

Abstract
Background
Torsional joint stiffness is thought to play in role in the observed sex bias in noncontact ACL injury rates.
Hypothesis
Females will exhibit lower torsional stiffness values of the knee in response to varus/valgus and internal/external rotations than males.
Study Design
Descriptive Laboratory Study.
Methods
Knee kinematics of 20 university students (10 males, 27.3 ± 3.4 yrs, 177.3 ± 6.8 cm, 81.1 ± 7.0 kg; 10 females, 22.9 ± 1.5 yrs, 169.0 ± 7.1 cm, 66.1 ± 11.4 kg) were measured while 0-10 Nm of varus and valgus torques were applied with the subject non-weightbearing (NWB) and when 0-5 Nm of internal and external torques were applied with the subject NWB and weightbearing (WB) with the use of a custom joint testing device. Joint stiffnesses values were calculated at 1 Nm increments.
Results
When low magnitudes of torque were applied to the knee, females had significantly lower stiffness values than males. With the exception of applied external torque with the joint WB and varus torque with the joint NWB, females demonstrated an increase in joint stiffness as the magnitude of torque increased from lower to higher magnitudes. In contrast, for the males, joint stiffness values remained unchanged as the magnitude of applied torque increased.
Conclusions
Females exhibited lower knee stiffness in response to low magnitudes of applied torque compared to males, and demonstrated an increase of joint stiffness as the magnitude of applied torque increased.
Clinical Relevance
The decreased stiffness behavior of the knee in response to low torques that was observed for females may have a role in detrimentally impacting knee biomechanics and resulting neuromuscular function, particularly when an individual transition from non-weightbearing to weightbearing.
Key Terms: Knee, biomechanics, incremental stiffness reliability
Introduction
Joint stiffness is a biomechanical parameter that characterizes the deformation of the soft tissue structures connecting one bone to another in response to applied load or torques. It is considered to have implications for both performance and for injury.[4] Human knee joint stiffness can be represented as a torsional spring[7] which can be described through mechanical means. Stiffness of the knee in response to torques that flex and extend the joint (sagittal plane stiffness) have been included in studies of overall leg spring stiffness[1;6;7]; however, less is known about stiffness of the knee in response to varus (VR), valgus (VL), internal (INT), and external (EXT) torques.[3;9;11;12] Anterior cruciate ligament (ACL) injury has been associated with valgus and external torques about the knee [14], and consequently stiffness characteristics in response to these torques may be important to examine relative to the sex bias in the incidence rate of ACL injury.[9]
There appears to be a paucity of studies that compare VR/VL and INT/EXT torsional knee stiffness between males and females. In cadaver studies it has been demonstrated that females have decreased knee stiffness compared to males when combined torques of 10 Nm valgus and ±5 Nm transverse plane tibial torque.[9] However, it remains unclear if there are sex differences in VR/VL or INT/EXT torsional stiffness in-vivo in the healthy, intact knee joint. Additionally, reported stiffness curves have traditionally been presented as two phases. This two-phase, or breakpoint, analysis,[9;13;17] is defined by a phase of “laxity” during low loads and a stiffness calculated as the slope of the load-displacement curve from the end of the “laxity” phase to a maximal applied load. Due to different ranges of applied load and tangent point choices in analysis of these curves, the use of a two-phase stiffness model, though widely accepted, may be limited in its generalizability of overall knee biomechanics.
Further, there is a possibility that examining stiffness only as the inverse of laxity, which is displacement in response to fixed load limits, may conceal important physiologic information. For example, in earlier work we have reported that females who demonstrate greater anterior knee laxity also demonstrate greater frontal and transverse plane knee joint laxity compared to males.[23] Examining the overall stiffness of this range would yield little new information. However, by gaining a more thorough understanding of stiffness throughout the load-displacement range, we may better determine where in the measured displacement range that the knee joint is more stiff (e.g. more resistive to applied loads or torques), and conversely, where the knee is less stiff (e.g. less resistive to applied loads or torques). In turn, this may help us better understand the sex dependent factors that may influence knee behavior during physiological loading conditions.
Thus, the purposes of this study were 1) to determine stiffness values for each 1.0 Nm of applied VR/VL (NWB) and INT/EXT (NWB and WB) torques and characterize the day-to-day measurement consistency of these stiffness values obtained from subjects with healthy knees in vivo, and 2) to compare these stiffnesses between males and females. It was hypothesized that given greater laxity values observed in females compared to males, females would also exhibit lower incremental stiffness values compared to males at some point in the range of applied torques.
