

Abstract
Foreign body ingestion is a common occurrence in childhood. We report the outcome of an infant who swallowed a piece of glass. The absence of a foreign body on chest radiograph led to delayed diagnosis and then to the well documented complications of retropharyngeal abscess and mediastinitis. She was admitted to the paediatric intensive care unit a week after her initial presentation, subjected to multiple invasive and non‐invasive procedures, and 6 weeks after her initial presentation to the accident and emergency department, was discharged back to her referring hospital having re‐established oral feeds.
Keywords: retropharyngeal, abscess, x ray, foreign body
A glass jar of baby food fell and broke on a kitchen floor. Some hours later, a child in the house, a 1 year old girl, was found surrounded by broken glass and bleeding from the mouth. On arrival in the emergency department (ED) there was no obvious bleeding or laceration, and the child was sleeping comfortably without respiratory distress. An anterior–posterior chest radiograph was reported as normal with no visible foreign body. The parents were reassured and returned home.
Two days later, the child was admitted via the ED with a fever of 39.5°C and mild dehydration. She was drooling saliva, had submandibular swelling and tenderness, and cervical lymphadenopathy, but no respiratory compromise. She was rehydrated, a septic screen was performed, and cefotaxime was prescribed for an upper respiratory tract infection.
The following day the fever persisted. The child continued to drool saliva and was no longer able to eat solids. An ear, nose, and throat (ENT) examination showed no further abnormalities on oral examination and she continued to receive cefotaxime. Four days after initial presentation she developed mild inspiratory stridor and altered her posture to maintain her airway by leaning to one side. An ultrasound scan of the neck confirmed the clinical suspicion of retropharyngeal abscess and she was referred for tertiary ENT management.
On arrival, she needed fluid resuscitation and inotropic support for septic shock. She was stabilised and an urgent computer tomography (CT) scan revealed a large retropharyngeal abscess tracking down to the mediastinum (fig 1A). During surgery, a left sided retropharyngeal abscess extending across the midline and down to the aortic arch with free pus in the oesophagus was drained and a drain left in the cavity. No foreign body was identified. She was transferred back to the paediatric intensive care unit (PICU) under sedation, muscle relaxant, and ventilation.
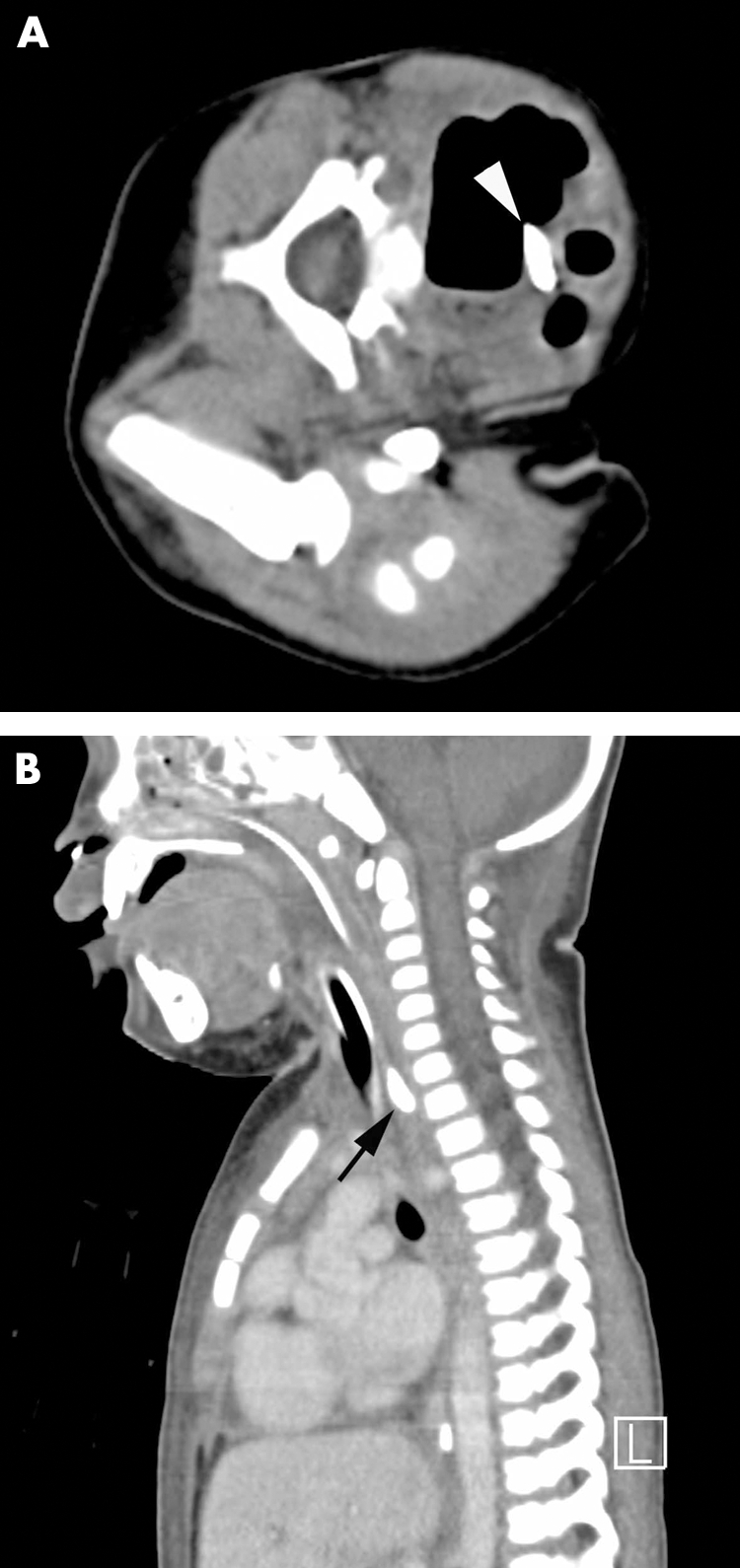
Figure 1 (A) Axial view of unenhanced CT with child lying on left side. Arrowed foreign body is seen lodged in anterior wall of upper oesophagus. The oesophagus is dilated with fluid level evident. (B) Sagittal view of enhanced CT showing foreign body in retropharynx.
