|
||||
|---|---|---|---|---|
| Noninvolved* | Victim | Bully | Bully-Victim | |
| Belgium, Flemish | 1.00 | 1.25 (1.00–1.56) | 2.77 (2.30–3.35) | 1.96 (1.48–2.59) |
| Hungary | 1.00 | 1.12 (0.74–1.70) | 2.88 (1.99–4.16) | 1.64 (1.00–2.69) |
| Israel | 1.00 | 1.98 (1.55–2.52) | 4.43 (3.27–6.00) | 3.44 (2.55–4.64) |
| Portugal | 1.00 | 1.40 (0.93–2.12) | 3.20 (2.00–5.12) | 2.88 (1.87–4.43) |
| Republic of Ireland | 1.00 | 1.99 (1.40–2.83) | 3.50 (2.54–4.81) | 4.12 (2.16–7.86) |
| United States | 1.00 | 2.27 (1.74–2.97) | 4.34 (3.58–5.26) | 8.50 (6.42–11.26) |
Referent group
COMMENT
This is the first study, to our knowledge, assessing the relationship between bullying and psychosocial adjustment across countries in nationally representative samples by standard measures and methods. Significant differences in the overall prevalence of bullying among countries, as well as the proportion of victims, bullies, and bully-victims, were observed; yet the consistency of findings regarding the relationship between bullying and psychosocial adjustment is striking. This suggests that being the victim or perpetrator of abusive social relationships may have an adverse effect on youths’ physical, emotional, and social development. Bully-victims exhibited the poorest psychosocial adjustment overall, in that they reported functioning equal to or worse than the poorest functioning group (bully vs victim) across all dimensions. Their poor functioning across all factors indicates an especially high-risk group for emotional and social difficulties.27,28
The universality of problems associated with bullying and victimization may provide some hints for understanding potential underlying mechanisms. Victims and bully-victims clearly demonstrated poor emotional adjustment and greater levels of health problems. Being bullied may lead to poor emotional adjustment by negatively shaping youths’ self-concept; this is supported by studies across several countries.29–31 Only a few studies have examined the relationship between bullying and health problems32–34; these associations may reflect the stress of repeated bullying. In addition to reporting poorer emotional and physical health, victims and bully-victims demonstrated problematic peer relationships. Youth who are victimized are likely marginalized from the mainstream peer group, lacking access to prosocial peers who provide role models of appropriate social skills, and also protection against bullying. Bullies, on the other hand, may have peer groups that endorse and support their aggressive behavior.11 This may account for some of the discrepancies across countries. The sociocultural environment may influence the extent to which bullies are successful in their domination and do not experience marginalization for it. The problems in school adjustment observed among bullies and victims may occur for multiple reasons. For both bullies and victims, problematic peer relationships may interfere with learning. Bullies may experience further school-related difficulty because of greater overall involvement in externalizing behavior, supported by the finding that they also reported the highest level of alcohol use. Whatever the mechanism, involvement in bullying has consistently been found to be negatively associated with multiple aspects of school functioning.5,35,36
Several limitations of this study should be noted. The HBSC Study covers a broad range of topics related to the health of youth. As such, in-depth information on bullying cannot be obtained. As is typical of population-based surveys of youth, data were collected during school class periods. Thus, youth who do not attend school were not represented. Surveys of this magnitude must rely on self-report data, limiting measurement of bullying to individual perceptions. To minimize differences in interpretation, however, participants were provided with a standard definition of bullying. In addition, the data are cross-sectional, and so do not indicate the direction of relationships or provide information about preceding family influence or long-term outcomes of bullying. Finally, the countries participating in the HBSC Study are primarily European and North American countries; therefore, findings from this study may not be generalized to other parts of the world.