Materials and Methods
Data for this study were obtained from a larger project examining the clinical usefulness of the Vermont Knee Laxity Device (VKLD; University of Vermont, Burlington, VT) to examine knee joint behavior in males and females[22;23], and consisted of twenty university students (10 males, 27.3 ± 3.4 yrs, 177.3 ± 6.8 cm, 81.1 ± 7.0 kg; 10 females, 22.9 ± 1.5 yrs, 169.0 ± 7.1 cm, 66.1 ± 11.4 kg) were recruited. Whereas previous worked reported on the capability of the VKLD to measure frontal and transverse plane laxity of the knee and compared these values in males and females [22;23], the current investigation is focused on reporting the incremental stiffnesses derived during applied VR/VL (NWB) and INT/EXT (NWB and WB) torques from the obtained data set. Subjects were included if they had no history of knee ligament injury or surgery, no history of injury or chronic pain in both lower extremities within 6 months of enrollment into the study, and were otherwise healthy. Subjects read and signed a consent form that had been approved by the Institutional Research Board prior to data collection.
In order to establish the reliability of the incremental stiffness data obtained, the first 10 subjects (5 males, 5 females) were asked to participate in a second identical data collection session within 24 to 48 hours of the initial test session. Data were collected from both the left and right knees.
Prior to data collection, electromagnetic position sensors (Mini Birds, Ascension Technologies, Colchester, VT) were attached to the lateral aspect of the thigh (just proximal to the thigh clamp portion of the VKLD along the iliotibial band) and to the tibial shaft (distal to the shank strap) to measure knee motion. Hip, knee, and ankle joint centers were determined and segmental coordinate systems were constructed as previously described.[22]
Knee stiffnesses in response to VR/VL and INT/EXT torques were measured with the VKLD. In previous work, we have described in detail the measurement procedures for VR/VL and INT/EXT knee testing[22]. The first limb tested (left/right) and first direction of applied torque (i.e. VR versus VL, or INT versus EXT) were counterbalanced across all subjects. All testing began with application of VR/VL torques while the subject was NWB, followed by application of INT/EXT torques while the subjected was NWB, and then INT/EXT torques while the subject was WB (defined as a compressive load of 40% body weight applied to the foot). This 40% load was chosen to replicate the double leg stance loading condition (with 50% bodyweight on each leg minus the approximately 10% of bodyweight located below the knee).[21] The subject was supinely positioned in the VKLD at 20° knee flexion. With the thigh securely fixed and the foot and ankle tightly restrained in the foot cradle, counterweights were applied to the thigh and shank to create an initial condition of zero shear and compressive loads across the tibiofemoral joint (Figure 1). For VR/VL, an external force was applied to the lateral and medial aspects of the distal tibia using a hand held force transducer (Model SM-50, Interface, Scottsdale, AZ) to produce the limits of 10 Nm VR and VL torque at the knee (Figure 2), respectively. INT and EXT torques were applied about the long axis of the tibia to the limit of 5 Nm using a T-handle connected to a six degree-of-freedom (6 DOF) force transducer (Model MC3A, Advanced Medical Technology, Inc; Watertown, MA) affixed to the foot cradle (Figure 3). Following three familiarization trials, three loading cycles were collected for each motion.
Figure 1.

Vermont Knee Laxity Device.
Figure 2.
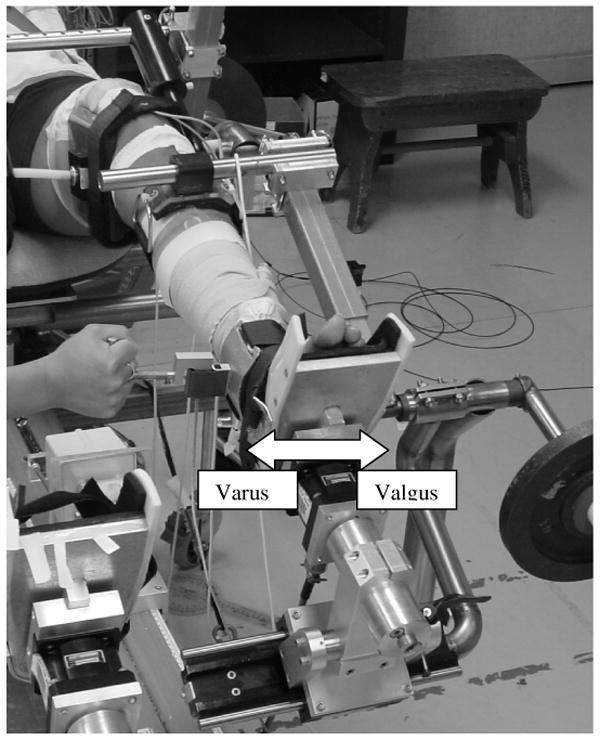
A hand-held force transducer applied resistance to the medial and lateral aspect of the distal tibia to create a 10 Nm varus and valgus torque at the knee.
Figure 3.