Antimicrobial cover was initially changed empirically to clindamycin and gentamycin. After isolation of Escherichia coli and Candida spp. from the abscess fluid, treatment was changed to ciprofloxacin and fluconazole for a 6 weeks.
The patient remained febrile and a further CT scan 3 days later revealed a 15 mm glass foreign body in the retropharynx (fig 1B); however, its precise location could not be pinpointed. Endoscopy identified a perforation of the left piriform fossa and a large piece of glass, which was removed from the hypopharynx.
The patient made a gradual recovery, complicated by an air and saliva leak through the neck wound. Mechanical ventilation was slowly weaned. Extubation was unsuccessful on the first attempt due to upper airway obstruction and copious secretions. A final CT scan showed no further abscess collection. She was successfully extubated after 16 days on PICU and discharged to the ward.
Enteral feeds, initially withheld post‐operatively, were started once a Replogle catheter and nasogastric tube were inserted under direct vision. Unfortunately, the nasogastric tube became displaced, so a nasojejunal feeding tube was passed under image intensifier guidance.
The child had a barium swallow and a test feed, neither of which showed a leak, 37 days after ingesting the piece of glass. She was started on a soft oral diet. She was also noted to have regression of milestones, being unable to sit up or support herself. She was discharged back to the referring hospital a week later. Six months following the incident, she has made a complete recovery.
DISCUSSION
Retropharyngeal abscess and mediastinitis are serious, well documented complications of foreign body ingestion.1,2,3 Early diagnosis of foreign body ingestion may not necessarily prevent progression to deep neck space infection; however, early recognition and removal, and commencement of appropriate therapy may help reduce the associated morbidity.
Unwitnessed foreign body ingestion always poses a difficult diagnostic problem in the pre‐verbal child. Indeed, in a child presenting with ENT signs and symptoms, a history of foreign body ingestion must be taken very seriously. In this instance, the diagnosis was made more difficult because a chest radiograph did not reveal the foreign body. It is of note that glass foreign bodies cannot always be seen on radiographs.4 A lateral neck radiograph is a good indicator of retropharyngeal swelling1,2,4 in the area where this foreign body was lodged, and might have been helpful in establishing the diagnosis sooner. As demonstrated in this instance, ultrasound scanning has been shown to be useful in the diagnosis of retropharyngeal abscess.5,6
It is clear that in the assessment of foreign body ingestion, a high index of suspicion is necessary as a delayed diagnosis can have devastating consequences. The history is very important. It must also be borne in mind that not all foreign bodies, including glass, are readily visualised on plain radiographs, and that lateral neck radiograph and neck ultrasound scan are useful imaging techniques in the diagnosis of retropharyngeal swelling and foreign body ingestion.
Abbreviations
TPN - total parenteral nutrition
ENT - ear, nose, and throat, PICU, paediatric intensive care unit
Footnotes
Competing interests: none declared
References
- 1.Coulthard M, Isaacs D. Retropharyngeal abscess. Arch Dis Child 1991661227–1230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Khan J. Retropharyngeal abscess. 2004. www.emedicine.com/emerg/topic506.htm
- 3.Gidley P W, Ghorayeb B Y, Stiernberg C M. Contemporary management of deep neck space infections. Otolaryngol Head Neck Surg 199711616–22. [DOI] [PubMed] [Google Scholar]
- 4.Cheng W, Tam P K. Foreign body ingestion in children: experience in 1265 cases. J Paediatr Surg 1999341472–1476. [DOI] [PubMed] [Google Scholar]
- 5.Glasier C M.et al CT and ultrasound imaging of retropharyngeal abscesses in children. Am J Neuroradiol 1992131191–1195. [PMC free article] [PubMed] [Google Scholar]
- 6.Levy A D, Harcke H T. Handheld ultrasound device for detection of non‐opaque and semi‐opaque foreign bodies in soft tissues. J Clin Ultrasound 200331183–188. [DOI] [PubMed] [Google Scholar]