Findings from this study suggest that the development and evaluation of programs designed to address bullying in schools are priority issues. Given the wide range of associated social and emotional correlates, influencing not only individual development but also success in the peer group and academic context, a comprehensive, systemic approach is needed to address bullying. Intervention needs to target not only the individuals who are directly involved but also the peers who may inadvertently support the bullying, and provide educators and parents with the tools to help their children and youth. Research to date on such programs provides strong evidence of their effectiveness.10,37–39 However, there is a need for randomized trials across countries and systematic reviews of the findings to fully understand how to create a school climate and changes in social norms that will substantially reduce bullying. Evaluation of programs should include program effects not only on bullying but also on psychosocial outcomes such as emotional adjustment, peer relationships, school adjustment, and occurrence of other problem behaviors. In addition to overall efforts to reduce the prevalence of bullying, particular attention should be given to bully-victims, who may be at especially high risk for maladaptive outcomes and may require more intensive intervention. Given the considerable range observed in the prevalence of bullying across countries, further research to understand the reasons for these differences is also warranted. Such research could delineate broader social and cultural factors that influence aggressive interpersonal and social behavior.
What This Study Adds.
While bullying has been shown to be a common problem across countries, direct comparison of prevalence and outcomes has not been possible because of methodologic variation across studies. This study provides an examination of the relationship between bullying and psychosocial adjustment across countries by standard measures and methods. Despite substantial variation in prevalence, there was remarkable consistency across countries in the relationship between bullying and psychosocial adjustment, with both bullies and victims demonstrating greater health problems, poorer emotional adjustment, poorer school adjustment, and higher rates of weapon carrying. Victims also reported poorer relationships with classmates, while bullies reported greater alcohol use. These findings provide strong support for the critical nature of this issue for healthy youth development internationally.
This study adds to the body of research documenting poorer psychosocial adjustment among youth involved in bullying and compares these relationships across multiple countries. The remarkable consistency across countries in the relationship between bullying and poorer psychosocial adjustment provides strong support for the critical nature of this issue for the health of youth internationally. Bullying is not only a problem that influences individuals; it transcends peer groups, communities, and countries and as such is a significant international public health issue that warrants attention.
HBSC Study and the HBSC Bullying Analyses Working Group.
The HBSC Study was performed in collaboration with the World Health Organization. The international coordinator of the 1997–1998 study was Candace Currie, PhD, University of Edinburgh, Edinburgh, Scotland, and the data bank manager was Bente Wold, PhD, University of Bergen, Bergen, Norway. This publication on the 1997–1998 HBSC Study reports on data from the following countries (principal investigators at that time are given in parentheses): Austria (Wolfgang Dür, MD), Belgium, Flemish (Lea Maes, PhD, and Els Van de Mieroop, PhD), Canada (Alan King, EdD, and William F. Boyce, PhD), Czech Republic (Ladislav Csémy, PhD), Denmark (Pernille Due, MD), England (Mary Hickman, MSc), Finland (Jorma Tynjälä, PhD), Germany (Klaus Hurrelmann, PhD), Greece (Anna Kokkevi, MD, PhD), Greenland (Michael Pedersen, MD, MPH), Hungary (Anna Aszmann, PhD), Israel (Yossi Harel, PhD), Latvia (Ieva Ranka, MD), Lithuania (Apolinaras Zaborskis, MD), Northern Ireland (Saoirse Nic Gabhainn, PhD), Norway (Oddrun Samdal, PhD), Poland (Barbara Woynarowska, PhD), Portugal (Margarida Gaspar de Matos, PhD), Republic of Ireland (Saoirse Nic Gabhainn, PhD), Scotland (Candace Currie, PhD), Slovak Republic (Miro Bronis, PhD), Sweden (Ulla Markland, PhD), Switzerland (Beatrice Janin Jacquat, PhD), United States (Peter C. Scheidt, MD, and Mary D. Overpeck, DrPH), and Wales (Chris Tudor-Smith, MSc).
The members of the HBSC Bullying Analyses Working Group are as follows: National Institute of Child Health and Human Development, Bethesda, Md:Tonja R. Nansel, PhD; Gitanjali Saluja; PhD, and June Ruan, MA. Queen’s University, Kingston, Ontario:Wendy Craig, PhD, and William Pickett, PhD. Maternal and Child Health Bureau, Health Resources and Services Administration, Rockville, Md:Mary D. Overpeck, DrPH. Universidade Técnica de Lisboa, Lisbon, Portugal: Susana Fonseca Carvalhosa, MA, and Margarida Gaspar de Matos, PhD. National Research Institute of Mother and Child, Warsaw, Poland:Joanna Mazur, PhD. Bar-Ilan University, Ramat Gan, Israel:Michal Molcho, PhD, and Yossi Harel, PhD.