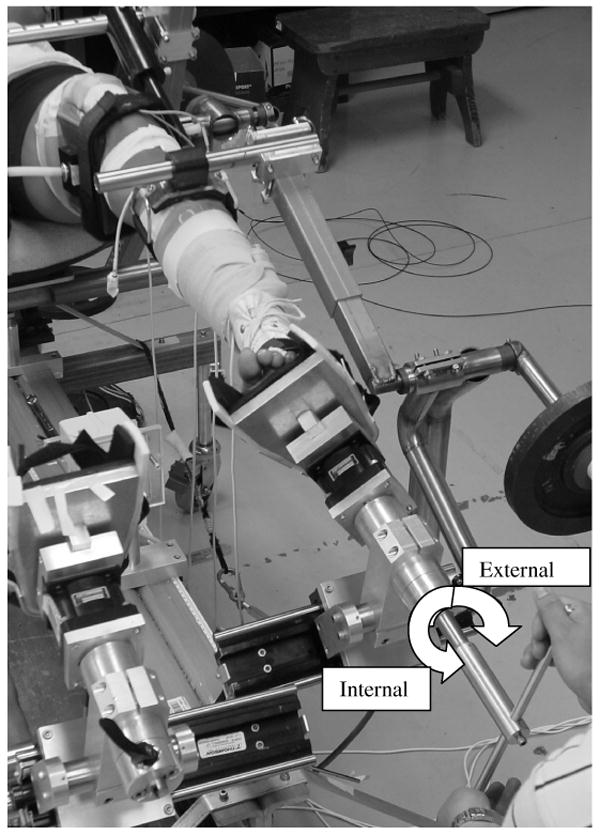
Internal and external rotation torques from 0-5 Nm were applied to the knee using a T-handle connected to a six degree-of-freedom force transducer firmly fixed to the foot cradle.
Signals from all force transducers and electromagnetic position sensors were interfaced with the data collection software (Motion Monitor, Innovative Sports Training; Chicago, IL) to allow simultaneous collection of force and displacement measures at 100 Hz. Signals from the position sensors and both handheld and 6DOF force transducers were low-pass filtered at 10 Hz and 20Hz respectively, using a 4th order zero lag Butterworth filter. For each segment, the +Y axis was directed superiorly, the +Z axis directed laterally for the right leg and medially for the left leg, and the +X axis directed anteriorly. Euler's equations describe knee joint motion using a rotational sequence of Z Y′ X″.[10]
Data Reduction
To form torque-displacement curves, displacements at each 0.1 Nm of applied torque were plotted for each trial. For each condition the displacements for each of three trials were averaged at each 0.1 Nm torque increment. This yielded an ensemble torque-displacement curve for each subject, for each test condition.
Each ensemble curve was then divided into increments of 1.0 Nm torques (e.g. 1-2, 2-3, 3-4 Nm etc.). For each increment, an incremental stiffness was calculated as the change in applied torque divided by the change in displacement (Nm/°). This resulted in 10 incremental stiffnesses for the VR loadings (0-10 Nm), 10 for the VL loading, 5 incremental stiffnesses for INT loading (0-5 Nm) and 5 for EXT loading.
Data Analyses
Upon close inspection of the incremental stiffness data it was revealed that during VL and VR loading that the stiffness values obtained from the 0-1Nm increment were abnormally high when compared to the average stiffness values obtained for applied torques between 1 and 10Nm (VL = 11.57 vs 2.17 Nm/deg (8 standard deviations greater) & VR = 21.37 vs 2.34 Nm/deg; (14 standard deviations greater)). These abnormally high values were attributed to overcoming any static friction in the device and limb rotational inertia at the point of loading during initial loading. These factors would all result in little to no bony segment movement with the onset of applied loading, thus giving the abnormally high stiffness values. Based on this, the 0-1Nm increment was eliminated from the valgus and varus analyses. This phenomenon was not observed for INT/EXT measures, likely due to the fact of less rotational inertia about the longitudinal axis of the tibia.
Further, a few individual subjects recorded incremental stiffnesses that were negative (a physiologic impossibility) during a loading condition, and therefore the subject was eliminated from the respective statistical analyses. These negative stiffness values were likely the result of uneven manual application of loads or inadvertent muscle guarding produced by the study participant. This consideration resulted in the elimination of 1 female and 2 males for varus loading (N=34 total remaining knees), which in turn resulted in the elimination of 2 subjects from the varus measurement consistency analysis. All other conditions retained the full complement of subjects.
In an effort to evaluate the first aim of our study and determine the between day measurement consistency of incremental stiffness values for the first 10 subjects, separate repeated measures ANOVA for each direction and condition [VL, VR, INT (WB and NWB), and EXT (WB and NWB)], increment of applied torque (1-10 VR/VL, 0-5 INT/EXT), and side were used to calculate intraclass correlation coefficients (ICC2,k) and standard errors of measurement (SEM).
To evaluate the second aim of our study and determine the effect of sex on knee stiffness, six separate repeated measures ANOVAs were performed for VL, VR, INT (WB & NWB), and EXT (WB & NWB) incremental stiffness values, with sex as the between subjects factor, and side (R/L) and increment of applied torque as the within subject factor. The alpha level was set a priori at P<0.05 and Tukey's Post hoc testing was used. Given the relatively small sample size, effect sizes were calculated for significant and non-significant sex differences.
Results
Measurement Consistency
Median and ranges for ICC values and standard errors of measurements for each loading condition are found in Table 1. VL, VR, and EXT-WB all demonstrated median ICCs that were acceptable (range: 0.66 - 0.81). INT-NWB, EXT-NWB and INT-WB median ICC values were lower (range: -0.15 - 0.75). Although only the ranges are presented here, it is important to note that there was a general trend in the data that ICC values typically were lower during the higher loading ranges.
Table 1.
Incremental Stiffness Medians and Ranges of Day-to-Day Intraclass Correlation Coefficients and Standard Errors of Measurement.
| ICC(2,k) | SEM (Nm/deg) | |||
|---|---|---|---|---|
| Median | Range | Median | Range | |
| Valgus | ||||
| Right | .80 | 49 - .91 | .51 | .37 – 2.87 |
| Left | .80 | .48 - .91 | .41 | .29 - .41 |
| Varus | ||||
| Right | .81 | .53 -.90 | .72 | .41 - .99 |
| Left | .66 | -.22 - .87 | .63 | .30 – 1.12 |
| INT-NWB | ||||
| Right | .54 | .26 - .84 | .23 | .13 - .54 |
| Left | -.07 | -.28 - .40 | .73 | .21 - .98 |
| EXT-NWB | ||||
| Right | .44 | .42 - .74 | .33 | .22 - .40 |
| Left | .75 | .69 - .92 | .08 | .07 - .14 |
| INT-WB | ||||
| Right | .59 | -.41 - .82 | .58 | .37 - .92 |
| Left | -.15 | -.47 - .71 | 2.09 | 1.44 – 4.51 |
| EXT-WB | ||||
| Right | .76 | .60 - .83 | .20 | .18 - .34 |
| Left | .72 | .71 - .79 | .33 | .23 - .91 |
Sex Comparisons
VL incremental stiffness differed by sex and increment of applied torque (F8,144=2.68, p=.009). The VL incremental stiffness values obtained from the females were less than those obtained from the males for applied torques between 1 and 4 Nm (effect sizes = 0.74 – 1.14). However, the incremental stiffness values between males and females were not significantly different for torques between 4 Nm and 10 Nm (effect sizes ranging from 0.08 – 0.57). For the females VL incremental stiffness increased as the magnitude of applied torque increased from 2-3 Nm to 9-10 Nm. In contrast, male incremental stiffness values remained unchanged across these same torque magnitudes. (Figure 4)
Fig. 4.

Valgus torsional stiffnesses of the knee for males and females (mean ± SD). * Males' stiffness value significantly greater than females. † Females' stiffness significantly greater than the lowest stiffness value for females.
The VR incremental stiffness was less in females than the males (F1,15=10.62, p=.005, effect size = .30), and this was not dependent on magnitude of applied torque. (Figure 5)
Fig. 5.

Varus torsional stiffnesses of the knee for males and females (mean ± SD). Main effect for male stiffness being greater than female stiffness.
For INT incremental stiffness with the knee unweighted, a significant interaction between sex and increment of applied torque (F4,72=6.41, p<.001) revealed that females had lower stiffness values in response to 0-1 Nm of torque (effect size = .98) but greater stiffness values for 3-5 Nm of applied torque compared to males (effect sizes = 0.59 – 0.65). (Figure 6) No sex differences were observed between 1 and 3 Nm of applied torque (effect sizes = 0.24 – 0.33) This interaction was primarily due to females demonstrating increased knee stiffness values as the applied torques increased from 0-1 Nm to 3-5 Nm while male incremental stiffness values remained unchanged across these same increments of torque.
Fig. 6.

Internal torsional stiffnesses with the joint unweighted of the knee for males and females (mean ± SD). * Stiffness value for one sex significantly greater than other at applied torque increment. † Females' stiffness significantly greater than the lowest stiffness value for females
For EXT incremental stiffness with the knee unweighted a significant interaction between sex and increment of applied torque (F4,72=3.00, p=.02) again demonstrated lower stiffness values in females for 0-1 Nm of applied torque (effect size = 1.18) (Figure 7). No sex differences were observed an between 1 -5 Nm of applied torque (effect sizes = 0.00 – 0.41) As with INT, females' stiffness values increased as the magnitude of torque increased from 0-1 Nm to 3-5 Nm, while male stiffness values remained unchanged in response to these same torques.