References
- 1.Carney AG, Merrell KW. Bullying in schools: perspectives on understanding and preventing an international problem. Sch Psychol Int. 2001;22:364–382. [Google Scholar]
- 2.Forero R, McLellan L, Rissel C, Bauman A. Bullying behaviour and psychosocial health among school students in New South Wales, Australia: cross sectional survey. BMJ. 1999;319:344–348. doi: 10.1136/bmj.319.7206.344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wolke D, Woods S, Stanford K, Schulz H. Bullying and victimization of primary school children in England and Germany: prevalence and school factors. Br J Psychol. 2001;92:673–696. doi: 10.1348/000712601162419. [DOI] [PubMed] [Google Scholar]
- 4.Kaltiala-Heino R, Rimpela M, Rantanen P, Rimpela A. Bullying at school: an indicator of adolescents at risk for mental disorders. J Adolesc. 2000;23:661–674. doi: 10.1006/jado.2000.0351. [DOI] [PubMed] [Google Scholar]
- 5.Karatzias A, Power KG, Swanson V. Bullying and victimisation in Scottish secondary schools: same or separate entities? Aggress Behav. 2002;28:45–61. [Google Scholar]
- 6.Nansel TR, Overpeck M, Pilla RS, Ruan WJ, Simons-Morton BG. Bullying behaviors among US youth: prevalence and association with psychosocial adjustment. JAMA. 2001;285:2094–2100. doi: 10.1001/jama.285.16.2094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bond L, Carlin JB, Thomas L, Rubin K, Patton G. Does bullying cause emotional problems? a prospective study of young teenagers. BMJ. 2001;323:480–484. doi: 10.1136/bmj.323.7311.480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kumpulainen K, Rasanen E. Children involved in bullying at elementary school age: their psychiatric symptoms and deviance in adolescence. Child Abuse Neglect. 2000;24:1567–1577. doi: 10.1016/s0145-2134(00)00210-6. [DOI] [PubMed] [Google Scholar]
- 9.Olweus D. Bullying among schoolchildren: intervention and prevention. In: Peters RD, McMahon RJ, Quinsey VL, editors. Aggression and Violence Throughout the Life Span. Newbury Park, Calif: Sage Publications; 1992. pp. 100–125. [Google Scholar]
- 10.Olweus D. Bullying at school: long-term outcomes for the victims and an effective school-based intervention program. In: Huesmann LR, editor. Aggressive Behavior: Current Perspectives. New York, NY: Plenum Press; 1994. pp. 97–130. [Google Scholar]
- 11.Olweus D. Sweden. In: Smith PK, Morita Y, Junger-Tas J, Olweus D, Catalano R, Slee P, editors. The Nature of School Bullying: A Cross-national Perspective. New York, NY: Routledge; 1999. pp. 7–27. [Google Scholar]
- 12.Baldry AC, Farrington DP. Types of bullying among Italian school children. J Adolesc. 1999;22:423–426. doi: 10.1006/jado.1999.0234. [DOI] [PubMed] [Google Scholar]
- 13.Rivers I, Smith PK. Types of bullying behaviour and their correlates. Aggress Behav. 1994;20:359–368. [Google Scholar]
- 14.Austin S, Joseph S. Assessment of bully/victim problems in 8 to 11 year-olds. Br J Educ Psychol. 1996;66:447–456. doi: 10.1111/j.2044-8279.1996.tb01211.x. [DOI] [PubMed] [Google Scholar]
- 15.Berthold KA, Hoover JH. Correlates of bullying and victimization among intermediate students in the Midwestern USA. Sch Psychol Int. 2000;21:65–78. [Google Scholar]
- 16.Borg MG. The extent and nature of bullying among primary and secondary school children. Educ Res. 1999;41:137–153. [Google Scholar]
- 17.Bosworth K, Espelage DL, Simon TR. Factors associated with bullying behavior in middle school students. J Early Adolesc. 1999;19:341–362. [Google Scholar]
- 18.Boulton MJ, Underwood K. Bully/victim problems among middle school children. Br J Educ Psychol. 1992;62:73–87. doi: 10.1111/j.2044-8279.1992.tb01000.x. [DOI] [PubMed] [Google Scholar]
- 19.Olweus D. Bully/victim problems in school: knowledge base and an effective intervention program. Ir J Psychol. 1997;18:170–190. [Google Scholar]