Fig. 7.

External torsional stiffnesses with the joint unweighted of the knee for males and females (mean ± SD). * Males' stiffness value significantly greater than females. † Females' stiffness significantly greater than the lowest stiffness value for females.
During the INT with the knee weightbearing, an interaction between sex and increment of applied torque was observed (F4,72=3.45, p=.01), revealing female knee stiffness was less than male stiffness from 0-2 Nm of applied torque (effect sizes = 0.61-0.99). (Figure 8). No sex differences were observed for torque magnitudes between 2 and 5 Nm (effect sizes = 0.21 – 0.26) The stiffness values for the females increased from 0-1 Nm to 4-5 Nm while stiffness was unchanged for the males.
Fig. 8.

Internal torsional stiffnesses with the knee weightbearing for males and females (mean ± SD). * Males' stiffness values significantly greater than females. † Females' stiffness significantly greater than the lowest stiffness value for females.
In EXT with the knee weightbearing an interaction between sex and increment of applied torque (F4,72=2.75, p=.04) revealed females were less stiff than males from 0 – 3 Nm of applied torque (effect sizes = 0.53-1.11). (Figure 9). No sex differences were observed between 3 -5 Nm of applied torque (effect sizes = 0.06 – 0.41) Stiffness values in both females and males remained relatively unchanged across force increments, with the exception of the initial force increment in males (0-1Nm), which was slightly higher than their stiffness at the 4-5Nm increment.
Fig. 9.

External torsional stiffnesses with the knee weightbearing for males and females. * Males' stiffness value significantly greater than females. † Male knee stiffness greater than the least male stiffness mean.
Discussion
This study introduces the use of the VKLD to quantify incremental stiffness values of the knee in response to VR-VL and INT-EXT torques in-vivo. Our primary findings confirm that consistent measures can be obtained from one day to the next, and that females generally exhibited lower knee stiffness in response to low magnitudes of applied torque compared to males, and demonstrated an increase of joint stiffness as the magnitude of applied torque increased. The discussion will first address our measurement consistency, and then explore the implications of the sex differences observed.
Measurement Consistency
Across the entire loading cycle, VL, VR, and EXT - WB median incremental stiffness values were the most consistent measures from day-to-day (ICC2,k Median = 0.66 -0.81.) (table 1). For INT, EXT, and INT during WB, the of ICC2,k median was much lower (range = -.15 - .75) (table 1). A detailed examination of the sources of variance used in the calculation of individual incremental reliability coefficients revealed that lower ICC values were due to both decreased variability between subjects and increased random error as INT and EXT torque magnitudes increased. Additionally the INT WB condition revealed the ratio of random error relative to the between subjects variability increased as the magnitude of torque increased. The increased random error associated with lower reliability coefficients observed at higher torque ranges for the INT, EXT, and INT during WB conditions could be explained by various involuntary muscle guarding responses invoked by the subjects in response to higher loads and the fact that variability in the joint stiffness values decreases between study subjects at higher magnitudes of torque. Although every attempt was made to insure that the subject was relaxed and did not activate their muscles during the NWB conditions, it is possible that subjects may have reacted to the applied loads with different strategies. It is reasonable to assume that if the study participants guarded by contracting their leg muscles, they would do so in ways that would diminish reliability. Additionally, through qualitative assessment, these torques often felt the most “unnatural” to the subjects, and this may have created the potential for more neuromuscular guarding. It is important to note that in our previous work addressing knee laxity of the loading conditions derived from this same data set, that ICCs, with the exception of INT-WB (.20 - .32), ranged between good and excellent (.68 - .96).[22;23] When studying these smaller incremental stiffnesses it is not surprising there is an inherent difficulty in obtaining more precise, reliable measures.
The occurrence of greater reliability when low magnitudes of torque were applied to the knee is important to the discussion of male/female stiffness differences that were observed. Where reliability is decreased due to increased measurement error, meaningful differences in stiffness would be more difficult to detect in the high torque ranges, and our findings should be viewed in that light. Due to the inability to locate other studies that have reported within day or between day measurement consistencies for stiffness values, we are unable to compare our reliability results with previous work.
Differences in Incremental Stiffness by Sex
The main finding of this study is that in response to low magnitudes of torque applied to the tibiofemoral joint stiffness values measured from the females were less than those of the males. During VL and VR testing it has been reported that females have, on average, knee stiffness values that are 35% less than males.[3]. Although this same observation was noted throughout our VR testing, females were less stiff than males only between 1-4 Nm during VL testing. This finding suggests that quantifying an overall stiffness of the knee, as defined by large magnitude of torque, may not allow a complete understanding of the biomechanical behavior of the knee.
Similar sex differences were noted in response to low magnitudes of torque for all INT and EXT incremental stiffnesses from 0-1 Nm. Cadaver work has shown that females have significantly lower torsional stiffness of the knee (as defined as the slope of the torque-displacement relationship between 2.5 and 5 Nm of internal tibial torque with a simultaneous 10 Nm valgus torque).[9] The current study identified that in response to low torques (0-1 Nm) the INT and EXT stiffnesses were less for the females compared to the males' and as the magnitude of torque increased (3-5 Nm) there were similar stiffness values between males and females. While the differences between the current study and previously reported work are likely produced by methodological differences (i.e. unidirectional versus multidirectional loading responses), these studies appear to be consistent in reporting decreased female joint stiffness in comparison to males.
The incremental stiffness values obtained in the current study are similar to previous reports.[3;12] Although invivo comparisons are few, the VL (range: 1.23-3.49 Nm/deg) and VR (range: 1.36-3.73 Nm/deg) incremental stiffness values obtained with the knee NWB are comparable to terminal or overall VL and VR stiffness previously reported as 3.05±1.02 Nm/deg and 2.94±.89 Nm/deg, respectively.[3] It must be noted that this prior study applied a 20 Nm torque with the knee extended (at about 0 deg flexion) while our study applied a 10 Nm torque with the knee at 20 deg flexion. Our study was limited to a 10 Nm threshold, as we have found that study subjects cannot maintain relaxed muscles beyond this magnitude of applied torque. In-vivo comparison to our NWB INT (range: 0.26-1.01 Nm/deg) and EXT (range: 0.26-0.58 Nm/deg) incremental stiffness values reveals similar stiffness at 5 Nm NWB INT and EXT as 0.57±.12 Nm/deg and 0.56±.12 Nm/deg, respectively.[12] We have been unable to locate previous in-vivo INT and EXT stiffnesses with the knee weightbearing.
To the best of our knowledge, this is the first study that has attempted to quantify incremental stiffness values of the knee in response to applied torques. With the exception of WB EXT stiffness (the finding of decreased male stiffness in this condition from low to high magnitudes of torque is puzzling but likely the result of both slight malalignment of VKLDs INT-EXT axis of rotation relative to the tibias longitudinal axis of rotation and slightly more static friction in the system experienced during the weightbearing condition) females demonstrated an increase of joint stiffness as the magnitude of torque increased from low to high magnitudes while the males' stiffness values were unchanged across the same torque magnitudes. Combined with the result of decreased female compared to male stiffness for low torque magnitudes, the tissue response suggests females have decreased stiffness in response to low loads followed by increasing incremental stiffness values similar to, and in some cases exceeding male values at higher loads. Possible explanations for these differences in joint stiffness values between males and females include differences in the material properties of the ligaments and geometry of the tibiofemoral joint.
This sex-specific tissue response to increasing loads fit well with the previous work of Markolf et al. 1984, who suggested that during diagnostic anterior/posterior knee joint laxity evaluation the examiner should “feel low” when assessing the stiffness of the joint.[12] It was suggested that anterior stiffness changes were best noticed in response to low load levels.[12] Given the current findings, it is possible that a similar suggestion is applicable to the testing VR/VL and EXT/IR motions of the knee joint.
Previous work by our group demonstrated that females exhibited significantly greater VR/VL and INT/EXT laxities than males.[23] Although laxity is also a useful measure to assess joint function, stiffness simply reported as the inverse of an overall laxity measure (also described as compliance) may not provide a complete picture of subtle sex differences during the loading process whereas the observed sex differences in incremental stiffness values may increase our understanding of sex-specific joint function. While joint stiffness appears to be a function of the magnitude of applied torque for females (through increasing stiffness values across the loading cycle), it appears to be less important in determining joint stiffness for males. Thus, the way in which one defines stiffness (e.g. the magnitudes of applied toques that are chosen to measure displacement) has an effect on the data and ultimately the outcome of the analysis.
It is important to note that our approach of measuring stiffness at smaller increments of torque allowed us to demonstrated sex specific effects at low torque magnitudes but not at high torques. If the study followed previously reported methods and only measured stiffness in response to high torques,[9] a sex effect may not have been found. Although many different techniques could have been used to analyze the data (e.g. a logistic fit or polynomial fit to the data) allowing us to comparing the coefficients or slopes of these fits between sexes, we feel that our current approach allowed us to characterize and ultimately understand joint stiffness behaviors throughout the entire loading cycles. With this approach, a more comprehensive description of joint biomechanics was obtained.