- 20.O’Moore AM, Smith KM. Bullying behaviour in Irish schools: a nationwide study. Ir J Psychol. 1997;18:141–169. [Google Scholar]
- 21.Pellegrini AD, Bartini M, Brooks F. School bullies, victims, and aggressive victims: factors relating to group affiliation and victimization in early adolescence. J Educ Psychol. 1999;91:216–224. [Google Scholar]
- 22.Rigby K. Attitudes and beliefs about bullying among Australian school children. Ir J Psychol. 1997;18:202–220. [Google Scholar]
- 23.Whitney I, Smith PK. A survey of the nature and extent of bullying in junior/middle and secondary schools. Educ Res. 1993;34:3–25. [Google Scholar]
- 24.Currie C, Hurrelmann K, Settertobulte W, Smith R, Todd J, editors. Health and Health Behaviour Among Young People (International Report From the HBSC 1997/98 Survey) Geneva, Switzerland: World Health Organization; 2000. WHO Policy Series: Health Policy for Children and Adolescents Series, No. 1. Additional information available at: http://www.hbsc.org. [Google Scholar]
- 25.Solberg ME, Olweus D. Prevalence estimation of school bullying with the Olweus bully/victim questionnaire. Aggress Behav. 2003;29:239–268. [Google Scholar]
- 26.Kessler RC, Little RJA, Groves RM. Advances in strategies for minimizing and adjusting for survey nonresponse. Epidemiol Rev. 1995;17:192–204. doi: 10.1093/oxfordjournals.epirev.a036176. [DOI] [PubMed] [Google Scholar]
- 27.Haynie DL, Nansel TR, Eitel P, et al. Bullies, victims, and bully/victims: distinct groups of youth at-risk. J Early Adolesc. 2001;21:29–50. [Google Scholar]
- 28.Salmivalli C, Nieminen E. Proactive and reactive aggression among school bullies, victims, and bully-victims. Aggress Behav. 2002;28:30–44. [Google Scholar]
- 29.Grills AE, Ollendick TH. Peer victimization, global self-worth, and anxiety in middle school children. J Clin Child Adolesc Psychol. 2002;31:59–68. doi: 10.1207/S15374424JCCP3101_08. [DOI] [PubMed] [Google Scholar]
- 30.Marsh HW, Parada RH, Yeung AS, Healey J. Aggressive school troublemakers and victims: a longitudinal model examining the pivotal role of self-concept. J Educ Psychol. 2001;93:411–419. [Google Scholar]
- 31.O’Moore M, Kirkham C. Self-esteem and its relationship to bullying behaviour. Aggress Behav. 2001;27:269–283. [Google Scholar]
- 32.Rigby K. Peer victimisation at school and the health of secondary school students. Br J Educ Psychol. 1999;68:95–104. doi: 10.1348/000709999157590. [DOI] [PubMed] [Google Scholar]
- 33.Williams C, Chambers M, Logan S, Robinson D. Association of common health symptoms with bullying in primary school children. BMJ. 1996;313:17–19. doi: 10.1136/bmj.313.7048.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wolke D, Woods S, Bloomfield L, Karstadt L. Bullying involvement in primary school and common health problems. Arch Dis Child. 2001;85:197–201. doi: 10.1136/adc.85.3.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nansel TR, Haynie DL, Simons-Morton BG. The association of bullying and victimization with middle school adjustment. J Appl School Psychol. 2003;19(2):45–61. [Google Scholar]
- 36.Natvig GK, Albrektsen G, Qvarnstrom U. School-related stress experience as a risk factor for bullying behavior. J Youth Adolesc. 2001;30:561–575. [Google Scholar]
- 37.Olweus D, Limber S, Milhalic S. Blueprints for Violence Prevention, Book Nine: Bullying Prevention Program. Boulder, Colo: Center for the Study of Prevention of Violence; 1999. [Google Scholar]
- 38.Sharp S, Smith PK. Bullying in UK schools: the DES Sheffield Bullying Project. Early Child Dev Care. 1991;77:47–55. [Google Scholar]
- 39.Smith PK. Bullying in schools: the UK experience and the Sheffield Anti-Bullying Project. Ir J Psychol. 1997;18:191–201. [Google Scholar]