Clinical Implications
Studies of ACL injury mechanisms typically describe an injury that occurs at or near foot strike with the knee near full extension.[2;14] The observation that females have lower knee stiffness values in comparison to males when low magnitudes of torque are applied may have important implication when impulsive loads are transmitted across the joint during the onset of weight bearing. For example, research has shown that during the transition from non-weight bearing to weight bearing, there is an anterior translation of the tibia relative to the femur that is restrained by the ACL and this translation is greater in those with increased knee laxity.[21] While these prior findings are restricted to the A-P direction, they suggest that during common athletic tasks such as the heal strike phase of gait, when landing from a jump, or during a plant and cut maneuver decreases in knee stiffness may be associated with alterations in early joint positioning that could produce corresponding effects on the sequence and magnitude of muscle contractions.[9] This, in turn, could produce sex differences in neuromuscular strategies for controlling potentially injurious motion. Given the recent finding of a valgus mechanism of ACL injury[8], our observation of decreased female knee stiffness in response to valgus torques highlights the need for alternate strategies of neuromuscular control in order to augment joint stiffness and protect the knee ligaments. Studies examining sex differences in neuromuscular recruitment have demonstrated that females activate their muscles sooner[5;20] in response to perturbing activities that have been reported to include components of valgus and external rotations of the tibia relative to the femur.[16] The finding that females activate their muscles sooner in response to a perturbation may be a neuromuscular adaptation to the decreased joint stiffness for females as demonstrated in the current study. This contention is supported by studies that have observed increased muscle activation (both preparatory and reactive), particularly in the lateral hamstrings, during weight bearing activity in females who have greater knee laxity values.[15;18] It may also be an adaptation to help mitigate the increased stiffness values that were associated with high magnitudes of torque during NWB VL, NWB INT/EXT, and WB EXT loadings.
Limitations
Although great care was taken to control all aspects of the study, several limitations exist. While extensive pilot testing was performed to ensure the most stable sensor position possible, it should be recognized that the superficial skin markers used may not exactly represent true skeletal motion. This same concern exists for all approaches that attempt to measure lower limb biomechances with the use of external markers attached to the skin. Further, while the same examiner applied torques in a consistent manner, the torque loading rate was controlled by the investigator and was not mechanically standardized. It should also be noted that the 40% body weight load used is well below bodyweight loads incurred during dynamic activity (e.g. walking, running), thus our weight bearing results should be viewed in reference to the foot contact that occurs during the early foot phase of weight acceptance. Finally, the efforts undertaken to control for neuromuscular effects on stiffness included verbal instructions, practice trials for acclimation of subjects, and visual observation on the part of the researcher; however, EMG data were not included, and therefore the level of muscular activation was not documented.
Additionally, certain subject characteristics were not controlled that may influence the data. Hormone level or cycle phase in females was not documented for day to day reliability testing. As ligamentous laxity has been shown to be affected by fluctuations in hormone levels[19], it is possible that small fluctuations in joint laxity could have occurred between repeat measures taken within 24-48 hours of the first test session, and in turn affected the reliability of incrementally derived stiffness measurement between days. Although subjects were carefully questioned to ascertain the health history of their knees and lower extremity, a formal knee exam was not performed to screen out any potential joint abnormalities nor was level of physical activity controlled.
Reference List
- 1.Arampatzis A, Bruggemann GP, Metzler V. The effect of speed on leg stiffness and joint kinetics in human running. J Biomech. 1999;32:1349–1353. doi: 10.1016/s0021-9290(99)00133-5. [DOI] [PubMed] [Google Scholar]
- 2.Boden BP, Dean GS, Feagin JA, Garrett WE. Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23:573–578. doi: 10.3928/0147-7447-20000601-15. [DOI] [PubMed] [Google Scholar]
- 3.Bryant JT, Cooke TD. Standardized biomechanical measurement for varus-valgus stiffness and rotation in normal knees. J Orthop Res. 1988;6:863–870. doi: 10.1002/jor.1100060610. [DOI] [PubMed] [Google Scholar]
- 4.Butler RJ, Crowell HP, 3, Davis IM. Lower extremity stiffness: implications for performance and injury. Clin Biomech (Bristol, Avon) 2003;18:511–517. doi: 10.1016/s0268-0033(03)00071-8. [DOI] [PubMed] [Google Scholar]
- 5.Carcia CR, Shultz SJ, Granata KP, Gansneder BM, Perrin DH. Knee ligament behavior following a controlled loading protocol does not differ by menstrual cycle day. Clin Biomech (Bristol, Avon) 2004;19:1048–1054. doi: 10.1016/j.clinbiomech.2004.07.006. [DOI] [PubMed] [Google Scholar]
- 6.Dutto DJ, Braun WA. DOMS-associated changes in ankle and knee joint dynamics during running. Med Sci Sports Exerc. 2004;36:560–566. doi: 10.1249/01.mss.0000121957.83226.cc. [DOI] [PubMed] [Google Scholar]
- 7.Farley CT, Houdijk HHP, Strien CV, Louie M. Mechanism of leg stiffness adjustment for hopping on surfaces of different stiffnesses. J Appl Physiol. 1998;85:1044–1055. doi: 10.1152/jappl.1998.85.3.1044. [DOI] [PubMed] [Google Scholar]
- 8.Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc. 2003;35:1745–1750. doi: 10.1249/01.MSS.0000089346.85744.D9. [DOI] [PubMed] [Google Scholar]
- 9.Hsu WH, Fisk JA, Yamamoto Y, Debski RE, Woo SL. Differences in torsional joint stiffness of the knee between genders: a human cadaveric study. Am J Sports Med. 2006;34:765–770. doi: 10.1177/0363546505282623. [DOI] [PubMed] [Google Scholar]
- 10.Kadaba MP, Ramakrishnan HK, Wootten ME, Gainey J, Gorton G, Cochran GV. Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. J Orthop Res. 1989;7:849–860. doi: 10.1002/jor.1100070611. [DOI] [PubMed] [Google Scholar]
- 11.Markolf KL, Bargar WL, Shoemaker SC, Amstutz HC. The role of joint load in knee stability. J Bone Joint Surg Am. 1981;63:570–585. [PubMed] [Google Scholar]
- 12.Markolf KL, Kochan A, Amstutz HC. Measurement of knee stiffness and laxity in patients with documented absence of the anterior cruciate ligament. J Bone Joint Surg Am. 1984;66:242–252. [PubMed] [Google Scholar]
- 13.Markolf KL, Mensch JS, Amstutz HC. Stiffness and laxity of the knee--the contributions of the supporting structures. A quantitative in vitro study. J Bone Joint Surg Am. 1976;58:583–594. [PubMed] [Google Scholar]
- 14.Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32:1002–1012. doi: 10.1177/0363546503261724. [DOI] [PubMed] [Google Scholar]
- 15.Rozzi SL, Lephart SM, Gear WS, Fu FH. Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. The American Journal of Sports Medicine. 1999;27:312–319. doi: 10.1177/03635465990270030801. [DOI] [PubMed] [Google Scholar]
- 16.Schmitz RJ, Shultz SJ, Kulas AS, Windley TC, Perrin DH. Kinematic analysis of functional lower body perturbations. Clin Biomech (Bristol, Avon) 2004;19:1032–1039. doi: 10.1016/j.clinbiomech.2004.07.012. [DOI] [PubMed] [Google Scholar]
- 17.Shoemaker SC, Markolf KL. In vivo rotatory knee stability. Ligamentous and muscular contributions. J Bone Joint Surg Am. 1982;64:208–216. [PubMed] [Google Scholar]
- 18.Shultz SJ, Carcia CR, Perrin DH. Knee joint laxity affects muscle activation patterns in the healthy knee. J Electromyogr Kinesiol. 2004;14:475–483. doi: 10.1016/j.jelekin.2003.11.001. [DOI] [PubMed] [Google Scholar]
- 19.Shultz SJ, Kirk SE, Johnson ML, Sander TC, Perrin DH. Relationship between sex hormones and anterior knee laxity across the menstrual cycle. Med Sci Sports Exerc. 2004;36:1165–1174. doi: 10.1249/01.MSS.0000132270.43579.1A. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shultz SJ, Perrin DH, Adams MJ, Arnold BL, Gansneder BM, Granata KP. Neuromuscular Response Characteristics in Men and Women After Knee Perturbation in a Single-Leg, Weight-Bearing Stance. J Athl Train. 2001;36:37–43. [PMC free article] [PubMed] [Google Scholar]
- 21.Shultz SJ, Shimokochi Y, Nguyen AD, et al. Nonweight-bearing anterior knee laxity is related to anterior tibial translation during transition from nonweight bearing to weight bearing. J Orthop Res. 2006;24:516–523. doi: 10.1002/jor.20040. [DOI] [PubMed] [Google Scholar]
- 22.Shultz SJ, Shimokochi Y, Nguyen AD, Schmitz RJ, Beynnon BD, Perrin DH. Measurement of Varus-Valgus and Internal-External Rotational Knee Laxities In-Vivo Part I: Assessment of Measurement Reliability and Bilateral Asymmetry Asymmetry. J Ortho Res. 2007 doi: 10.1002/jor.20397. In Press. [DOI] [PubMed] [Google Scholar]
- 23.Shultz SJ, Shimokochi Y, Nguyen AD, Schmitz RJ, Beynnon BD, Perrin DH. Measurement of Varus-Valgus and Internal-External Rotational Knee Laxities In-Vivo Part II: Relationship with Anterior-Posterior and General Joint Laxity in Males and Females. J Ortho Res. 2007 doi: 10.1002/jor.20398. In Press. [DOI] [PubMed] [Google Scholar]